Skip to content
Open Menu
Blog (Home)
Transfusion Medicine
Blood Bank IT
COVID-19 Plasma CCP
Plasma Fractionation
About me
Work with me
Contact me
Search
Search for:
Close
Dr. Zeyd Merenkov
Transfusion Medicine, Blood Bank IT, Pathogen Inactivation, Plasma Fractionation, COVID-19 Convalescent Plasma Production
Tag:
Donor Collection
Recruitment and Collection
Confidential Unit Exclusion
Image
23rd Jul 2026
25th Jan 2026
drzeyd
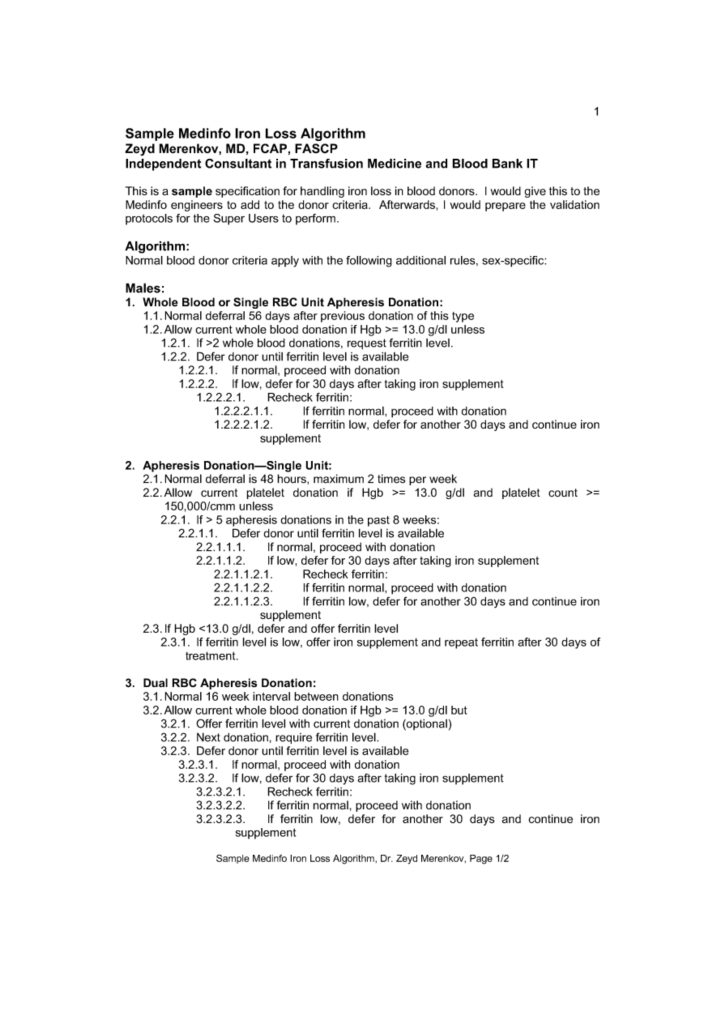
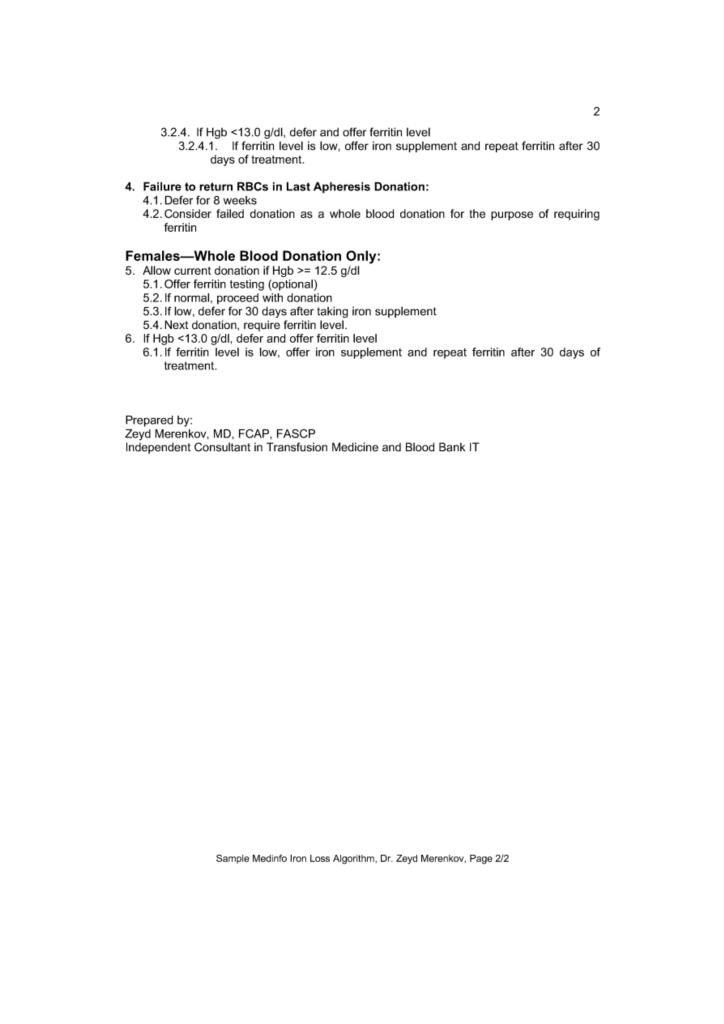
Sample Medinfo Iron Loss Algorithm
21st Jul 2026
23rd Jan 2026
drzeyd
Minimizing Iron Deficiency in Blood Donors
Image
20th Jul 2026
23rd Jan 2026
drzeyd
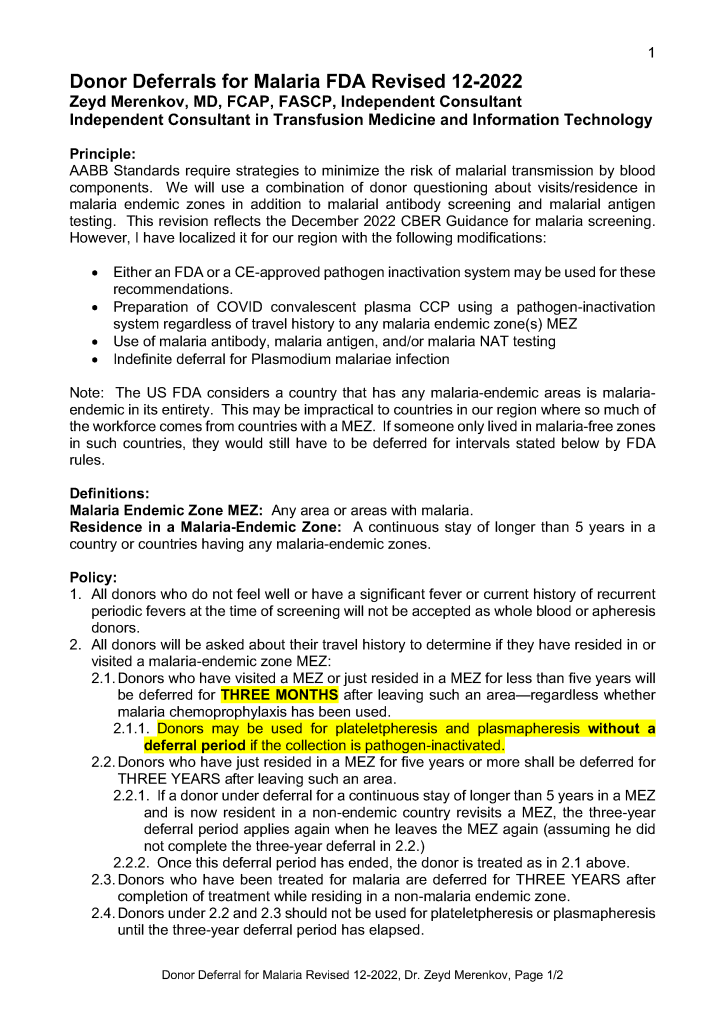
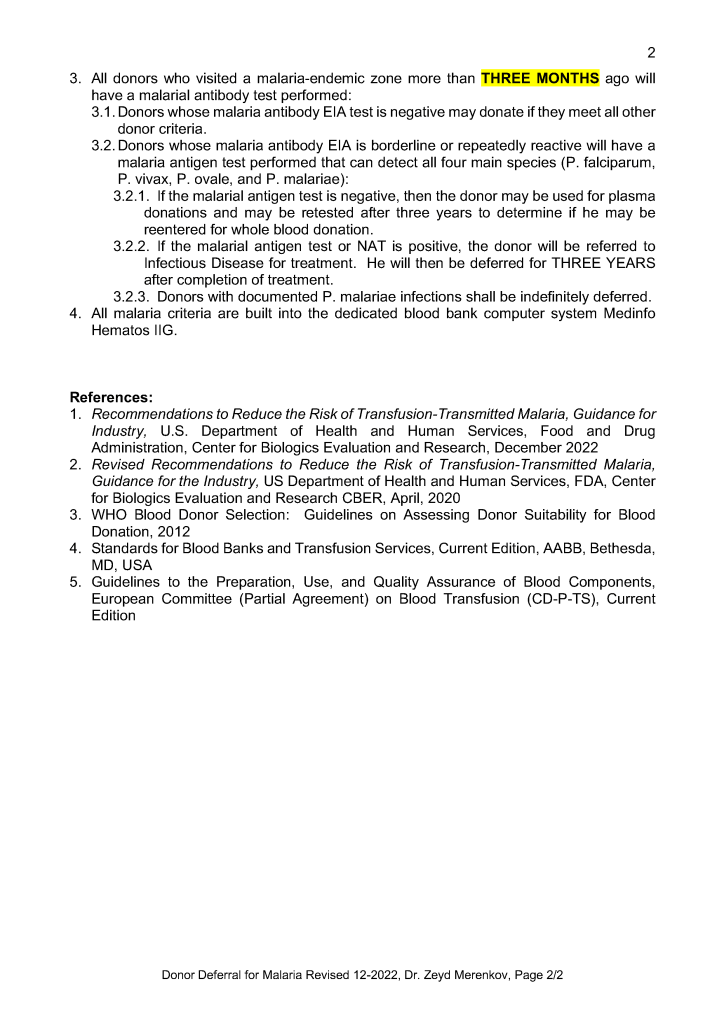
Donor Deferrals for Malaria 2022
18th Jul 2026
21st Jan 2026
drzeyd
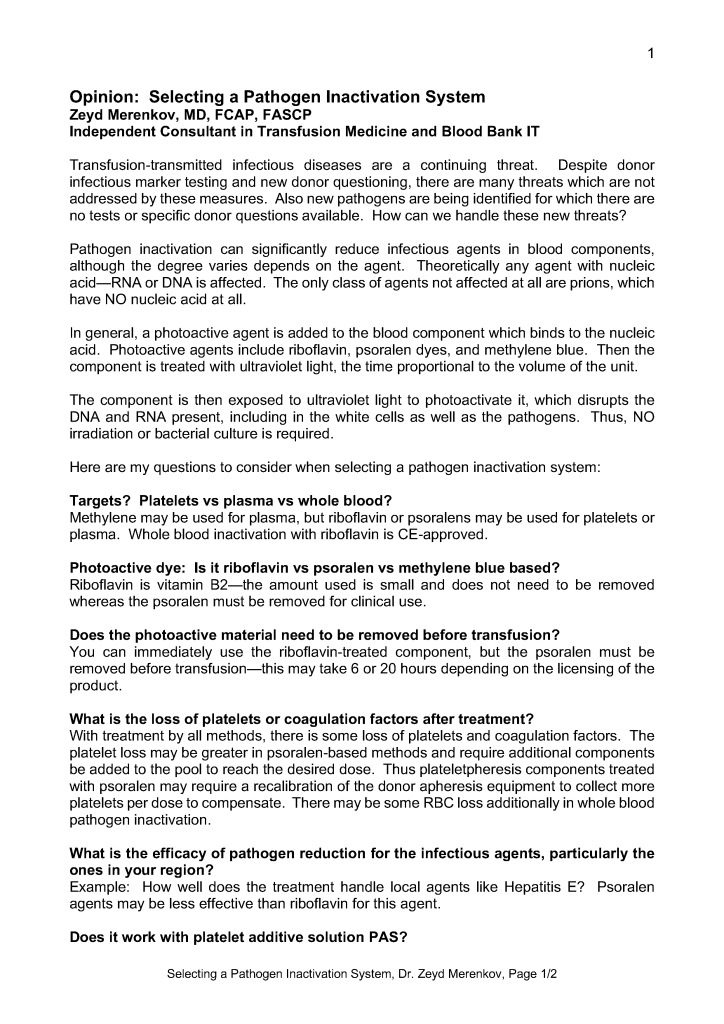
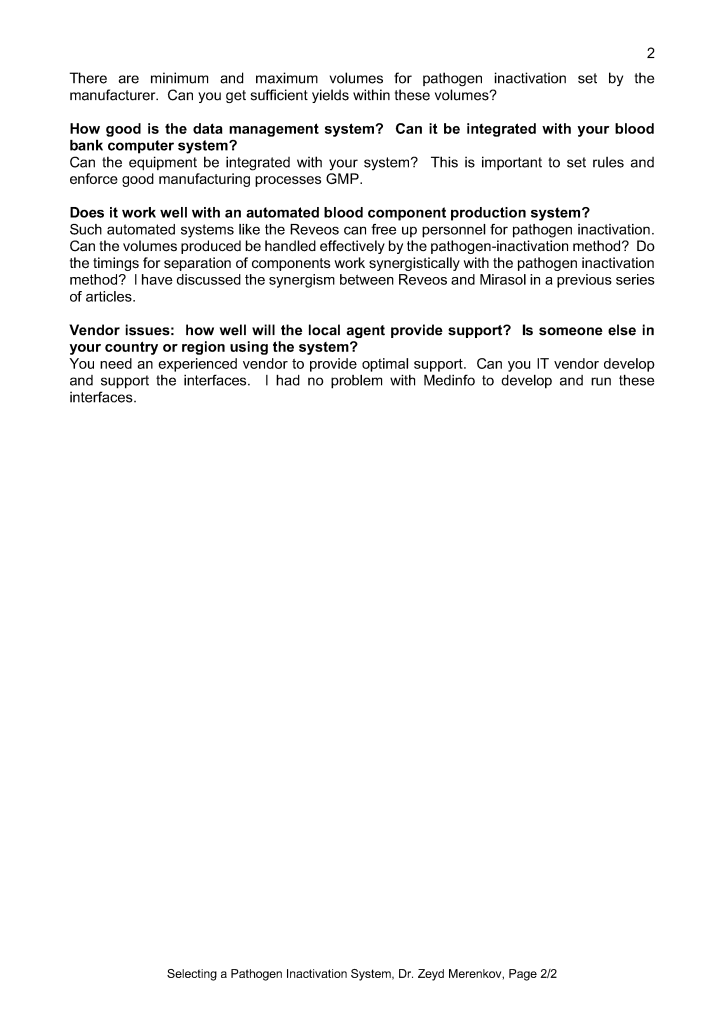
Selecting a Pathogen Inactivation System
15th Jul 2026
17th Jan 2026
drzeyd
Policy: Handling Registration Errors
Image
7th Jul 2026
6th Jan 2026
drzeyd
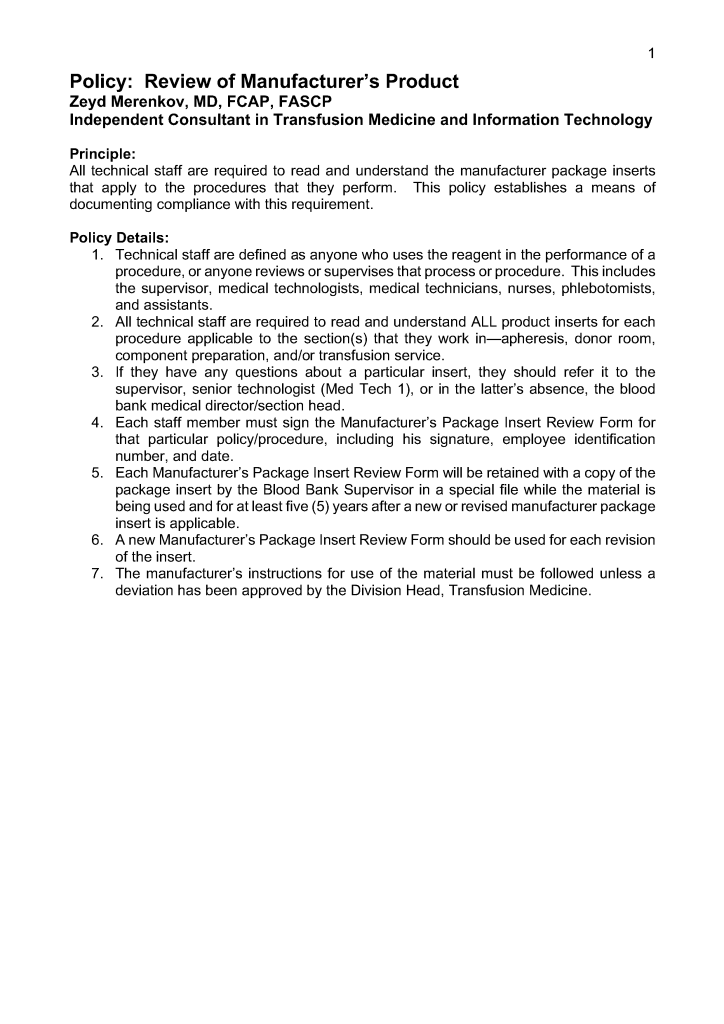
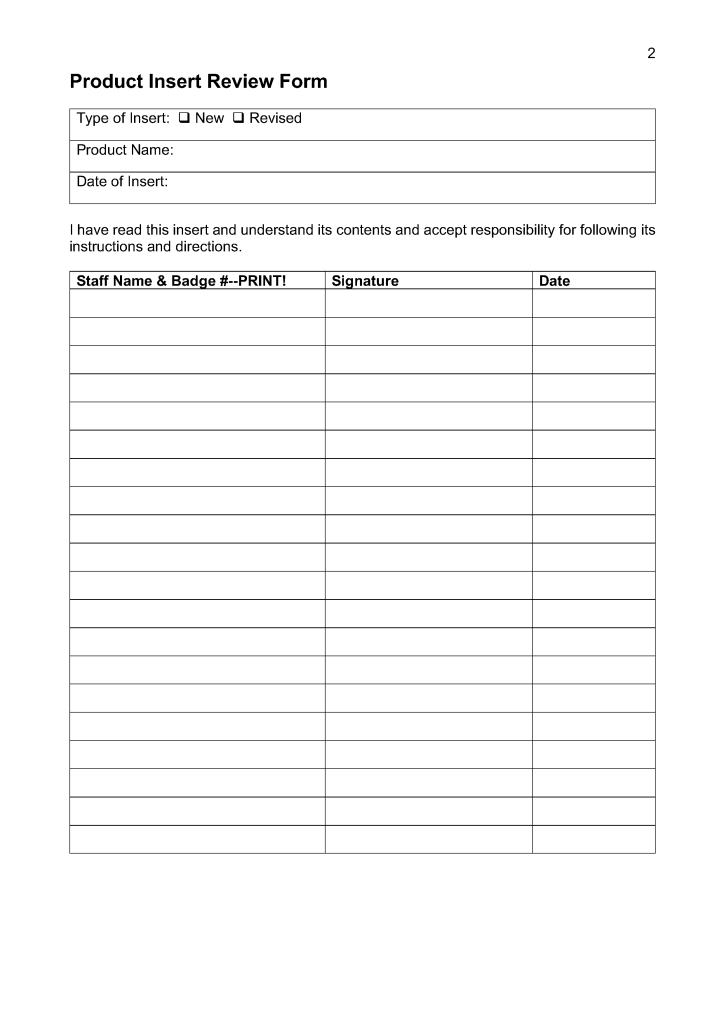
Product Insert Review
3rd Jul 2026
28th Dec 2025
drzeyd
Revised Donor Screening for Ebola
Image
30th Jun 2026
drzeyd
Teaching Medical Students and Residents
Image
28th Jun 2026
24th Dec 2025
drzeyd
Acceptable Donor Identification
Image
24th Jun 2026
21st Dec 2025
drzeyd
Posts navigation
Older Posts
Back to top
Subscribe
Subscribed
Dr. Zeyd Merenkov
Join 41 other subscribers.
Sign me up
Already have a WordPress.com account?
Log in now.
Dr. Zeyd Merenkov
Subscribe
Subscribed
Sign up
Log in
Report this content
View site in Reader
Manage subscriptions
Collapse this bar
Loading Comments...
Write a Comment...
Email (Required)
Name (Required)
Website