This presentation was originally given to third-year medical students at NGHA-Riyadh as their first lecture, Introduction to Transfusion Medicine. It has been updated for new component types and will be presented in multiple parts.
This presentation was originally given to third-year medical students at NGHA-Riyadh as their first lecture, Introduction to Transfusion Medicine. It has been updated for new component types and will be presented in multiple parts.
This presentation was originally given to third-year medical students at NGHA-Riyadh as their first lecture, Introduction to Transfusion Medicine. It has been updated for new component types and will be presented in multiple parts.
End Part 1.
The AABB just updated its Ebola Toolkit and made proposed changes to the Uniform Donor Questionnaire UDQ to reflect this. Up to five (5) questions should be included in your questionnaire. What question(s) to use depends on:
| Yes | No | |
| Ebola Question 1: Have you ever had Ebola virus disease or infection? | q | q |
| Ebola Question 2: In the past 8 weeks, have you lived in, or traveled to, a country with widespread transmission of Ebola virus disease or infection? (Review list of affected areas, as classified by CDC) * | q | q |
| Ebola Question 3: In the past 8 weeks, have you had sexual contact with a person who has EVER had Ebola virus disease or infection? | q | q |
| Ebola Question 4: In the past 8 weeks, have you had direct exposure to body fluids (blood, urine, stool, saliva, semen, vaginal fluids or vomit) from a person who may have Ebola virus disease or infection, including a person under investigation? | q | q |
| Ebola Question 5: In the past 8 weeks, have you been notified by a public health authority that you may have been exposed to a person with Ebola virus disease or infection? | q | q |
If the response to question #1 is YES, then the donor is indefinitely deferred.
For questions 2-5, there is an 8-week deferral.
In areas with no widespread transmission, self-deferral of donors with a history of Ebola infection should be adequate, only question #1 is required. If there is widespread transmission, questions #2-5 should be added. Four (4) weeks after widespread transmission stops, revert back to using question #1 only.
These can be easily added to the donor questionnaire in Medinfo blood donor module.
References:
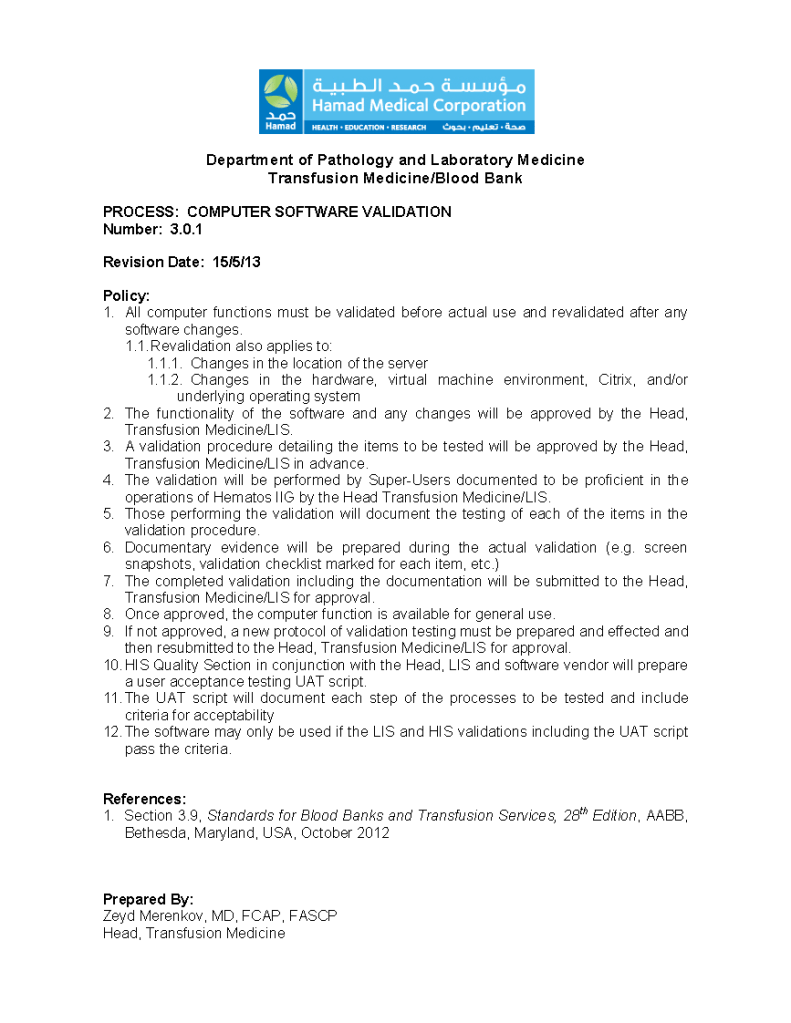
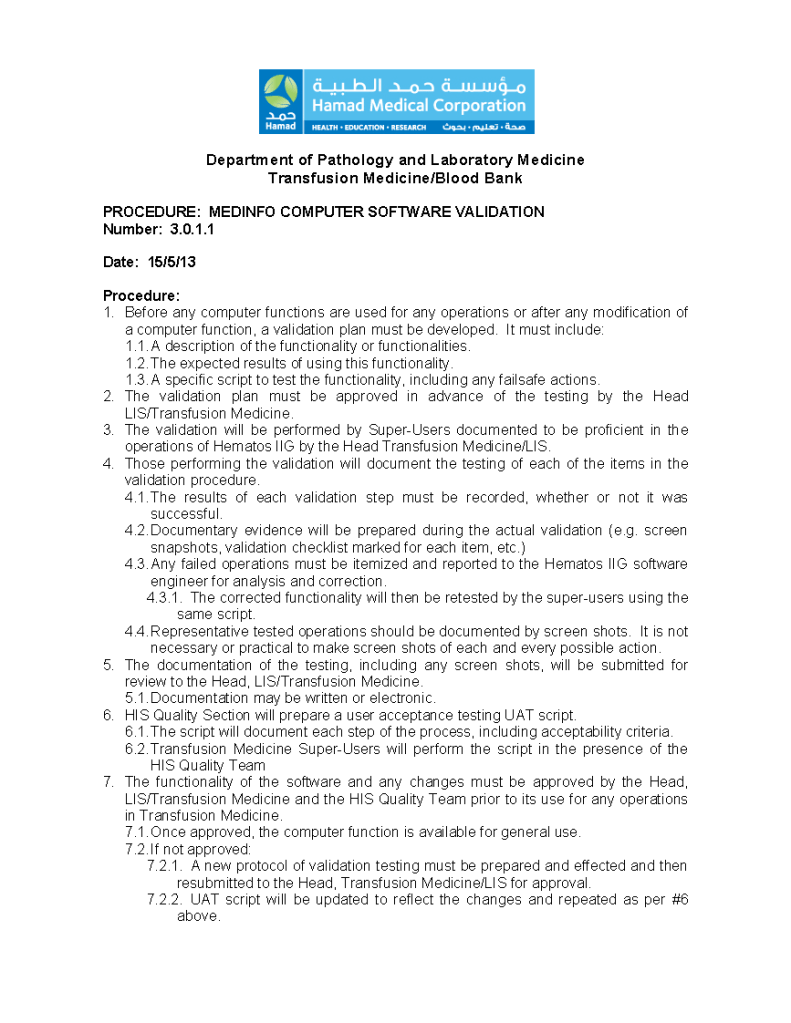
It is now almost eight years since HMC Doha went live with Medinfo donor and patient modules. These are the base documents (policy, process, and procedure) to perform those validations.
These are the answers to the previous post.
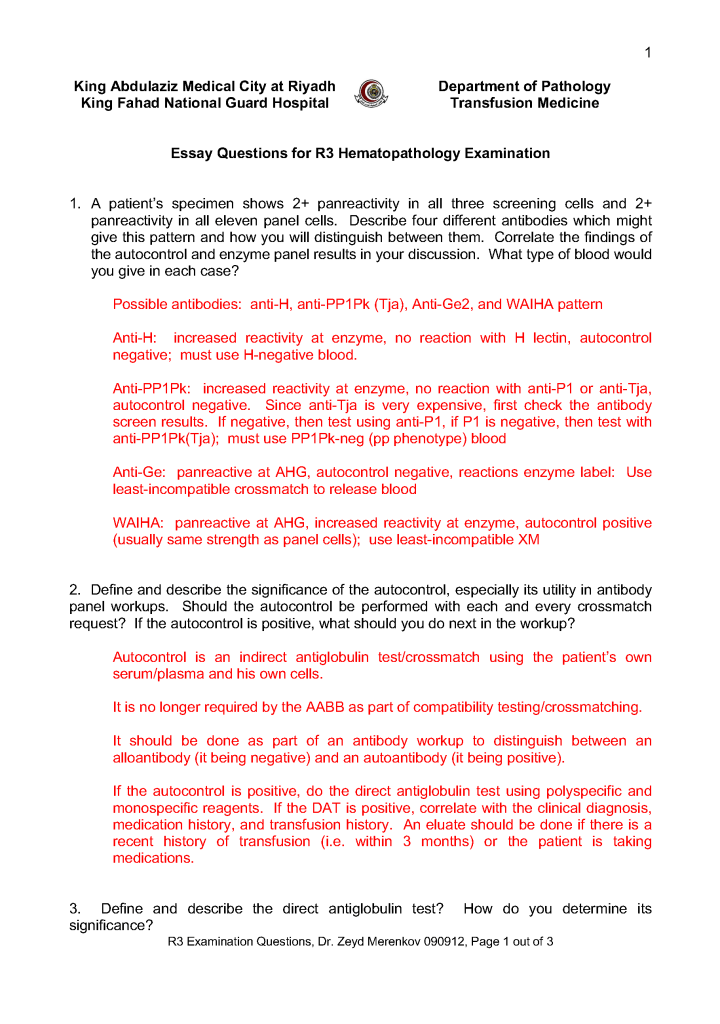
This is the third-year hematology fellow examination I prepared for NGHA Riyadh:
This is a post of an old teaching presentation for pathology residents, hematology fellows, and transfusion medicine fellows from my time at NGHA-Riyadh.
The World Health Organization WHO just released a Key Facts document on HTLV-1 infection (references below) as follow up to their February, 2020 Technical Report. Here are some highlights for blood bankers:
HTLV-1 is efficiently transmitted by blood transfusion with a rate of 28-63% from a donor with HTLV-1 and up to 87% from a tissue transplant.
Testing can be made more complicated due to the length of time between contracting the virus andthe seroconversion required for the virus to appear on tests. This period has been reported to be aslong as 65 days.
Mandatory HTLV-1 antibody screening of all blood donations has been implemented in 23 countries.
Because HTLV-1 is almost always cell associated, leukoreduction may be as effective as blood donation screening in preventing transmission.
Following current practices, screening tests for HTLV-1 should be followed by confirmatory tests for the diagnosis of HTLV-1. Most screening tests use immunoassays, which rely on detecting anti-HTLV-1 antibodies. Commonly used confirmatory tests detect antibody responses to specific HTLV-1antigens. Test types include the Western Blot, radioimmunoprecipitation assay (RIA) and linear immunoblot assay LIA. However, the Western Blot test has been found to give unreliable results. Several studies have proposed transitioning from using Western Blot for confirmation in routine testing to using line immunoassay or NAT.
In my laboratory in Qatar, we detected approximately 8-10 cases of infection per year on a donor testing base of 36,000 for the year 2019. These were confirmed cases by LIA. In addition to the universal leukodepletion of all components to the CE-mandated level of < 1E6, we also pathogen-inactivated platelet components and plasma.
References:
This is a reprint of a previous post.
This is an updated version of a previous post.