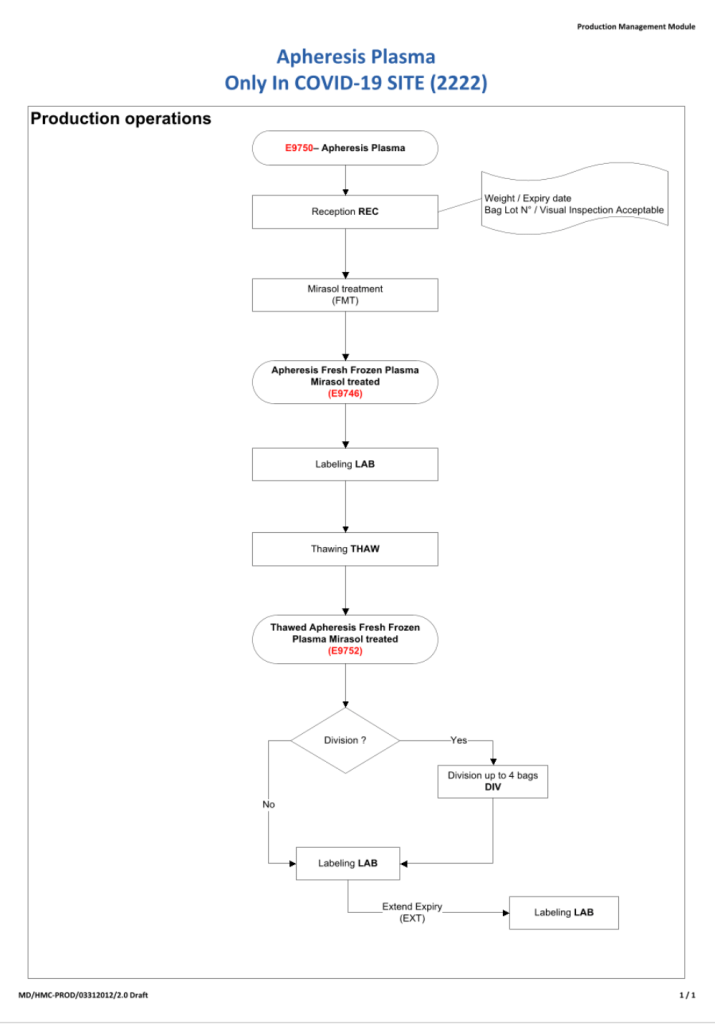
It now has been over eight 8 months since I prepared the CCP workflow in Medinfo. It was built on the framework of the manual CCP process including donor prescreening with an abbreviated donor questionnaire. It was really quite simple and used the donor and patient modules to create quarantine areas for donor screening, collection, processing, and hospital patient blood bank release.
Here are my current comments on the process:
Donor Qualification:
I would still exclude malaria and HTLV from the donor questionnaire and would update to UDQ 2.1. Since these donors have recovered from a potentially life-threatening illness, I would keep the Hgb threshold at 11 g/dl.
Donor Collection:
In the future, I would consider using one of the soon-to-be-released portable devices that continuously monitor vital signs with pO2 and EKG lead to rule out asymptomatic pulmonary or cardiac problems.
I would also consider using low-ABO-titer, group A, universally to meet the demand for group B and AB patients.
Donor Testing:
There is still no need to segregate and separately test CCP donor specimens from regular blood donor specimens. I would perform SARS-CoV-2 antibody testing and set a threshold for qualifying donors—that threshold will be based on the manufacturer’s recommendations. However, if the treating physician wanted to use a low-titer unit, I would permit this.
Donor Processing:
There is no need to change this from the current processes. Keep the CCP processing separate from the regular operations.
CCP Plasma Release:
I would keep the quarantine release and restrict it to the locations used for treating COVID-19 patients
Medinfo Software Modifications:
I would record the IgG and IgM titers for SARS-CoV-2 antibodies in each donation record. This would include testing and entering the results on donations prior to this testing. ISBT labels should include this antibody titer.
Hospital Information Software Modifications:
Set up restricted CCP ordering for the actual treating physicians only. Also provide the ISBT code and shortened descriptors to it if necessary (certain HIS vendors still cannot read ISBT codes natively).
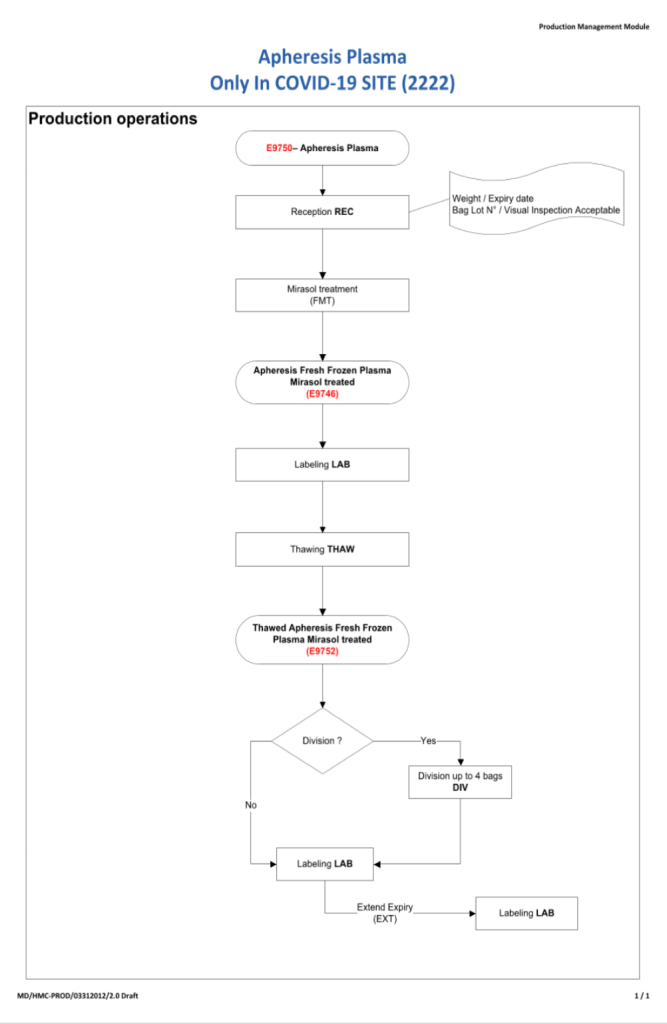
The original CCP workflow is attached for reference.