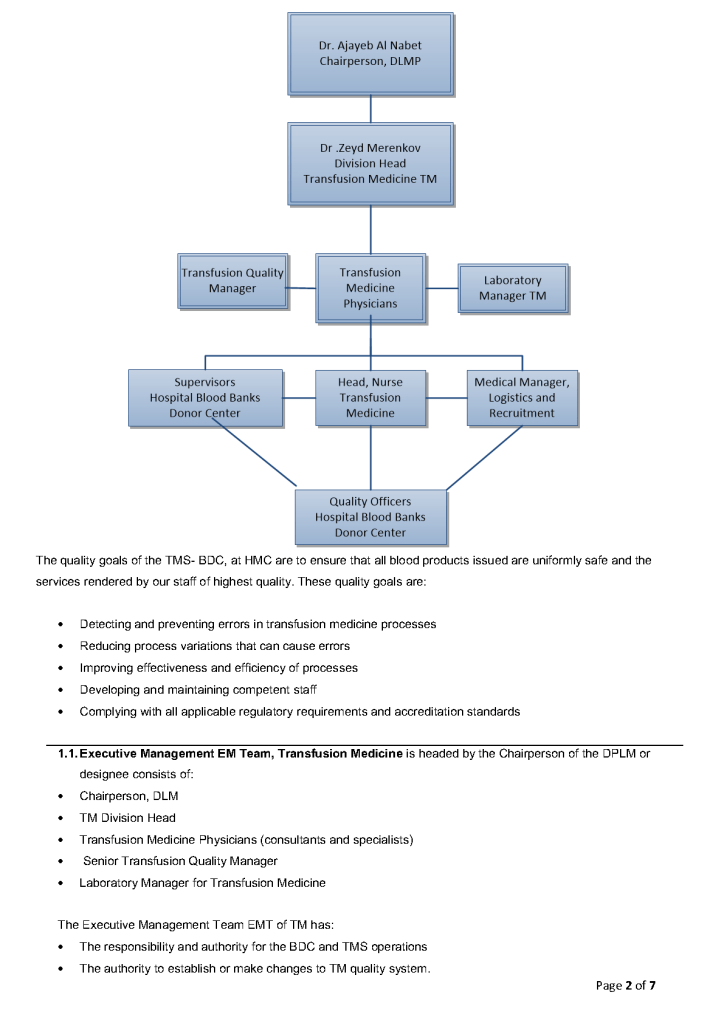
This is a sample quality system plan to comply with AABB and CAP accreditation standards that I used at HMC Doha.
This is the policy I used at HMC Doha for screening donors for this agent.
Principle:
Nipah virus NiV is a paramyxovirus that may cause a fatal encephalitis in infected patients. Transmission to humans may occur after direct contact with infected bats, infected pigs, or from other infected humans. ELISA, NAT, and direct culture may be used for confirmation of diagnosis, but there is no available licensed donor test. The geographical distribution of this virus corresponds generally to the areas of malaria exclusion used for blood donor screening. Most cases are fatal, and survivors may have neurologic sequelae.
The incubation period is 5-14 days with illness presenting 3-14 days of fever, headache, followed by drowsiness, disorientation, and confusion. These findings may progress to coma within 24-48 hours. Some patients also develop a respiratory illness. Latent infections with subsequent reactivation of the virus have occurred months to years after exposure.
Policy:
References:
Nipah Virus Fact Sheet, Center for Disease Control, Atlanta, GA, USA—current edition—attached.
This is an updated version of a previous post.
Principle:
All donor unit mislabeling is potentially life-threatening and must be stringently investigated as soon as possible after the discrepancy is detected. Most importantly, if there is one error, there may be possibly ADDITIONAL donor unit errors (e.g. switch of donor tubes or units, etc.). All donor units processed in the same batch must be also quarantined until the discrepancies are resolved.
Policy Details:
The following steps MUST be performed as soon as possible:
Reference:
Standards for Blood Banks and Transfusion Services, Current Version, AABB, Bethesda, MD, USA
