Skip to content
Open Menu
Blog (Home)
Transfusion Medicine
Blood Bank IT
COVID-19 Plasma CCP
Plasma Fractionation
About me
Work with me
Contact me
Search
Search for:
Close
Dr. Zeyd Merenkov
Transfusion Medicine, Blood Bank IT, Pathogen Inactivation, Plasma Fractionation, COVID-19 Convalescent Plasma Production
Tag:
Processes and Software Building
Detailed discussion of Medinfo processes for all blood bank donor and patient services
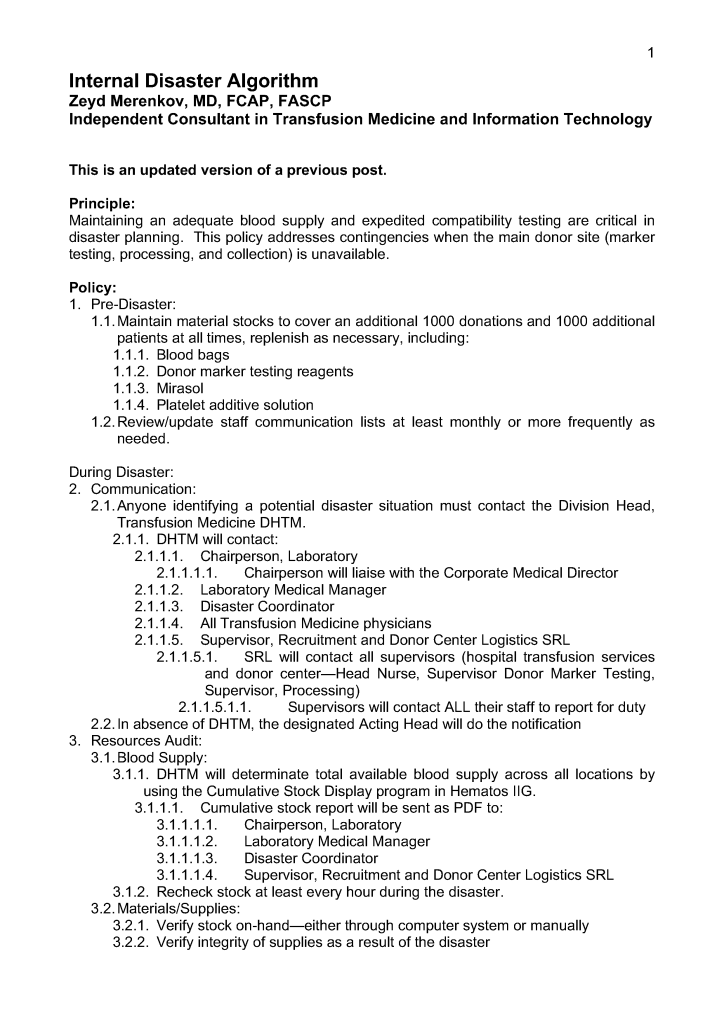
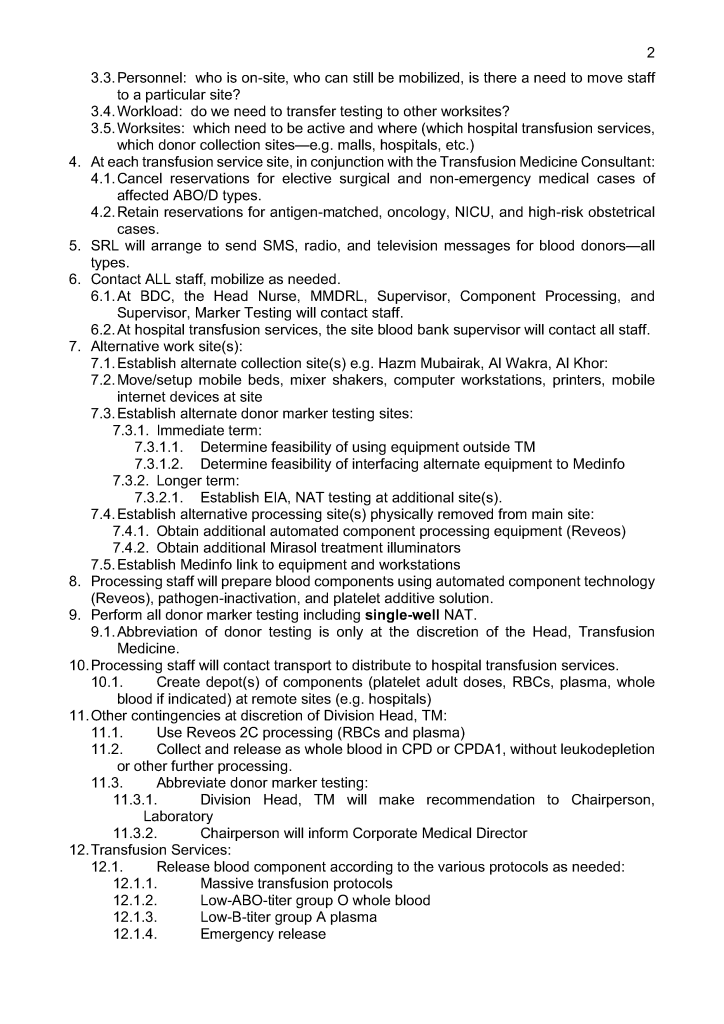
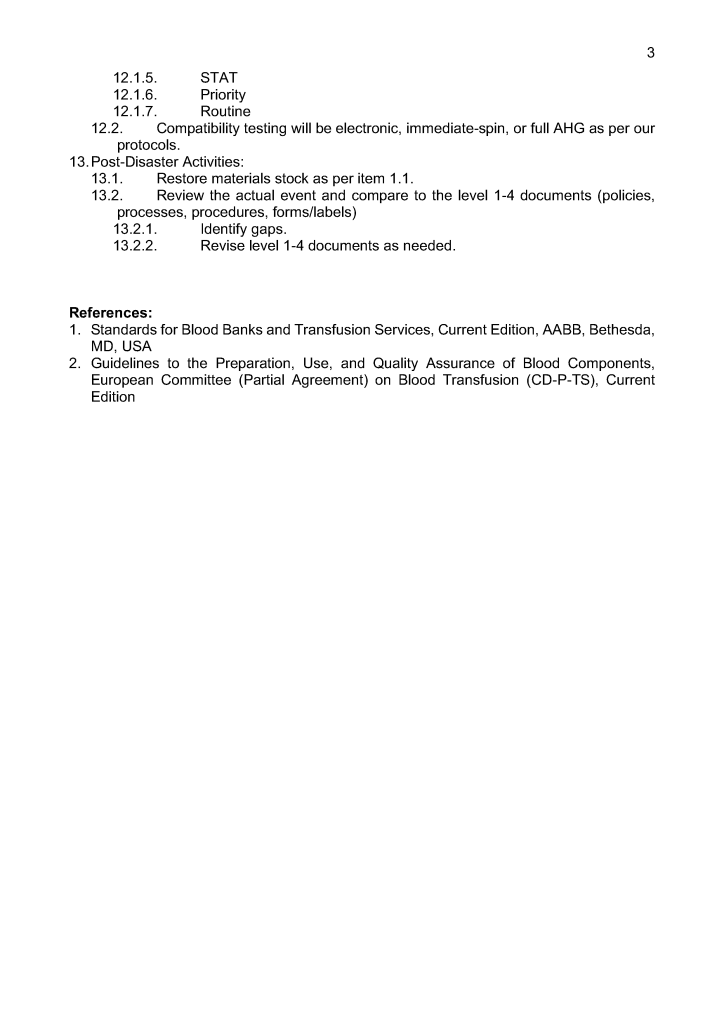
Internal Disaster Algorithm
8th Dec 2021
5th Sep 2021
drzeyd
Policy: Elution Indications
Image
20th Nov 2021
22nd Aug 2021
drzeyd
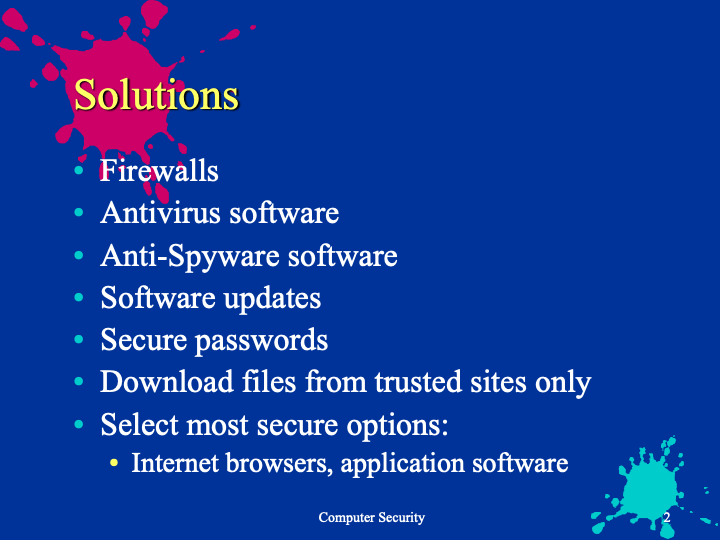
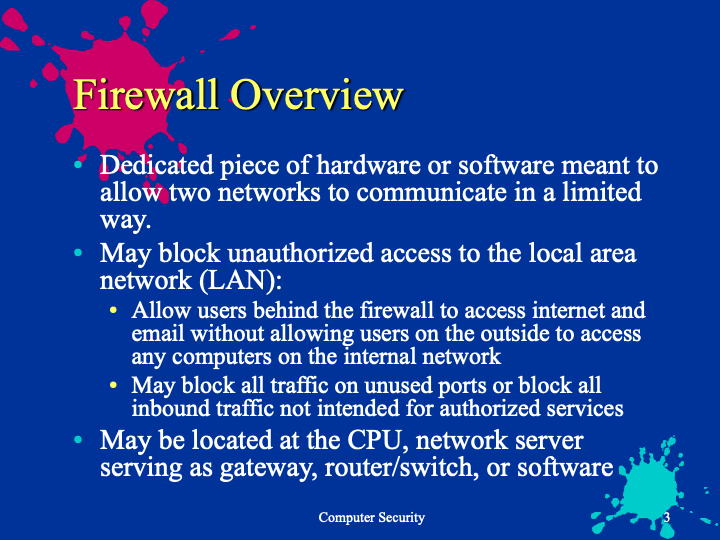
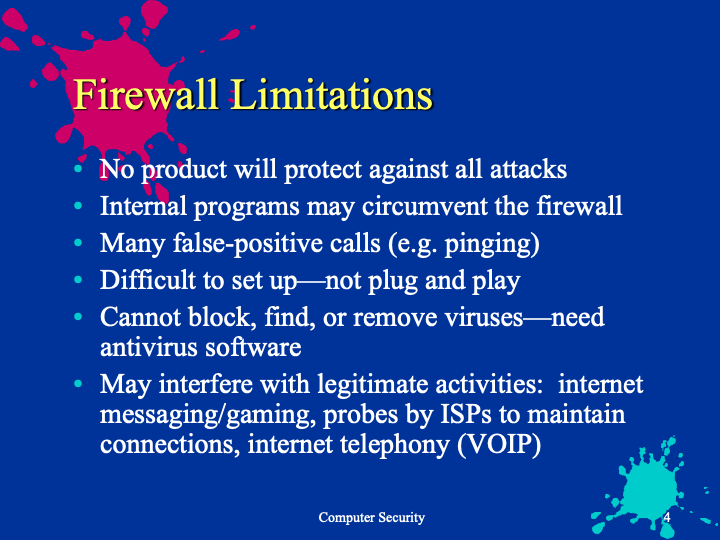
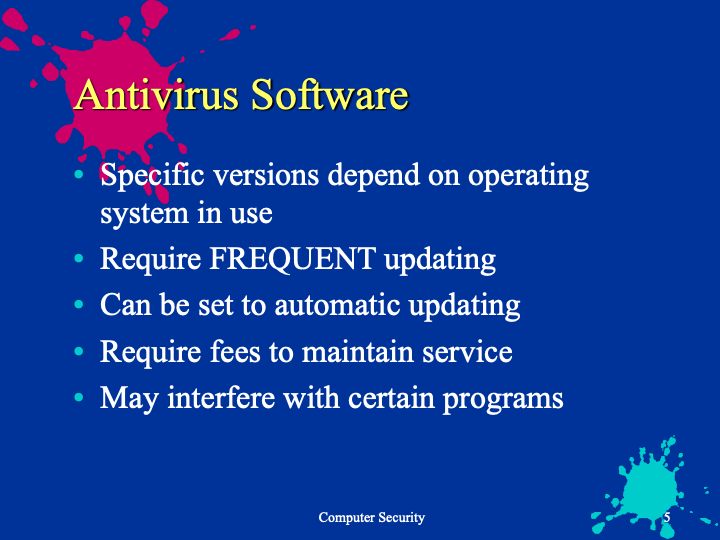
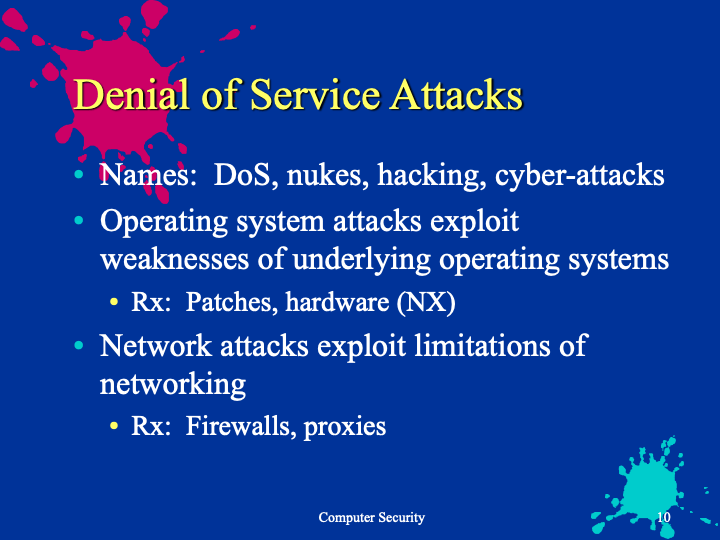
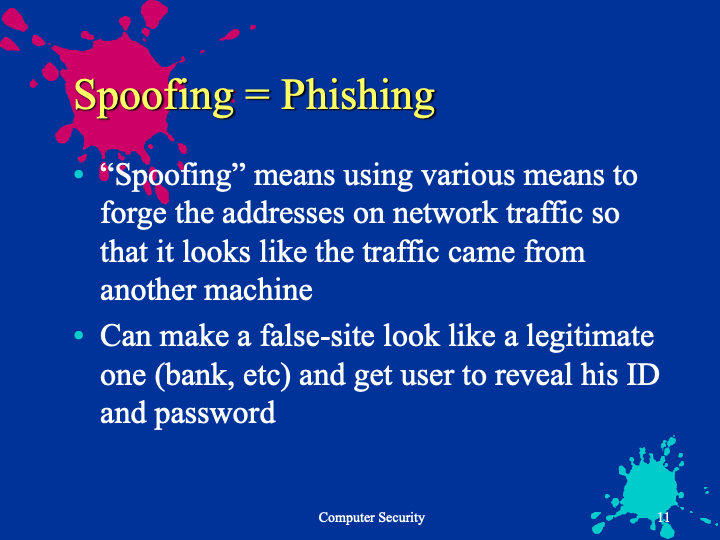
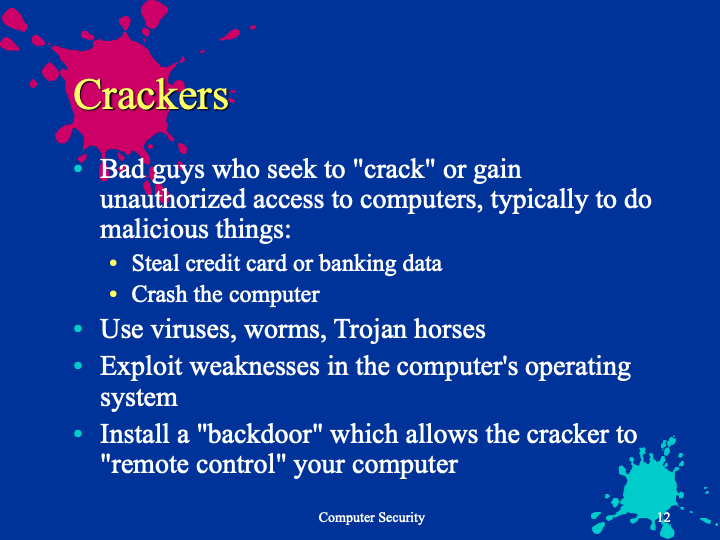
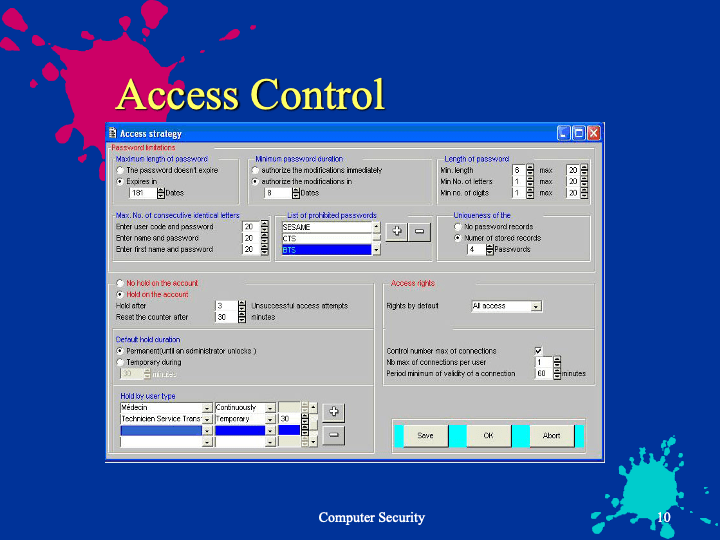
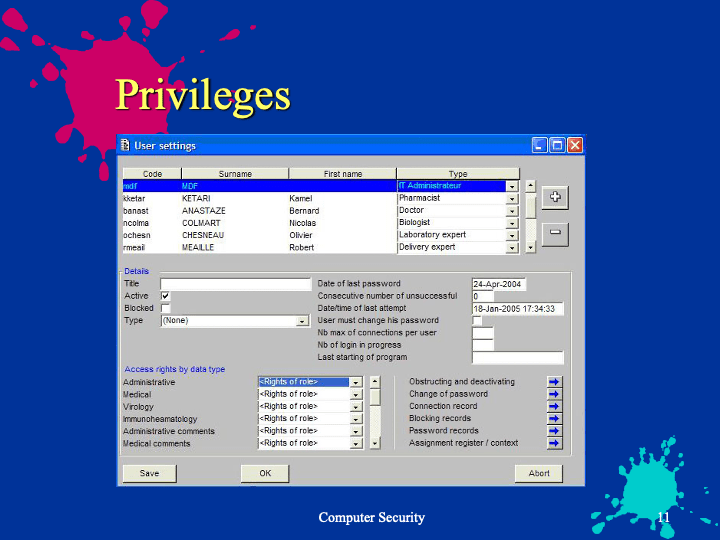
Blood Bank Computer Security 4
19th Nov 2021
21st Aug 2021
drzeyd
Blood Bank Computer Security 3
18th Nov 2021
21st Aug 2021
drzeyd
Blood Bank Computer Security 2
17th Nov 2021
21st Aug 2021
drzeyd
Blood Bank Computer Security 1
16th Nov 2021
21st Aug 2021
drzeyd
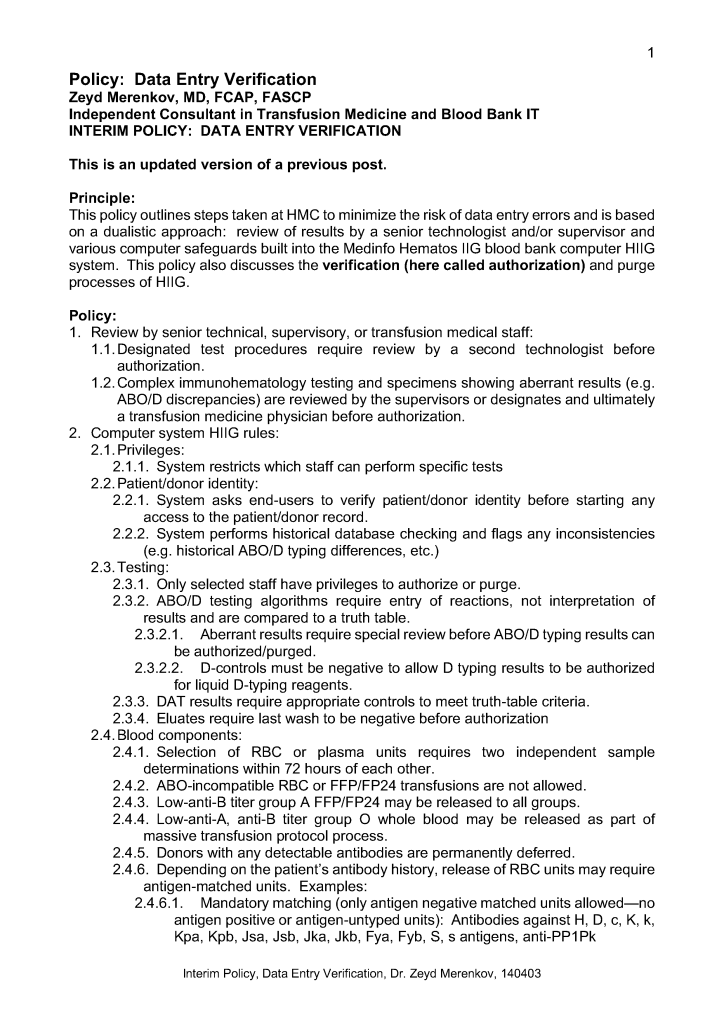
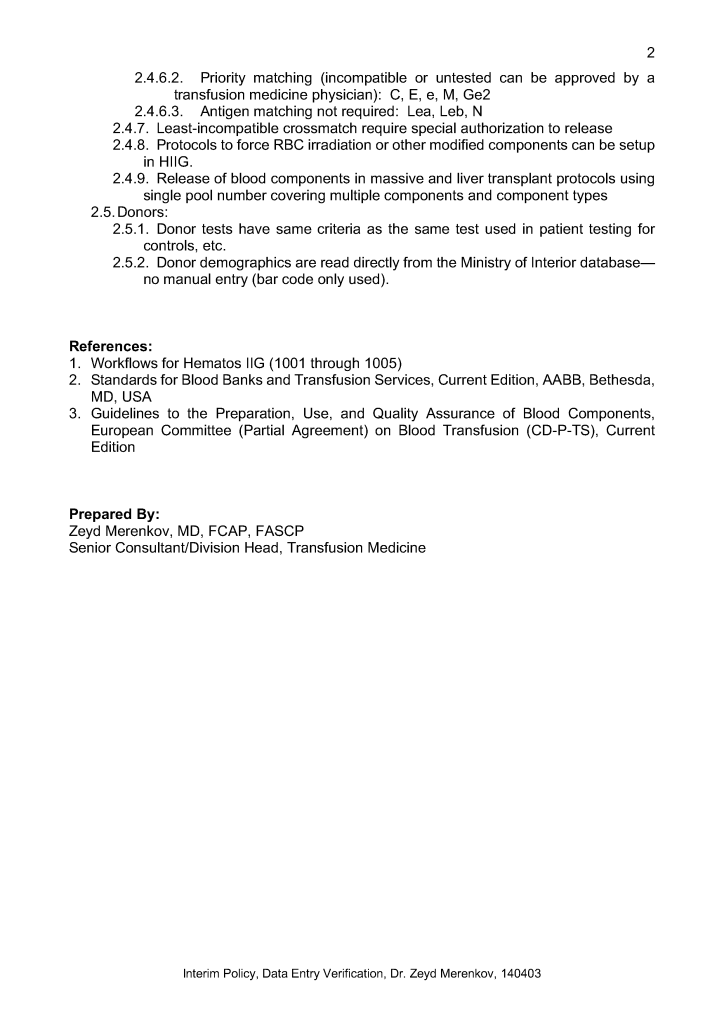
Policy: Data Entry Verification
11th Nov 2021
17th Aug 2021
drzeyd
Policy: Contingency Planning
Image
1st Nov 2021
11th Aug 2021
drzeyd
Business Plan for Medinfo Hematos IIG Downtime
Image
19th Oct 2021
4th Aug 2021
drzeyd
Policy: Blood Supply Quarantine
Image
18th Oct 2021
3rd Aug 2021
drzeyd
Posts navigation
Older Posts
Newer Posts
Back to top
Subscribe
Subscribed
Dr. Zeyd Merenkov
Join 41 other subscribers.
Sign me up
Already have a WordPress.com account?
Log in now.
Dr. Zeyd Merenkov
Subscribe
Subscribed
Sign up
Log in
Report this content
View site in Reader
Manage subscriptions
Collapse this bar
Loading Comments...
Write a Comment...
Email (Required)
Name (Required)
Website