In February 2020, I established COVID-19 plasma collection and distribution for the state of Qatar. Here is a research paper prepared in conjunction with the Qatar Communicable Disease Center about using it for patients there.




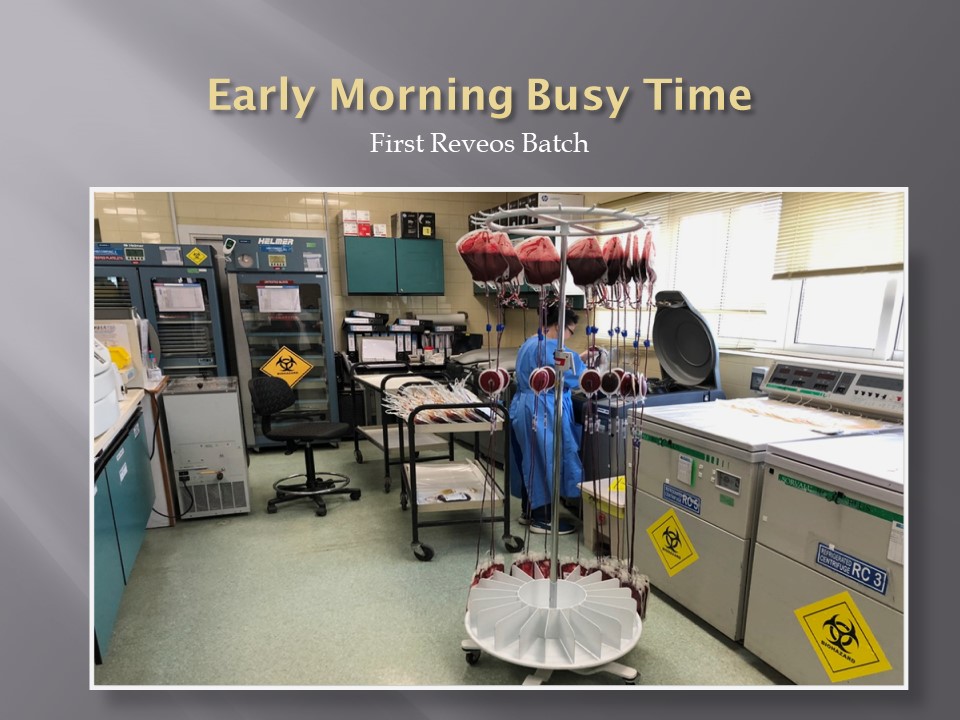
Collection of plasma, platelets, RBCs, or combinations of them using apheresis equipment
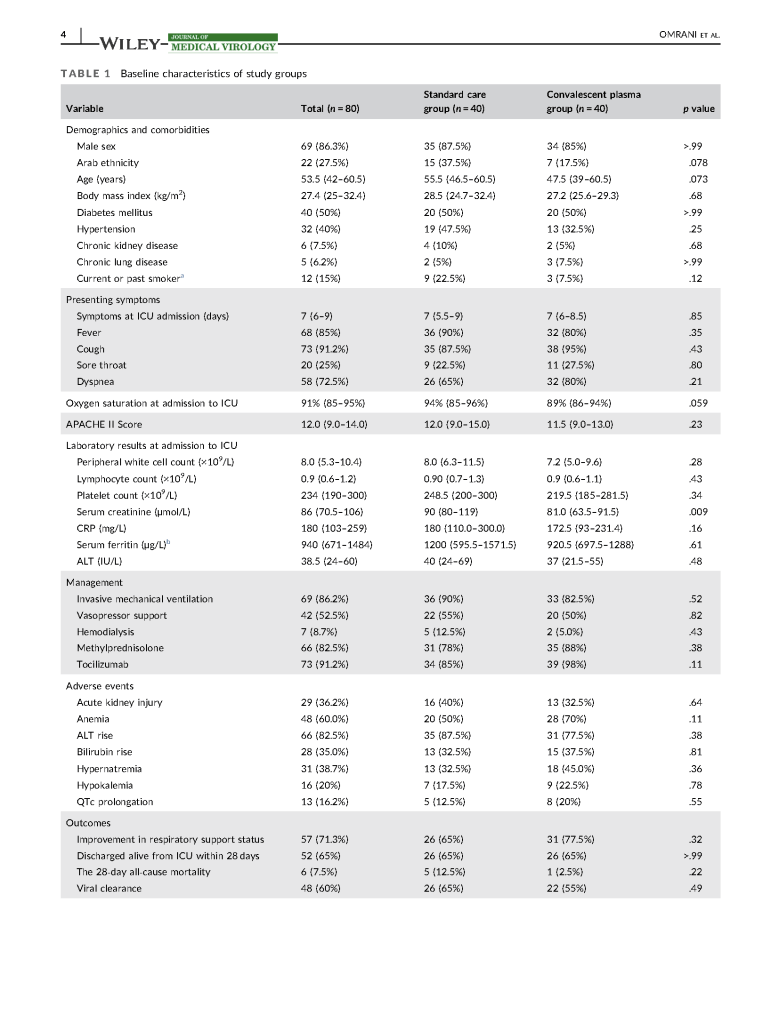
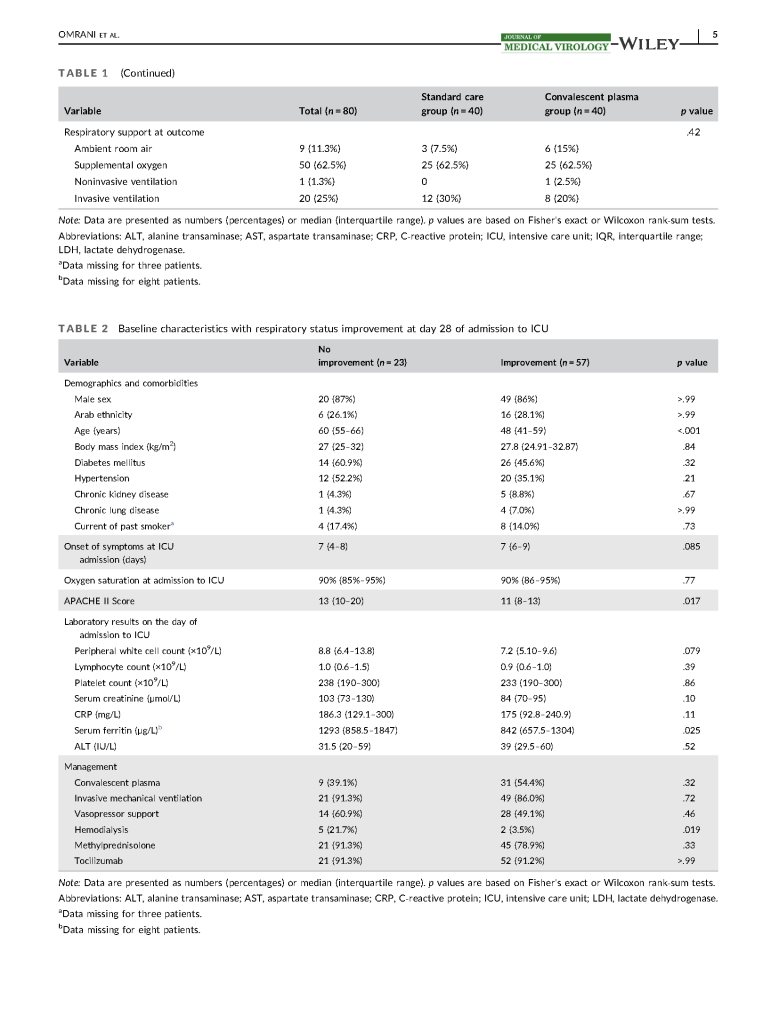
In February 2020, I established COVID-19 plasma collection and distribution for the state of Qatar. Here is a research paper prepared in conjunction with the Qatar Communicable Disease Center about using it for patients there.
This is the policy I developed for HMC Doha Blood Donor Center:
Policy:
References:
Principle:
New rules have been approved by US FDA CBER for body fluid exposure, tattooing, body fluid exposure, and body-piercing. By similar logic we will extend this also to HIJAMA. We will not make any changes to our sexual history/practices or history of sexually transmitted disease treatment.
Policy:
Reference:
Revised Recommendations for Reducing the Risk of Human Immunodeficiency Virus Transmission by Blood and Blood Products, Guidance for Industry, U.S. Department of Health and Human Services, Food and Drug Administration, Center for Biologics Evaluation and Research, April 2020
This is a policy I made for NGHA Jeddah many years ago but is still useful today.
Principle:
All technical staff are required to read and understand the manufacturer package inserts that apply to the procedures that they perform. This policy establishes a means of documenting compliance with this requirement.
Policy Details:
Insert Review Form
| Type of Insert: New Revised |
| Product Name: |
| Date of Insert: |
I have read this insert and understand its contents and accept responsibility for following its instructions and directions.
| Staff Name & Badge #–PRINT! | Signature | Date |
Reading Assignments:
Study Questions:
Revised:
29/8/20
Objectives:
Clinical Responsibilities (after proven competence):
Assessments:
Working Hours:
Reviewed 17/8/20
Objectives:
Venue:
TMS Donor and Transfusion Services
Conducted by: Head, TMS, and senior TMS technical staff
Evaluation:
Discussion of topics with TMS Head and written final examination
Source Materials:
This is a full-time, one-month rotation—attendance in mandatory. Vacations should NOT be taken during this rotation.
Originally Prepared for NGHA Riyadh 31/3/09
Reviewed 26/8/20
Transfusion Medicine includes laboratory and non-laboratory functions. The non-laboratory and purely clinical functions are unique and have no analogy within the general laboratory.
The transfusion service/hospital blood bank laboratory is the closest to a laboratory operation, but there is component modification and complex manual testing, especially for reference immunohematology testing. The staff must make detailed manual decisions, the errors for which could be life-threatening for the patient.
The blood donor center manufactures a pharmaceutical, i.e. blood components with collection, donor qualification, donor abnormal results review, infectious disease marker testing, component production, and donor immunohematology testing—all subject to Good Manufacturing Practices. Never forget: Blood is a drug!!
No other laboratory section is directly responsible for treatment of critically ill patients. Therapeutic apheresis is essential for organ and stem-cell transplants, nephrology, neurology, etc. No other laboratory section is directly responsible for treatment of critically ill patients. Transfusion Medicine physicians are functioning as intensivists. There is no hiding in the laboratory from clinical medicine.
There may also be an industrial manufacturing plant to extract various blood derivatives (e.g. factor concentrates, albumin, Rh immune globulin, etc.) This is pharmaceutical manufacturing on a large-scale basis. There is medical, technical, and special administrative expertise.
Many functions may operate 24/7. The transfusion medicine physician may be on-call for donor issues and review of complex immunohematology problems to acutely decide which blood component (and phenotype) should be given as well as review all adverse reactions to transfusion.
The unique blend of clinical skills is unlike anything else in the laboratory. Also, those outside the blood bank rarely have the skills or judgments for the best course of action for transfusion medicine or for its operations.
The clinical transfusion medicine physician must make acute, life-threatening decisions unlike anyone else in the laboratory. The blood bank technologist is at the cutting edge of the battle with his testing and interpretations. No other area of the laboratory is at such risk for injuring or even killing the patient. There is high stress and burn-out.
I have talked with many blood bankers and many seem to share the exasperation that the laboratory does not understand us. The latter looks at blood bank testing like that coming off a hematology or chemistry analyzer—although patients rarely would have severe morbidity or mortality like the blood bank from errors in those analyzers.
No laboratory pathologist has the pressure of the blood bank physician on-call. It really is 24/7 and requires a broad, clinical background to make the right decisions. It is very stressful and does not permit a good night’s sleep.
Thus, I make my case to separate us from the laboratory. We can form our own more effective administrative organization and optimize our own planning. Regretfully, I have never worked in such an administrative structure. I also am a realist that cost-containment nowadays makes it much less likely high administration would permit this change for a mere cost center. This will probably never happen during my career.
Finally, Transfusion Medicine is an essential service. Blood components are essential drugs. The operations and staff must be free of political influences. This is a service for the entire region or country like the fire department, civil defense, etc.
8/8/20
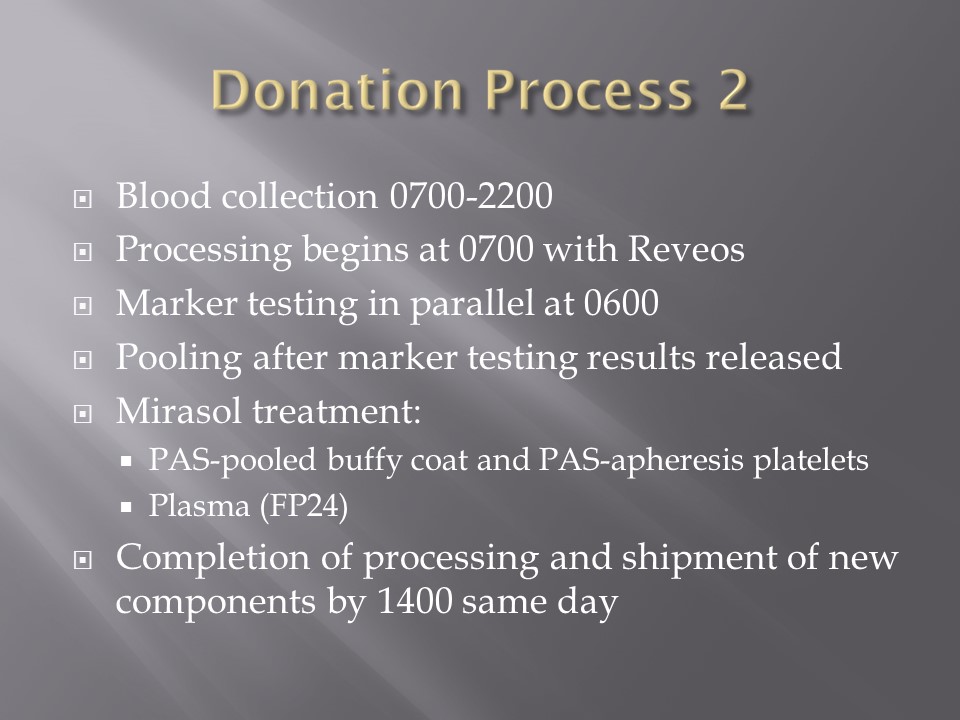
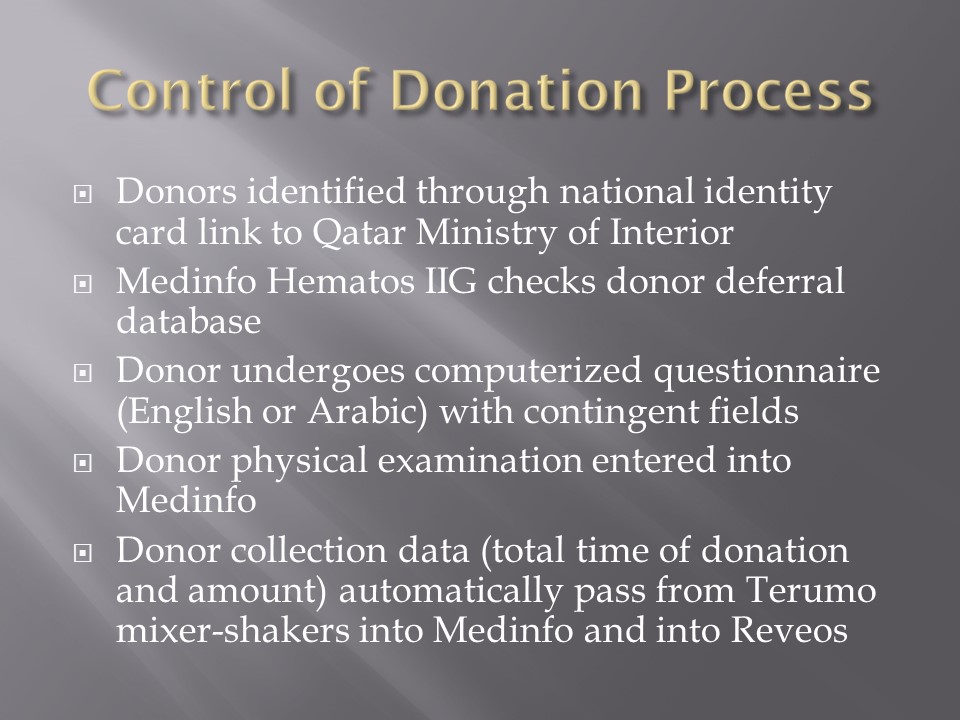
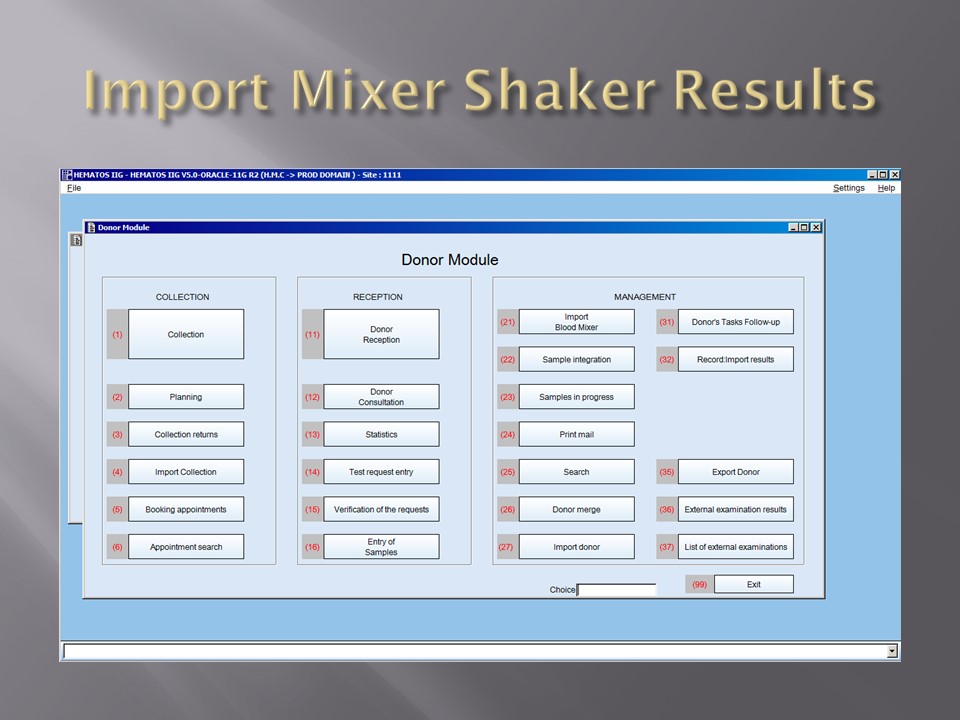
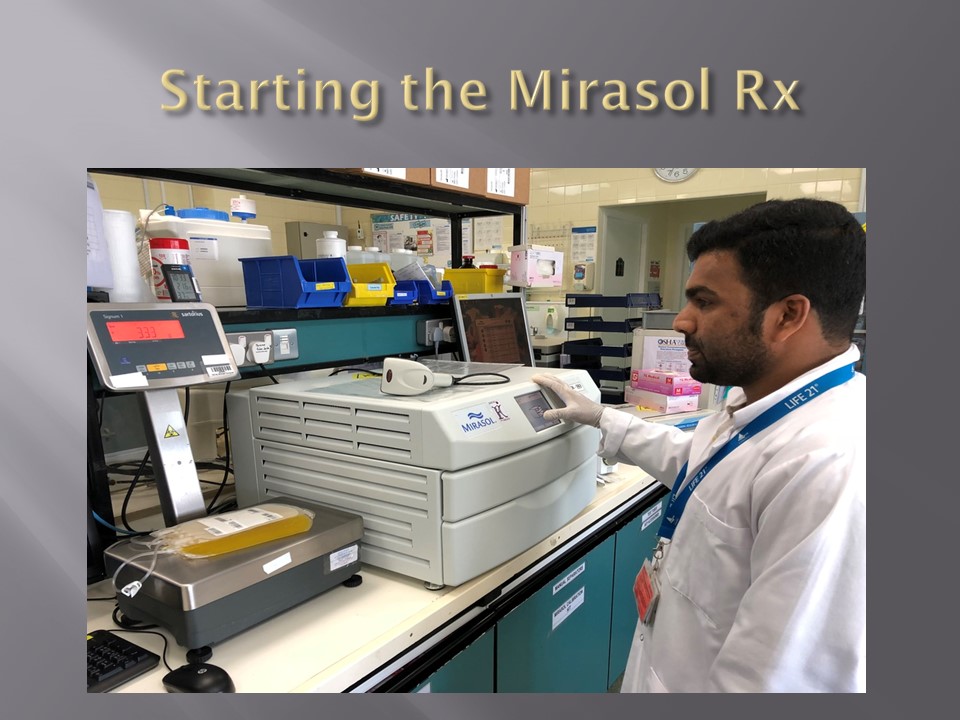
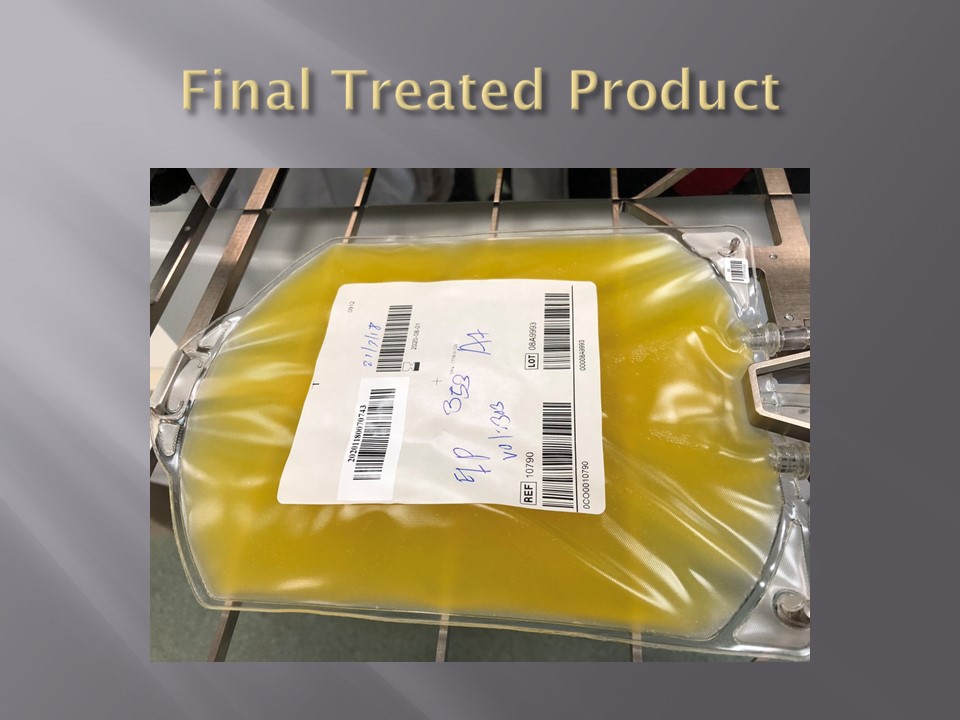
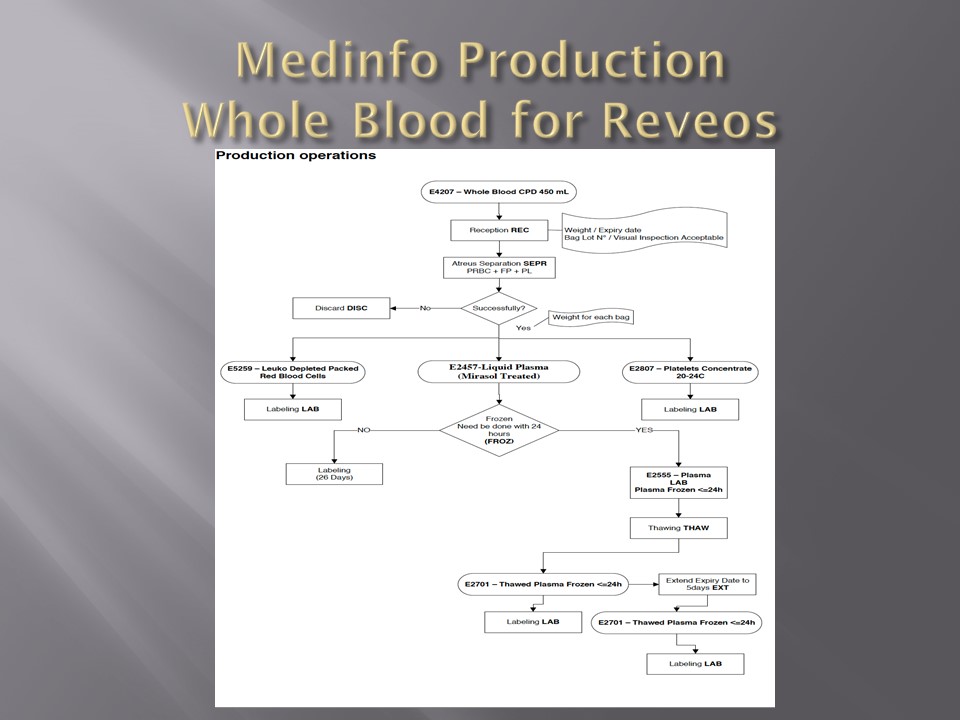
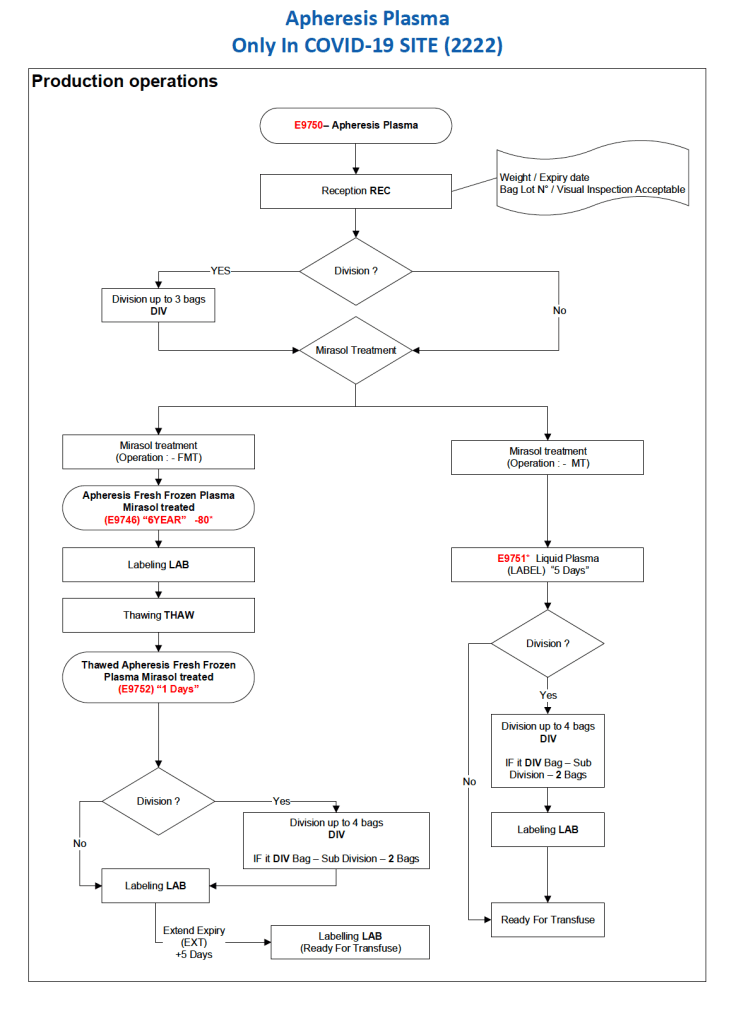
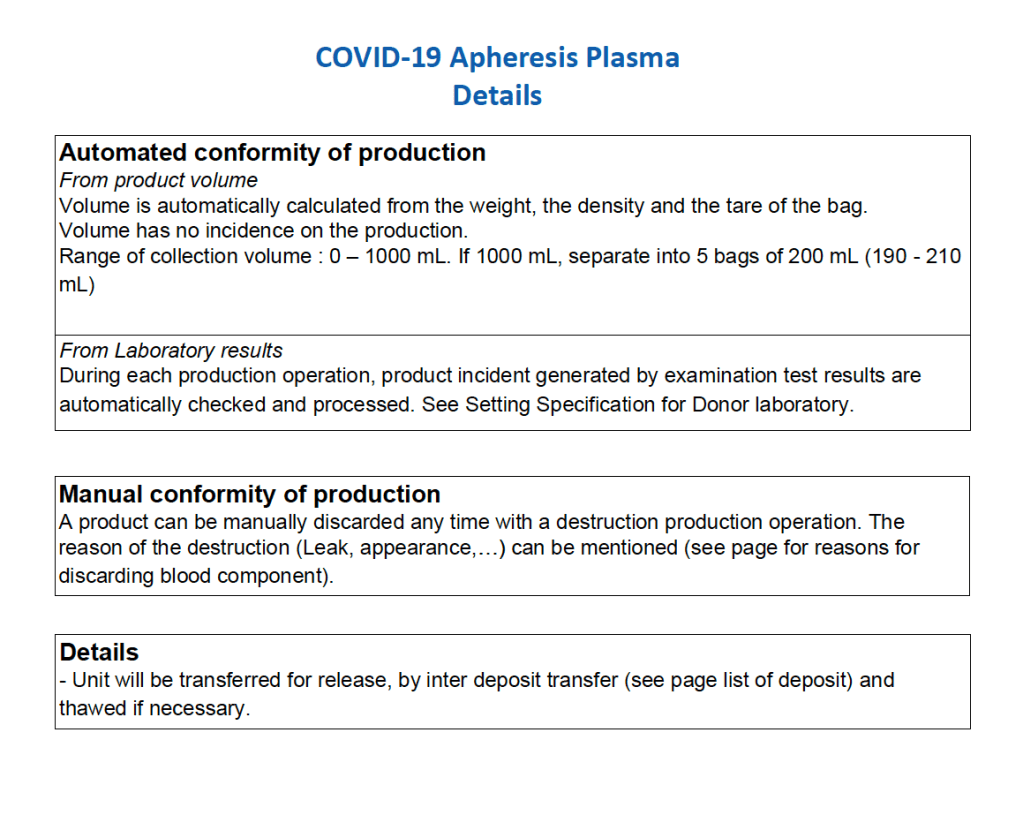
After the initial manual setup of the CCP program, the Medinfo process was set up. The following workflow shows the production of CCP from the raw apheresis collection, including division into aliquots based on the total volume. The plasma volumes were kept within the range for riboflavin pathogen inactivation (Mirasol).
The usual safeguards for production were also in effect for CCP. The product could not be labelled without all criteria (donor screening, collection, marker testing) being met. Furthermore, the inter-depot and transfusion service processes still applied. However, all steps were done in quarantine at a location separate from the regular processes. Also, the actual ordering and release of CCP was restricted to the quarantine hospital blood bank site.
The following outline the production process:
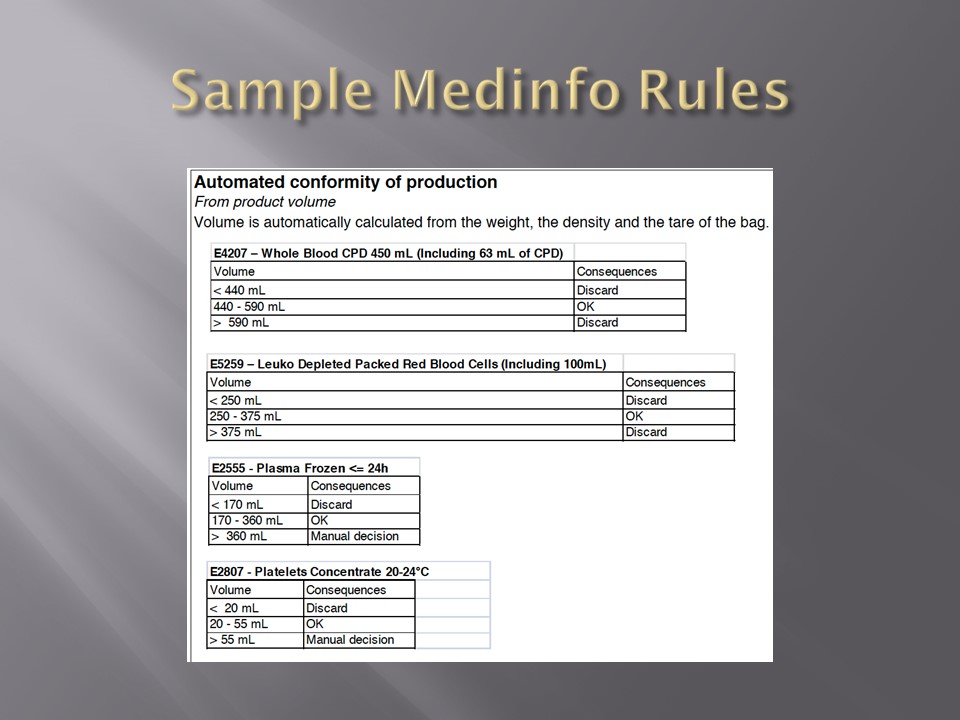
This Powerpoint file summarizes the past previous posts about the use of automated components, pathogen inactivation, and their synergism with the blood bank computer software Medinfo Hematos IIG