This is a teaching case presented to the Medical and Nursing staff at one of my previous affiliations.
Medinfo Hematos IIG software is rules-based so the institution may set its own custom rules for all processes. One chooses a framework and then adds any additional rules it needs for optimization. Turnkey systems do not offer this flexibility.
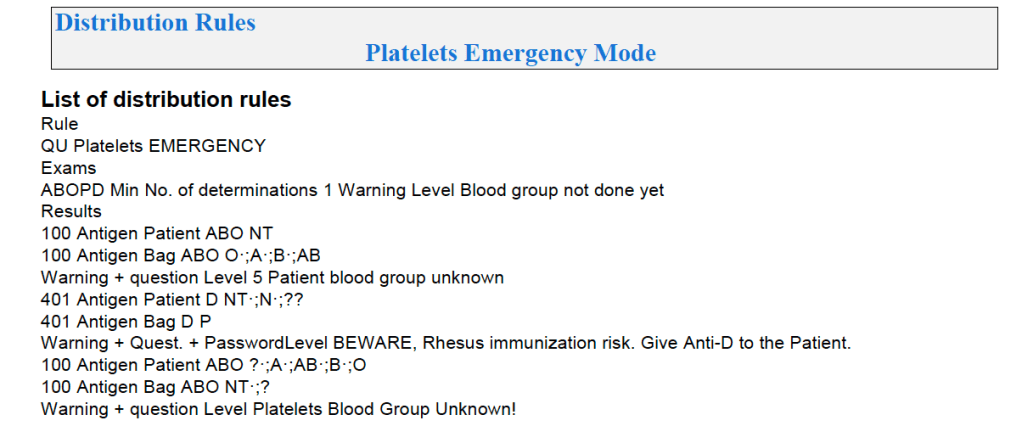
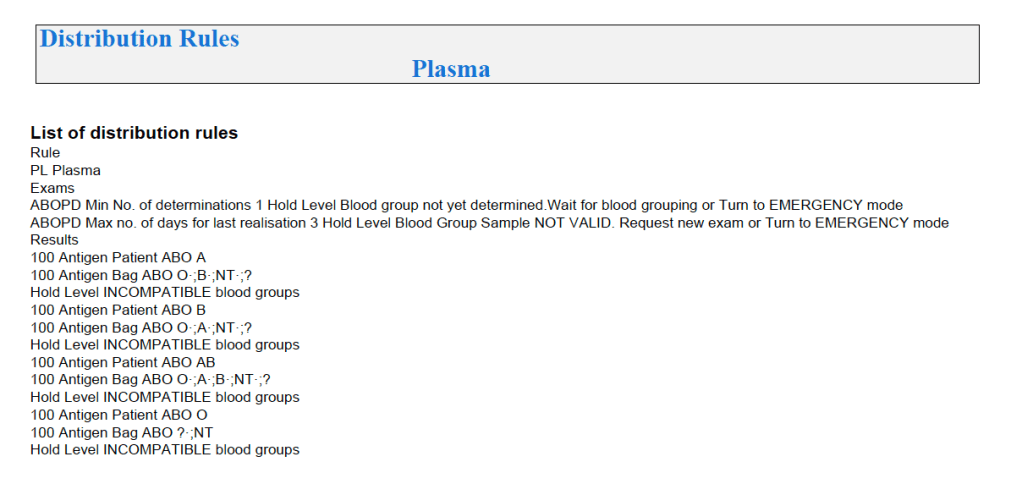
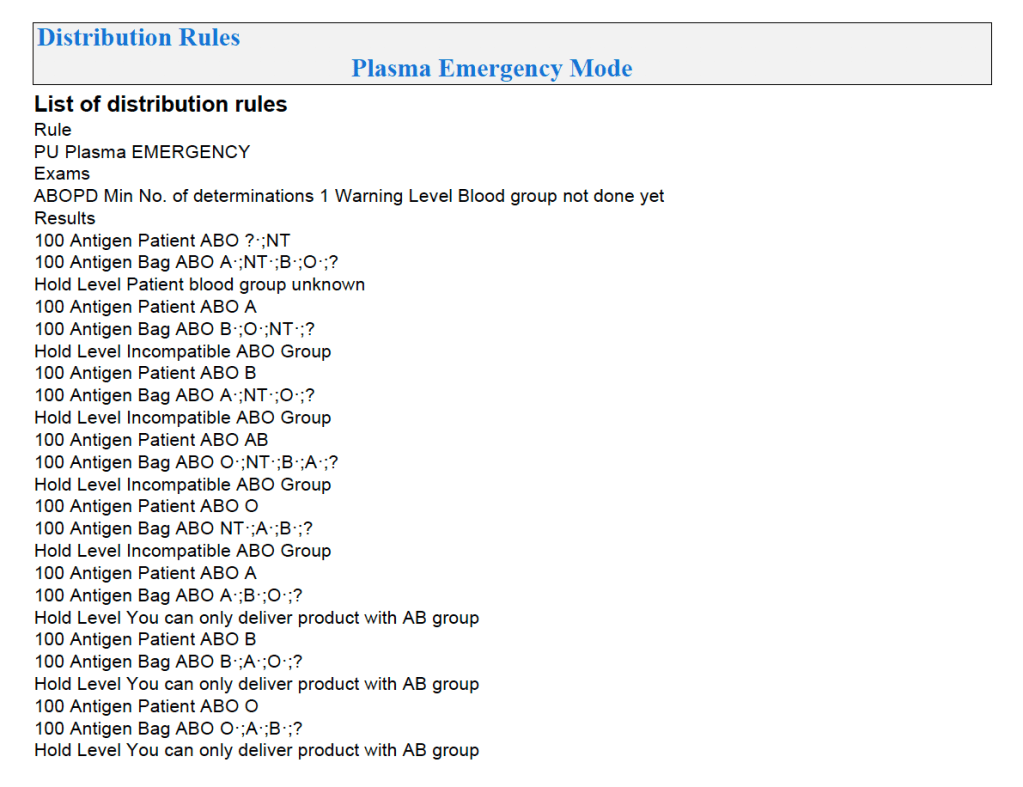
The rules for platelet and plasma components are much simpler than those for RBCs since usually we only consider ABO type. There are two modes: regular and emergency, the latter applying if not all the patient testing (including historical checking) is available. The components, on the other hand, must meet all criteria before being considered for patient use.
Please note that any donor with antibodies is automatically excluded from plasma and platelet production based on our donor testing criteria.
Example rules for plasma follow:
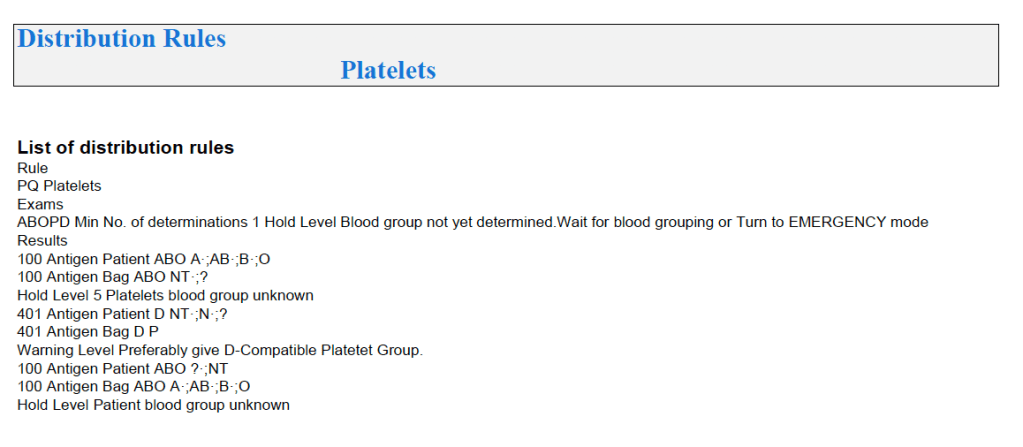
For platelets, note that for adults and anyone else >= 20 kg, I gave any type of platelet pool or plateletpheresis component without regard to ABO matching. With our production method, I did not give Rh immunoprophylaxis to females of child-bearing age receiving platelets from D-positive donors based on our clean (essentially RBC-free) Reveos automated production process.
For platelets, there were also different allocation rules for regular and emergency mode:
Similarly, allocation rules for granulocytes, etc. can be made and enforced by the software. Low-B-titer group A universal plasma would also be easy to implement.
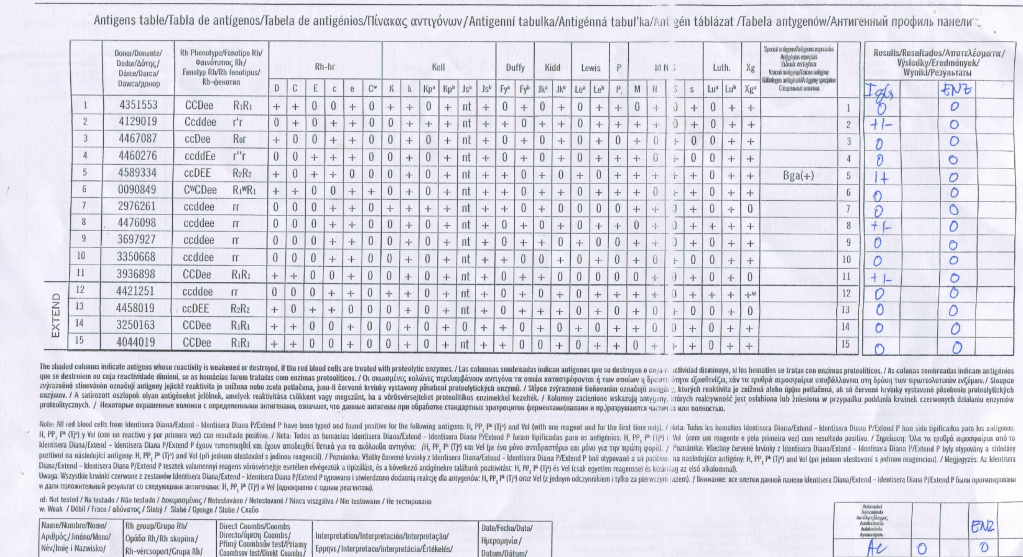
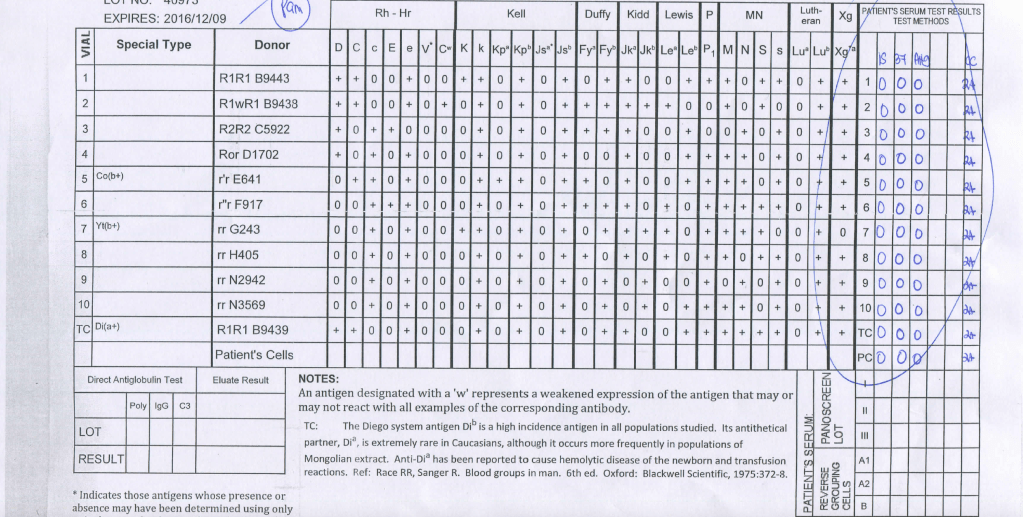
In my Middle Eastern experience, I have found antibody panels from a certain manufacturer show a lot of weak, nonspecific reactivity which disappears with another manufacturer’s panels, particularly when gamma-heavy-chain-specific reagents are used:
Normally, in my protocols, the first encounter in this situation, I would do extended RBC phenotyping beyond Rh and Kell systems as well.
In my experience, the nonspecific reactions detected are not clinically significant and they may be ignored if the conditions of the following algorithm is used:
What do you do when you encounter this is in your laboratory? Please share your thoughts.
Manufacturer 1’s Panel:
Manufacturer 2’s Panel:
Note: This is an update of a previous post.
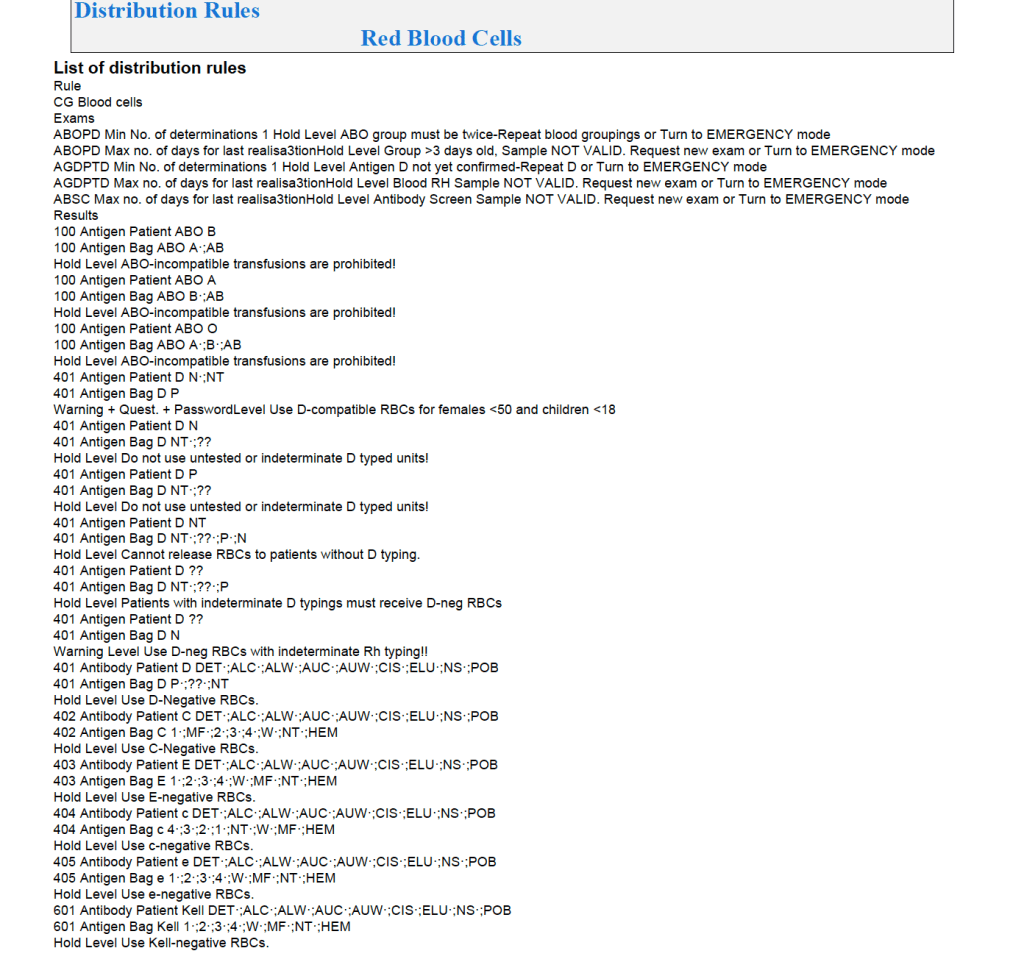
In the previous posts I outlined how Medinfo handled antibody screening and identification. This post reviews how antigen matching is used based on these results.
There are two modes, regular and emergency. If the patient has not had at least two ABO/D determinations and/or does not have a recent antibody screen within the past 3 days, then emergency mode must be selected with its own rules. Otherwise, the regular mode applies.
Regular Mode:
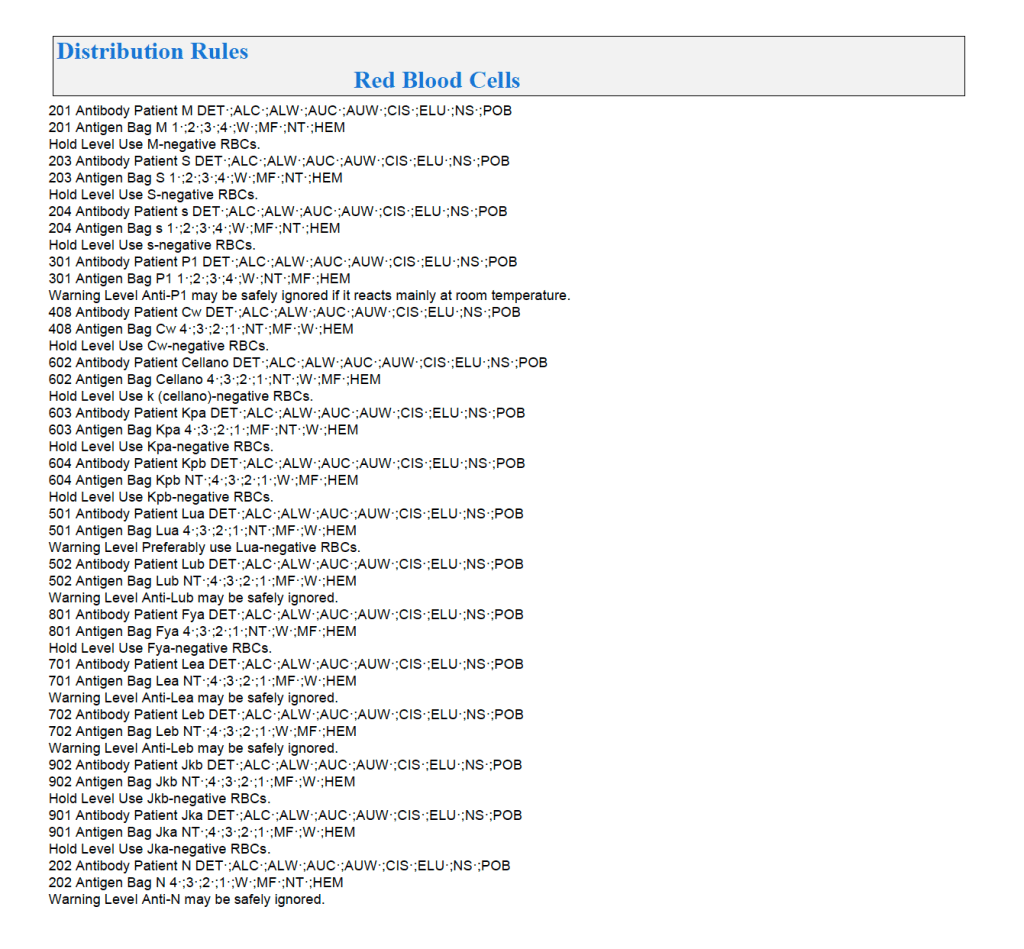
In general, if there is a clinically significant antibody, an RBC unit which has not been matched for the corresponding antigen or has the corresponding antigen cannot be routinely selected. However there is a hierarchy here also:
Examples of Regular Mode rules follow (these are not the complete lists but just provided to show the complexity of the process).
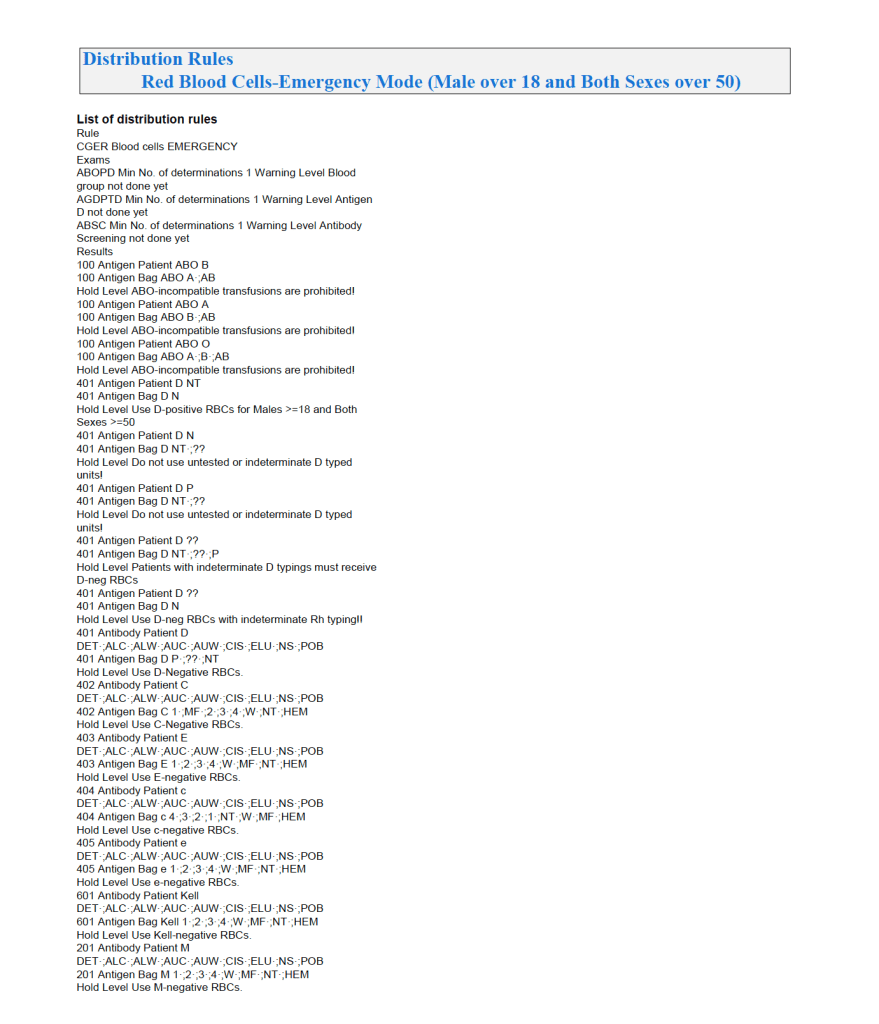
Emergency Mode:
This is much more restricted for selection of ABO/D and other antigen typings. An example follows:
If low-titer group O whole blood is available, then a specific rule must be added to both regular and emergency mode to allow this to be given to any ABO type except Bombay.
