Always review the transfusion history of all component types, medication history, and the clinical history!! Start with this first.
Receipt of plasma with anti-D (RhIG, IVIG, etc.)–passive antibodies
Partial D with anti-D:
Partial or mosaic D patient who received D positive RBCs and made anti-D directed against its missing epitopes
Anti-G:
Not all anti-G is anti-C and anti-D: It is really a separate specificity. It is possible that anti-G may be made even though the patient is C-positive.
Anti-LW:
However, it is unlikely to show such strong reactions
As a transfusion medicine physician, I must know if I can trust my staff’s interpretation of immunohematology testing. I may be called at night and they will provide me with results and I must use these to make a medical judgment. If their interpretation is flawed, I might make a decision that harms the patient.
I really don’t like multiple-choice questions, but nowadays this is often the norm. For my staff, especially senior staff and those who want to be promoted to senior staff, I have developed a series of projective exercises to help me understand their thought processes. I emphasize that I do not want a mere regurgitation of isolated facts: I want integration of the facts into useful information!!
The following is my favorite assessment, offered to advanced staff and candidates for senior technologist, supervisors, and technical manager positions. Usually, these staff have SBB, ART, FIBLS or equivalent qualifications.
You are reviewing abnormal test results and receive the following case:
Anti-A: 4+
Anti-B: 0
Anti-A,B 4+
A1 cells 0
B cells 3+
Anti-D 3+
D-control 0
Antibody Screen: 3+ in SC1 (R1R1), 4+ in SC2 (R2R2), 0 in SC3 (rr)
Antibody Identification: Anti-D
Give possible explanation(s) for this situation. Request any additional information you need.
As a transfusion medicine physician, I must know if I can trust my staff’s interpretation of immunohematology testing. I may be called at night and they will provide me with results and I must use these to make a medical judgment. If their interpretation is flawed, I might make a decision that harms the patient.
I really don’t like multiple-choice questions, but nowadays this is often the norm. For my staff, especially senior staff and those who want to be promoted to senior staff, I have developed a series of projective exercises to help me understand their thought processes.
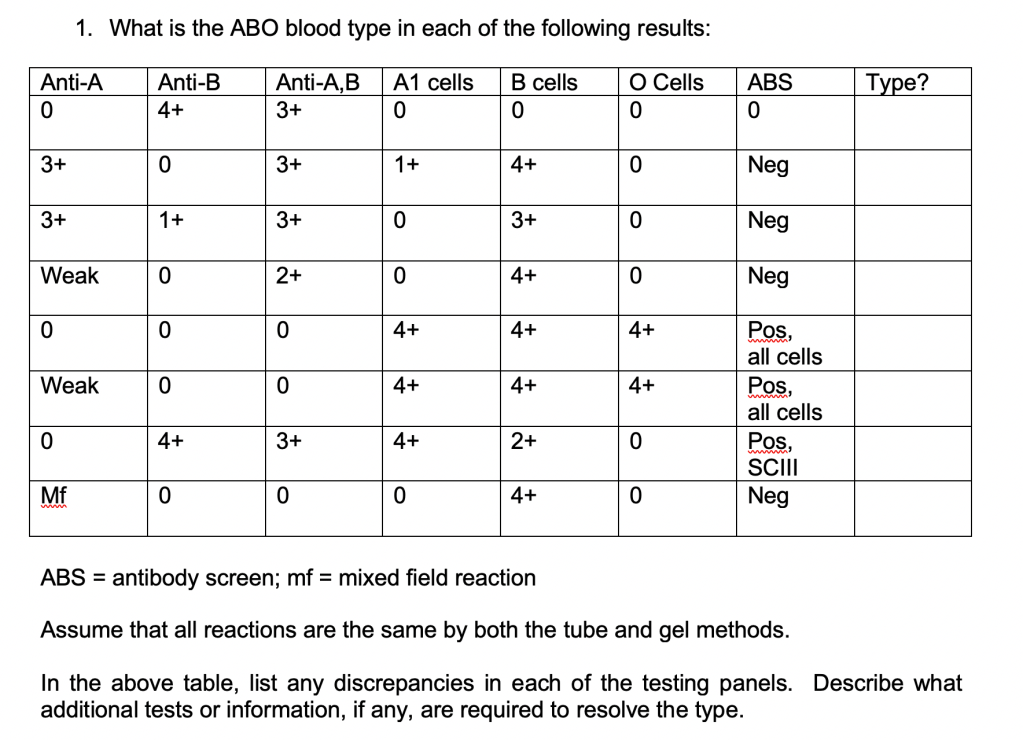
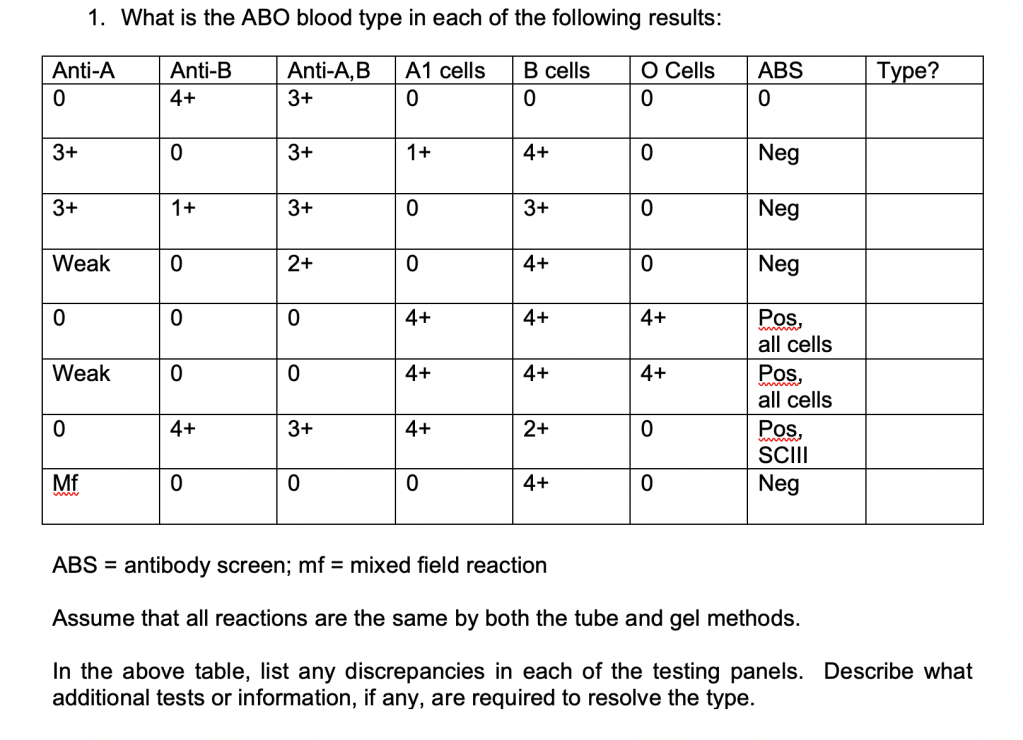
Here is another exercise for ABO discrepancies. I offered this to senior technologist and supervisory candidates:
Can they name the conditions that give these results?
As a transfusion medicine physician, I must know if I can trust my staff’s interpretation of immunohematology testing. I may be called at night and they will provide me with results and I must use these to make a medical judgment. If their interpretation is flawed, I might make a decision that harms the patient.
I really don’t like multiple-choice questions, but nowadays this is often the norm. For my staff, especially senior staff and those who want to be promoted to senior staff, I have developed a series of projective exercises to help me understand their thought processes.
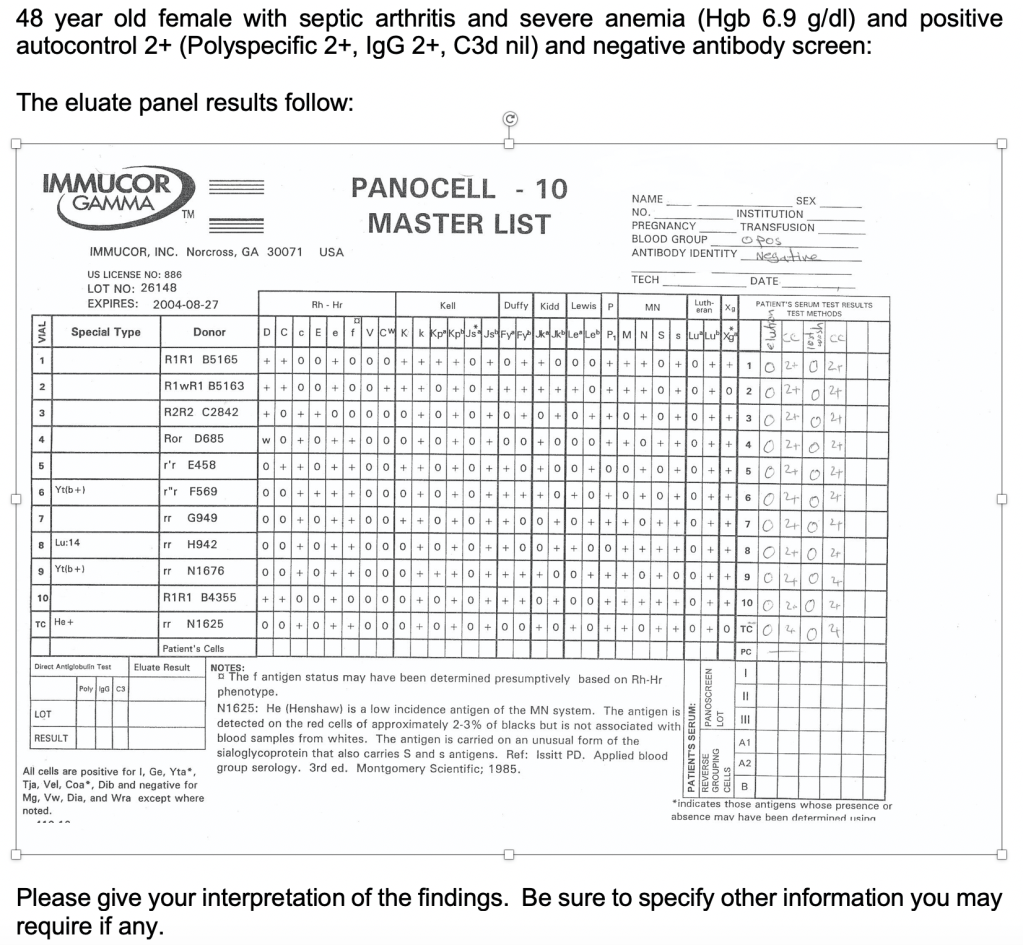
Here is another exercise using elution:
Will they know to get the medication history? What are the mechanisms by which a drug may cause a positive DAT?
As a transfusion medicine physician, I must know if I can trust my staff’s interpretation of immunohematology testing. I may be called at night and they will provide me with results and I must use these to make a medical judgment. If their interpretation is flawed, I might make a decision that harms the patient.
I really don’t like multiple-choice questions, but nowadays this is often the norm. For my staff, especially senior staff and those who want to be promoted to senior staff, I have developed a series of projective exercises to help me understand their thought processes.
Here is another series of exercises, usually given to advanced technologists and supervisor candidates. I want them to tell me what they need to assess each scenario. Can they definitively diagnose solely on the information provided?
These are open-ended and may have more than one possible interpretation:
As a transfusion medicine physician, I must know if I can trust my staff’s interpretation of immunohematology testing. I may be called at night and they will provide me with results and I must use these to make a medical judgment. If their interpretation is flawed, I might make a decision that harms the patient.
I really don’t like multiple-choice questions, but nowadays this is often the norm. For my staff, especially senior staff and those who want to be promoted to senior staff, I have developed a series of projective exercises to help me understand their thought processes.
Here is another exercise, usually given to physicians. I give them the following scenario:
There is a major trauma on an unidentified young adult male patient. We do not know the transfusion, medical, or medication history. They need six units RBCs STAT.
What blood type do you select? How do you release the blood?
You give the 6 units and receive a specimen back. The patient’s typing reactions are:
Forward type: Anti-A, anti-B both negative
Reverse type: 4+ reaction with A1 and B cells
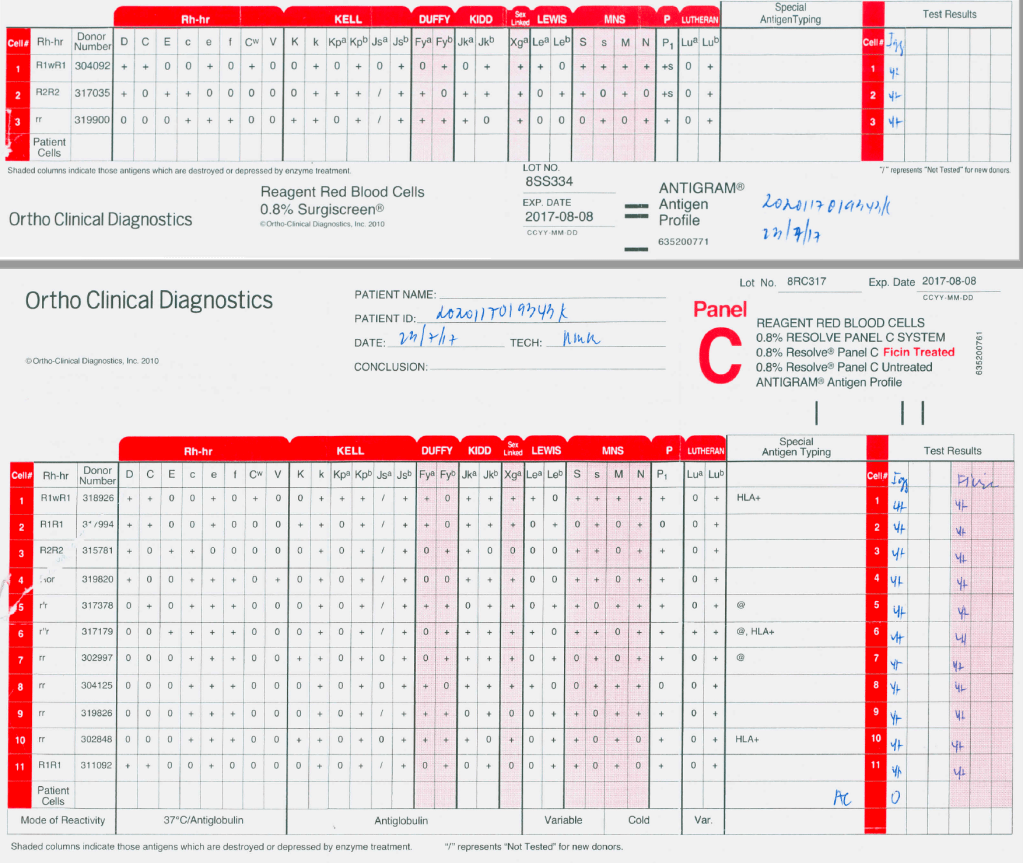
About 15 minutes later, your technologist tells you that the antibody screen is 4+ in all cells and all panel cells react 4+ both at AHG and enzyme phases. What do you tell the treating clinician? What do you do?
The technologist in panic has been performing AHG crossmatches but all 4+ incompatible.
Here is the panel:
I have them review this panel and tell me to interpret it
What further testing would you do, if any?
What blood type do you release now?
What is the significance of the negative autocontrol when there is panreactivity?
What if the enzyme panel results are all negative?
What if the autocontrol is 4+?
The smart ones will ask for a full extended phenotype (e.g. Diamed/Biorad’s three profile cards) and for anti-H.
I tell them the clinician is very angry and demands you release more group O blood immediately? How do you respond?