In a previous post, I discussed transfusion training for hematology fellows and general pathology residents. I have no expectations that most of them have any interest in the field so I suggested concentrating on the interpretation of the direct antiglobulin test DAT and turn-around-times for services.
In contrast, the transfusion medicine physician in-training needs to understand in detail all processes, donor and patient—especially test interpretation so that he/she can make medical decisions and variances.
During my training, I was fortunate to be in a residency training program that also had an American Specialist-in-Blood Bank SBB training program. To a large extent, I attended the SBB program and even worked on the “wet” specimens.
I had no delusions that I would ever function as technologist or SBB in the blood bank. However, that extended blood bank training has made me the physician I am. I can correlate advanced, even reference, procedures to my medical knowledge and thus provide a unique offering. In contrast, even the SBB is not a physician and cannot make the medical correlations. Recently, I was flattered at an AABB meeting when the speaker thought that I was an SBB.
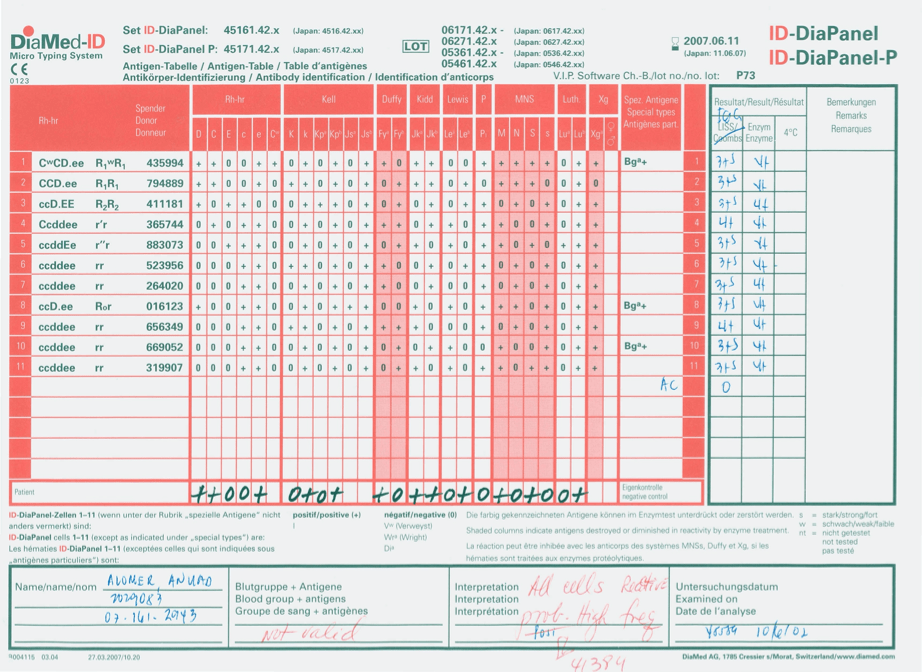
In certain regions where reference immunohematology laboratories and SBBs or equivalent are rare, the transfusion medicine should have sufficient technical background to help fill this gap. In my practice, I review all antibody and DAT workups and make interpretative comments for the physicians and nursing staff. These comments are entered into the blood bank computer system.
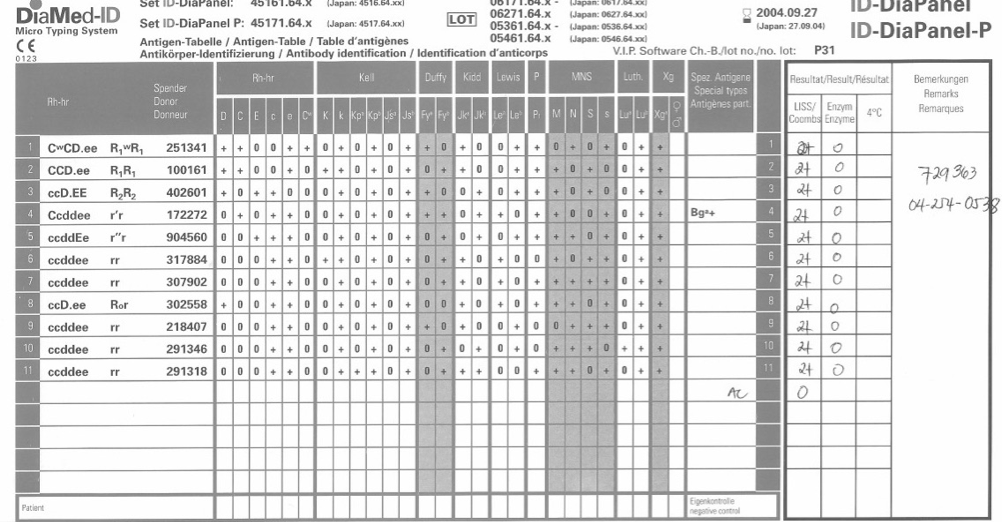
I personally tutor the trainees and make certain that they understand potentially dangerous patterns such as antibodies to high-incidence antigens, significance of the autocontrol in panreactivity, and assessing for fatal acute transfusion reactions—both hemolytic and non-hemolytic.
It also helps when I can discuss with my technical staff my interpretations and choices for clinical management. They get a better idea how important their work is for patient care and understand how any errors may adversely affect the patient.
In regions where there are good immunohematology reference laboratories, some of this may be less necessary. I lament that transfusion medicine physicians may not maintain these skills and must rely on others to their detriment. Even if one is comfortable with this, the physician is still ultimately responsible for making the clinical decision.