This is an update of a presentation I gave while working as Head of Transfusion Medicine for Saudi Arabian National Guard Affairs, King Abdulaziz Medical City at Riyadh. I used this strategy there and later at HMC Doha.
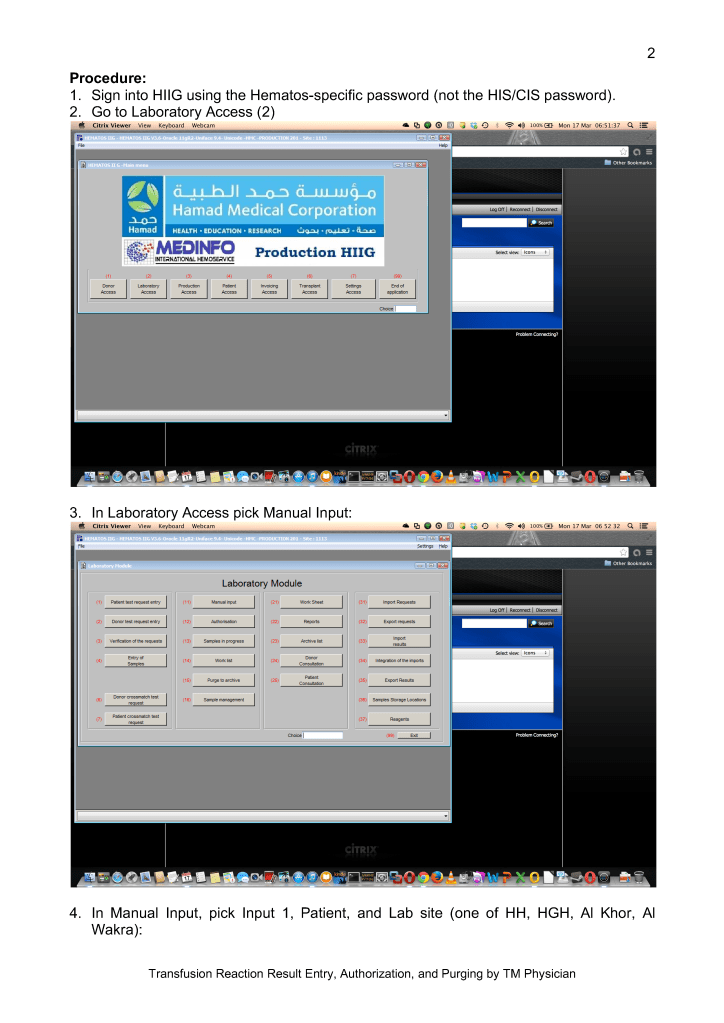
Fortunately we had access to rare antisera such as anti-Tja (anti-PP1Pk) which we could purchase from Diamed AG and its successor Biorad. I emphasize that we only sparingly used these rare antisera AFTER ruling out more common high-incidence antibodies.
This is a teaching document of a process to irradiate RBC components when our irradiators are not functioning. In our system, we used Mirasol pathogen-inactivation so our RBC units were affected. The number of units for advance irradiation was based on our historical usage of irradiated units across our system. The workweek is Sunday-Thursday so on Thursday special effort was made to have the minimum number of irradiated units available.
We used irradiated units for compatibility testing to avoid the possibility that the unit would be released without irradiation.
Emergency Interim Procedure:
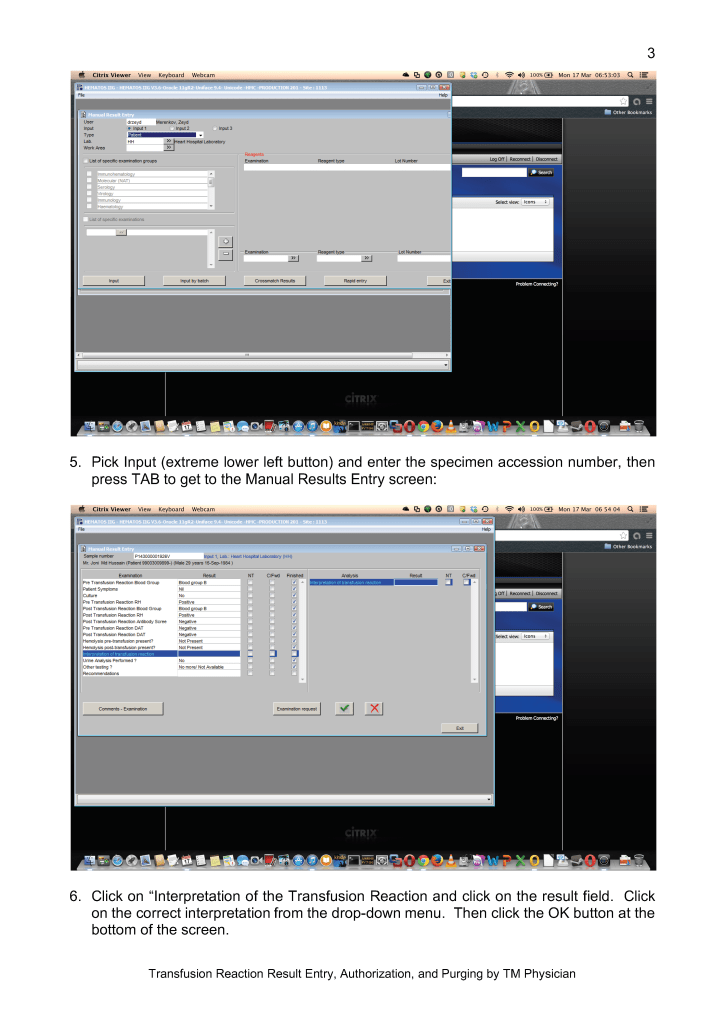
Verify the patient’s diagnosis/location: All Hematology-Oncology patients should receive irradiated blood. Refer to the list of diagnoses for which irradiation is indicated (attached).
Only PRBCs need to be irradiated. Mirasol-treated (pathogen-inactivated) platelets can be used directly without irradiation in accordance to Council of Europe CE regulations.
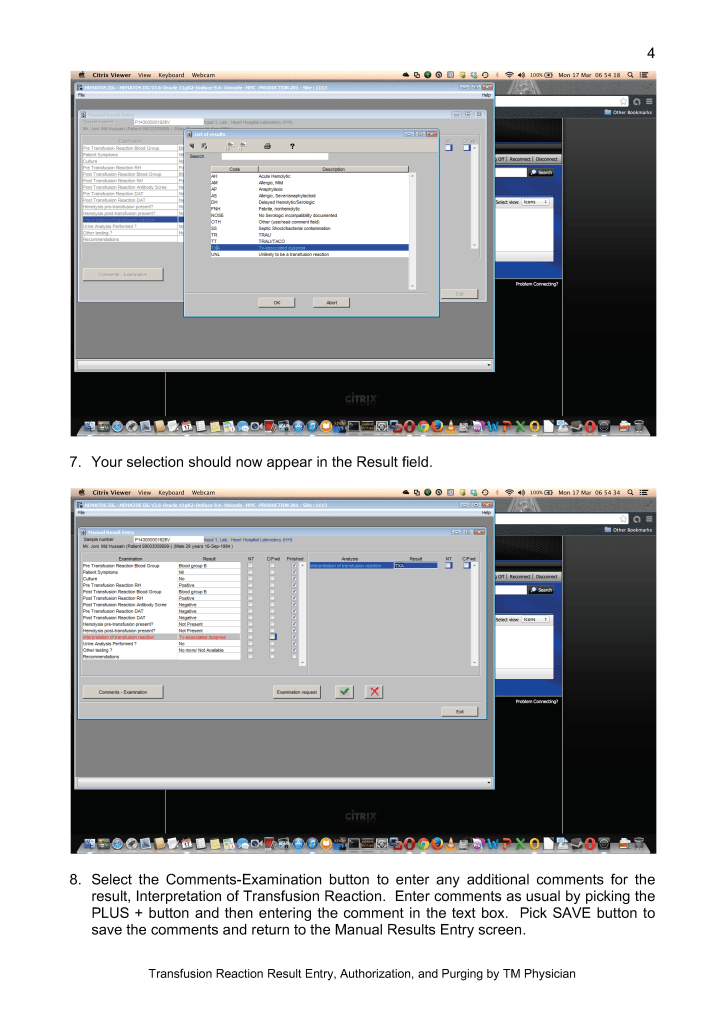
Attach radiation indicator labels to the selected units as per the irradiation procedure.
Send the units for irradiation to the Radiation Oncology department.
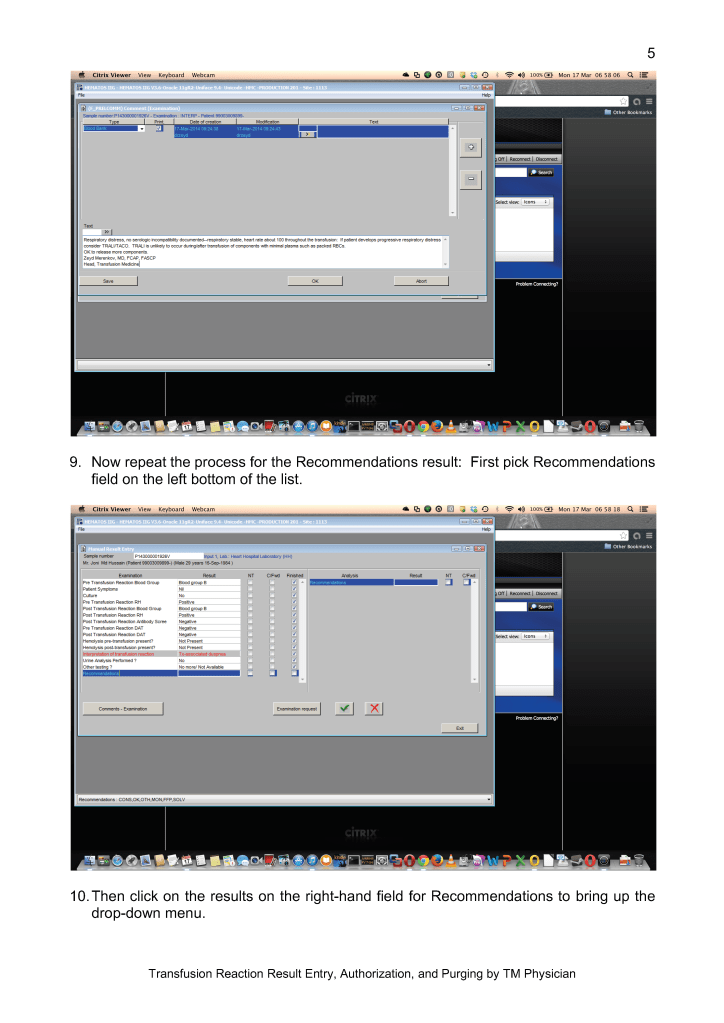
Verify that the proper dose of irradiation was received while in the Radiation-Oncology department.
Keep a minimum stock of 20 group O-positive units irradiated at the start of each day AND before the start of the weekend on Thursday afternoon. Irradiate that number of group O-positive units plus any other specific requests for blood.
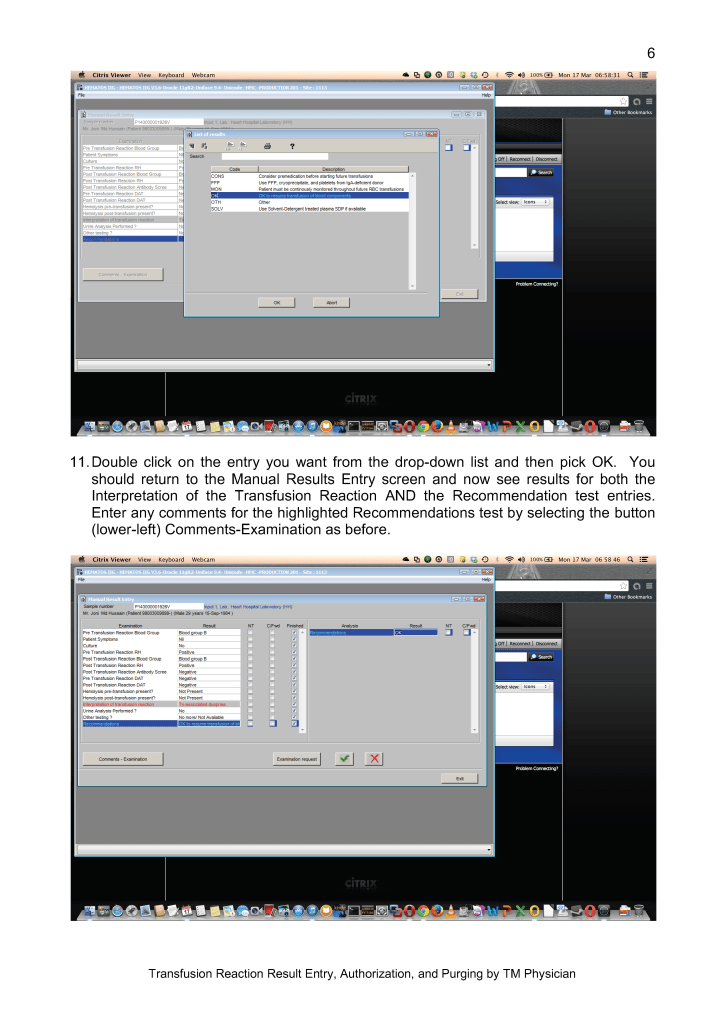
You should use the irradiated units for crossmatching. DO NOT CROSSMATCH FIRST BEFORE IRRADIATING!! If the antibody screen is positive, refer the specimen to the Transfusion Service for further processing and selection of units.
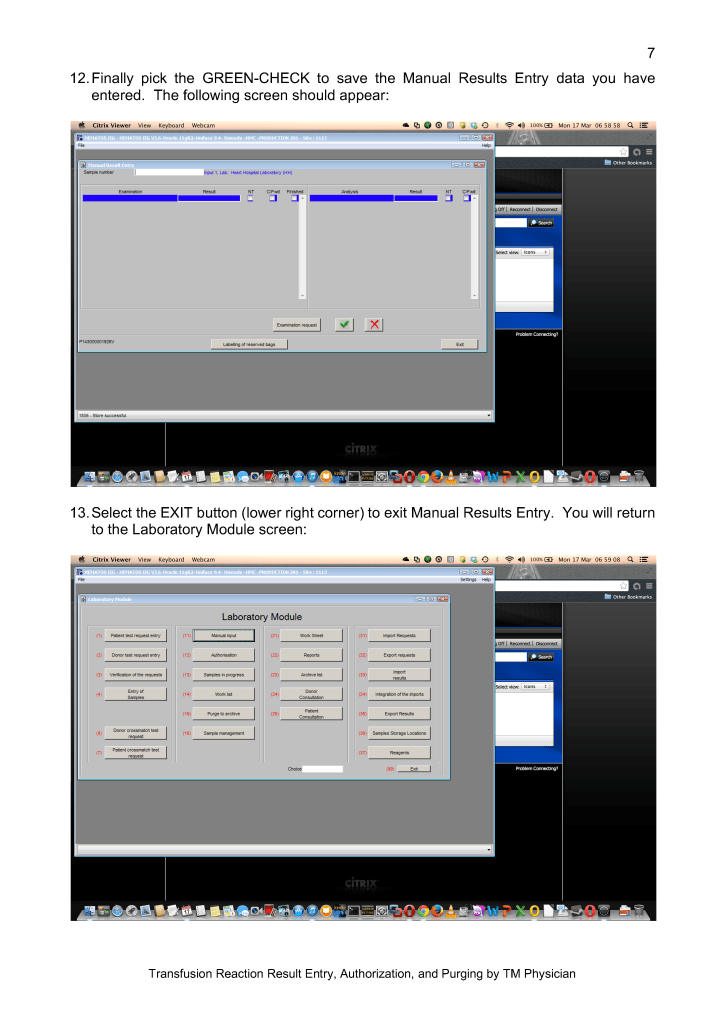
Note: If a special antigen typing is needed, we may have to irradiate after selecting the antigen-matched unit if it is not found in the group of irradiated units.
If a unit is required for a child < 20 kg, it must be washed before release if the unit was irradiated more than 24 hours previously according to our irradiation policy.
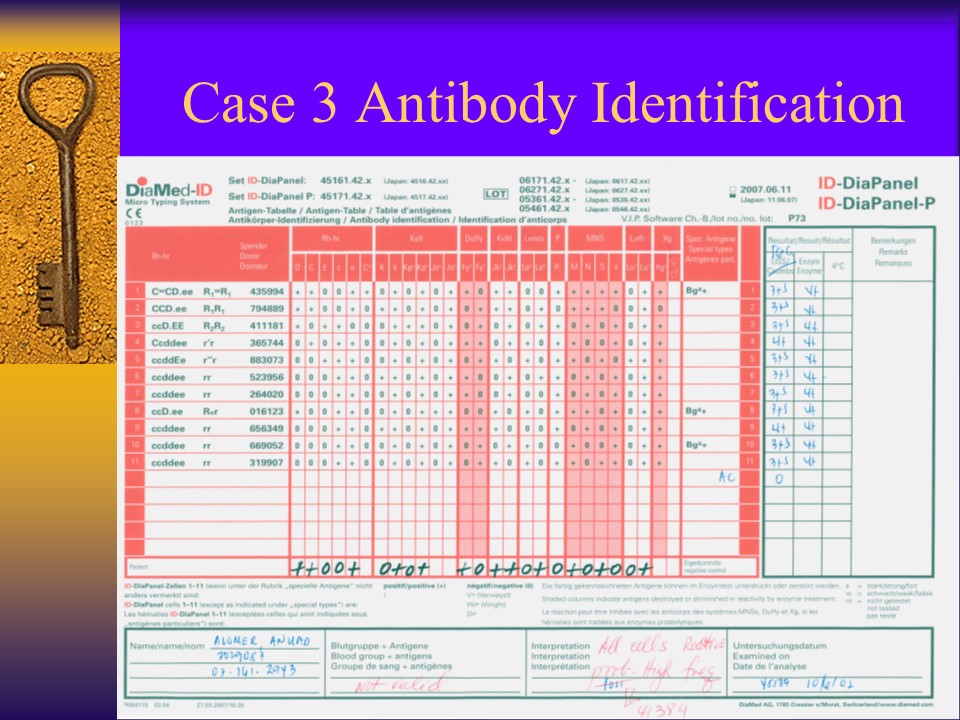
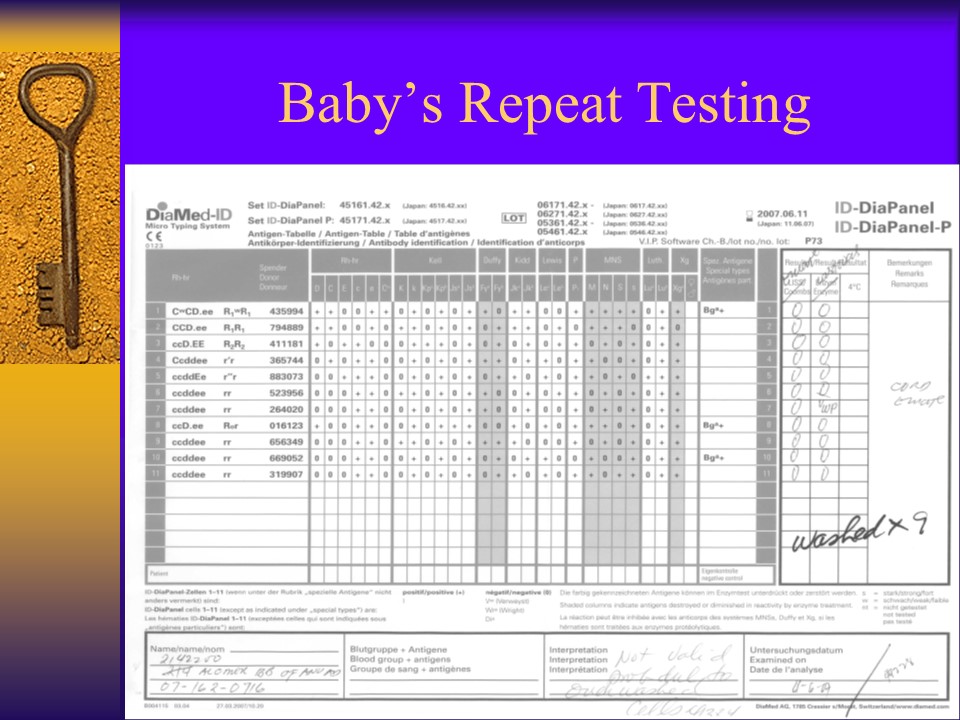
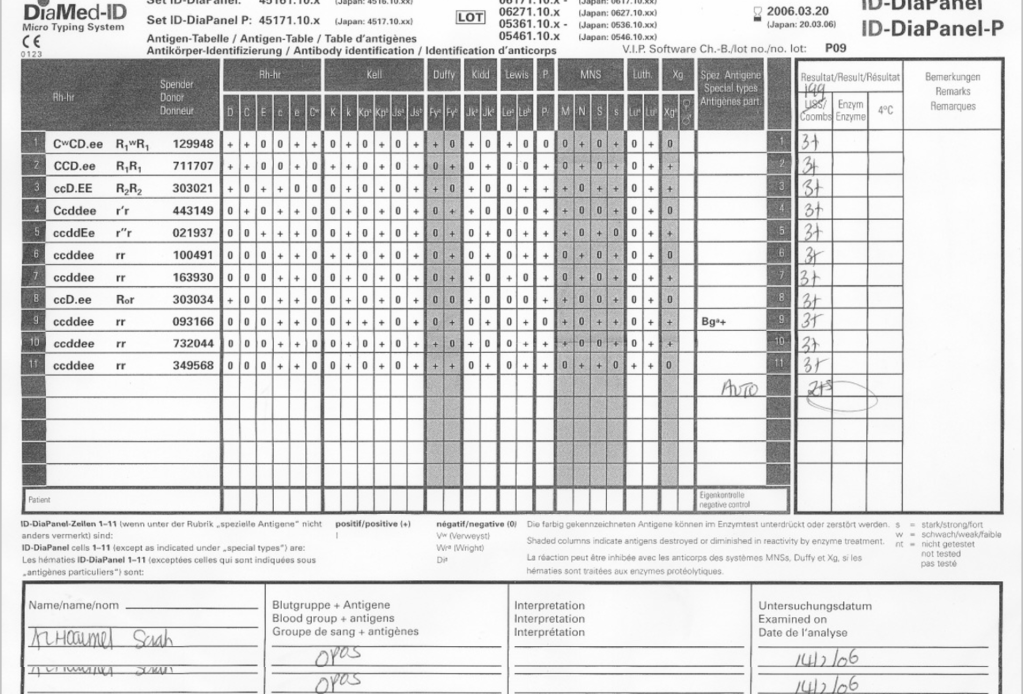
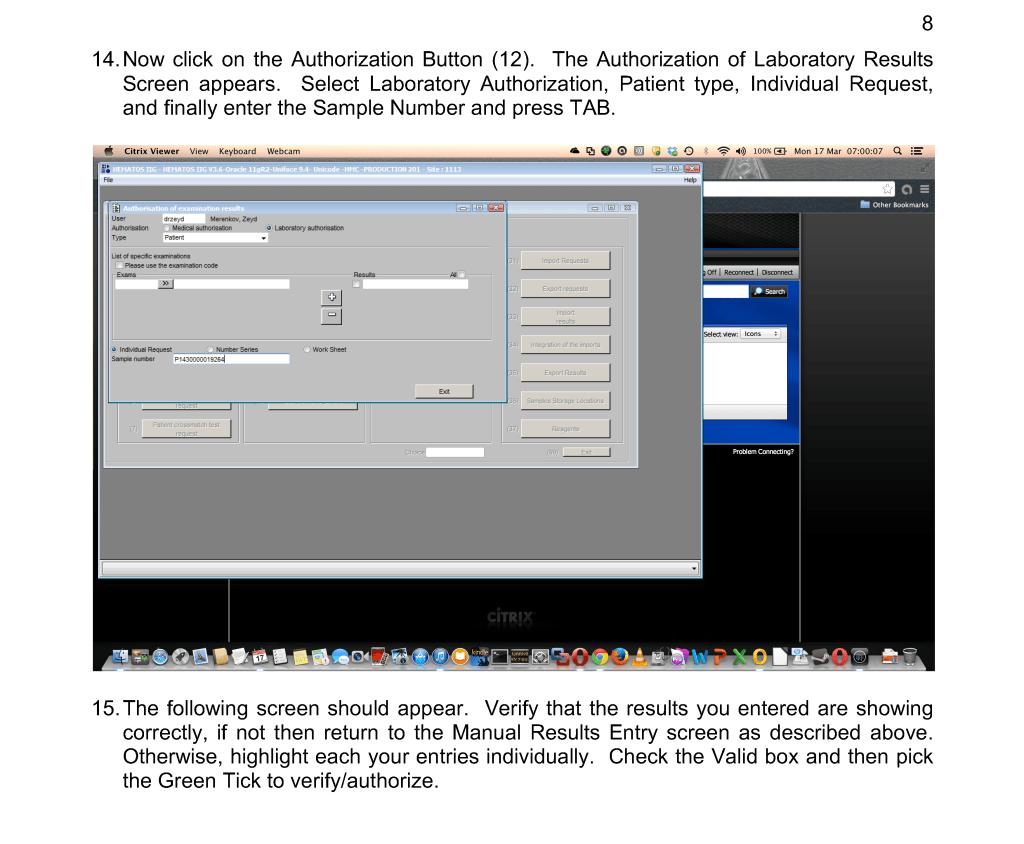
Whenever I had a “nonspecific” antibody, I had to first rule out issues with the reagents themselves. The following example shows weak to 2+ reactions in the panel cells and autocontrol.
The variability in the reactions made me initially uncomfortable about called this WAIHA. I then checked the panel details: the testing was done only six days before the panel outdate.
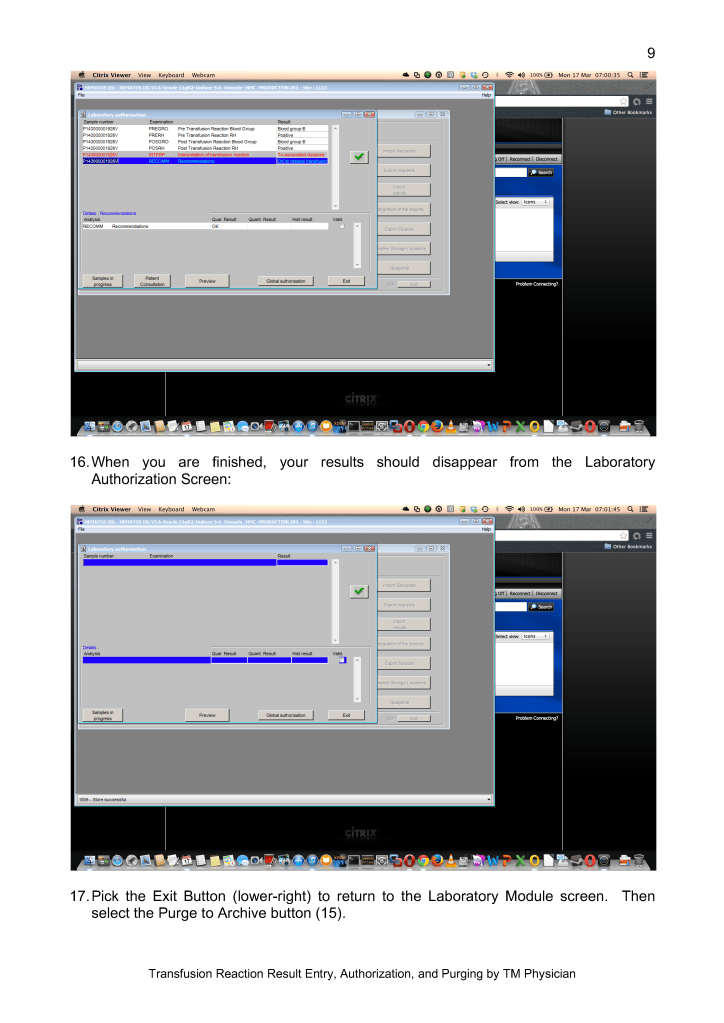
I told my staff to repeat the workup with the new panel expiring five weeks later. The difference is astounding!!
Remember: if you work in the Middle East, the environmental conditions can be extreme in summer (>50C). Do you know how your reagents were handling during transport?
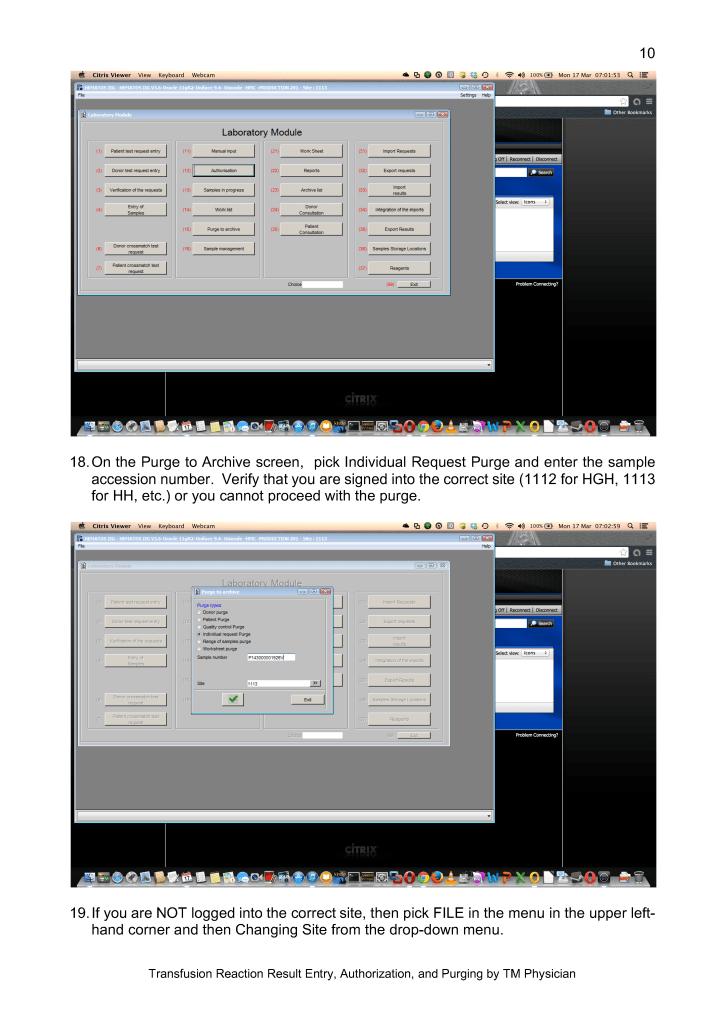
My advice: if you are concerned there is a clinically significant antibody but cannot confirm it, consider repeating the workup using fresh reagents and a fresh specimen. Repeating the workup after a few days may make the detection clearer.
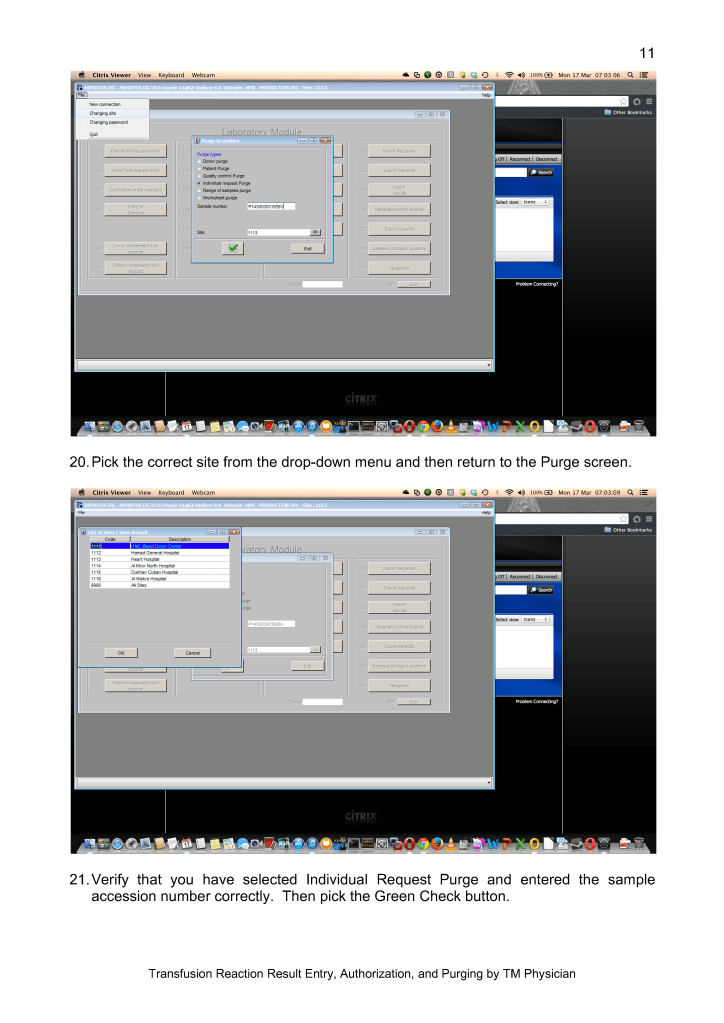
This is a repost of this rare antibody with a few new additional comments.
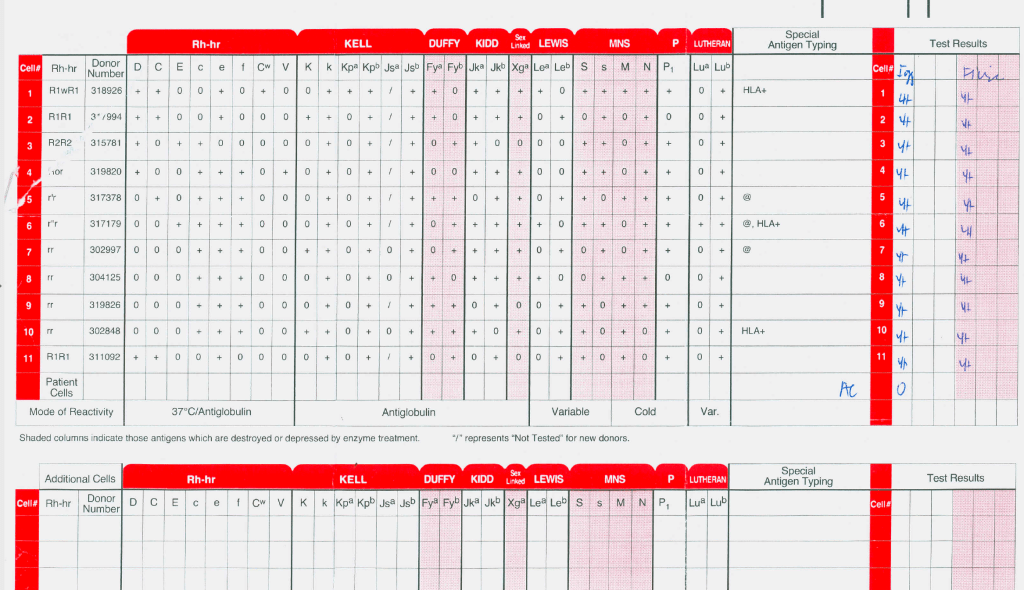
This is a rare anti-Jka antibody that only reacts with polyspecific AHG and only in homozygous Jka+ cell. In the past three decades, I have only seen three of these.
Almost all anti-Jka and anti-Jkb antibodies can be detected using heavy-chain gamma specific AHG. I prefer to use this reagent since it minimizes interference from cold antibodies.
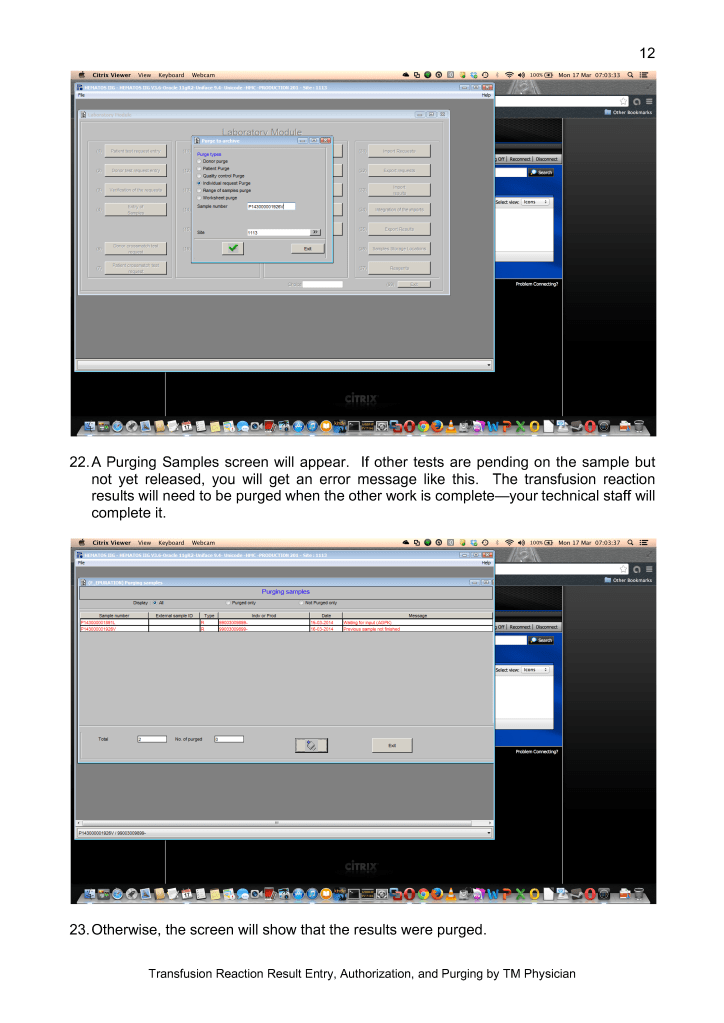
Whenever you have a nonspecific antibody, never discount the possibility of a Kidd antibody. Consider doing extended phenotyping and include Jka and Jkb typing and always check for dosage effect. I have a specific post on my approach to nonspecific antibodies.
Select antibody screening cells including homozygous Jka+ and homozygous Jkb+. This usually requires a three-cell screen.
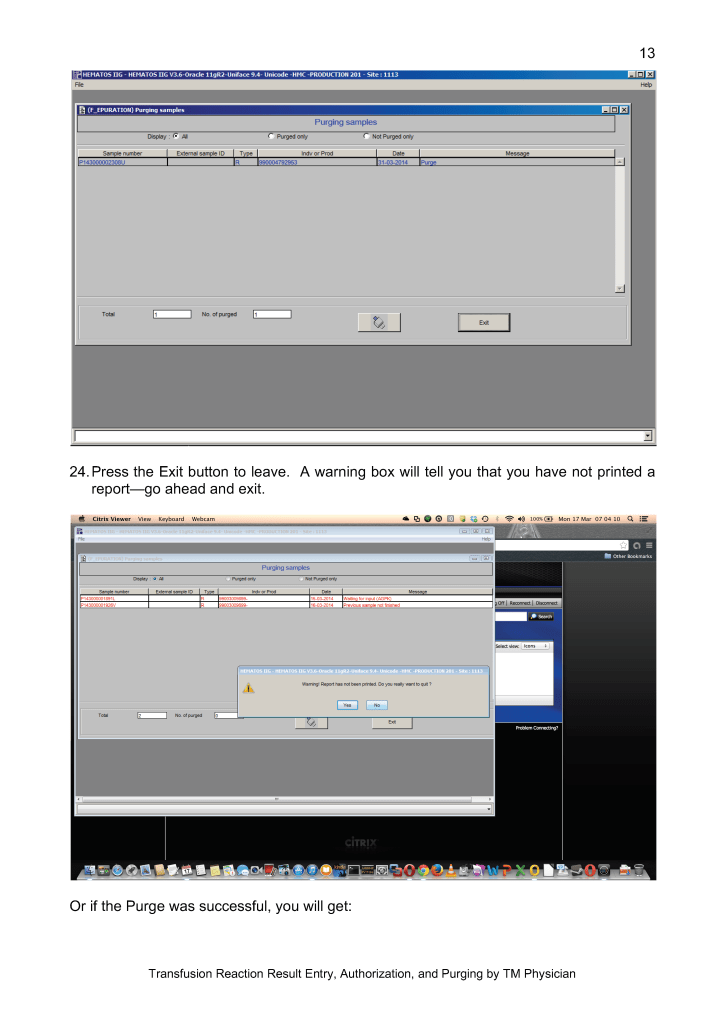
Never forget that a negative result only means not-detected. If there is other evidence for hemolysis, consider performing additional studies.
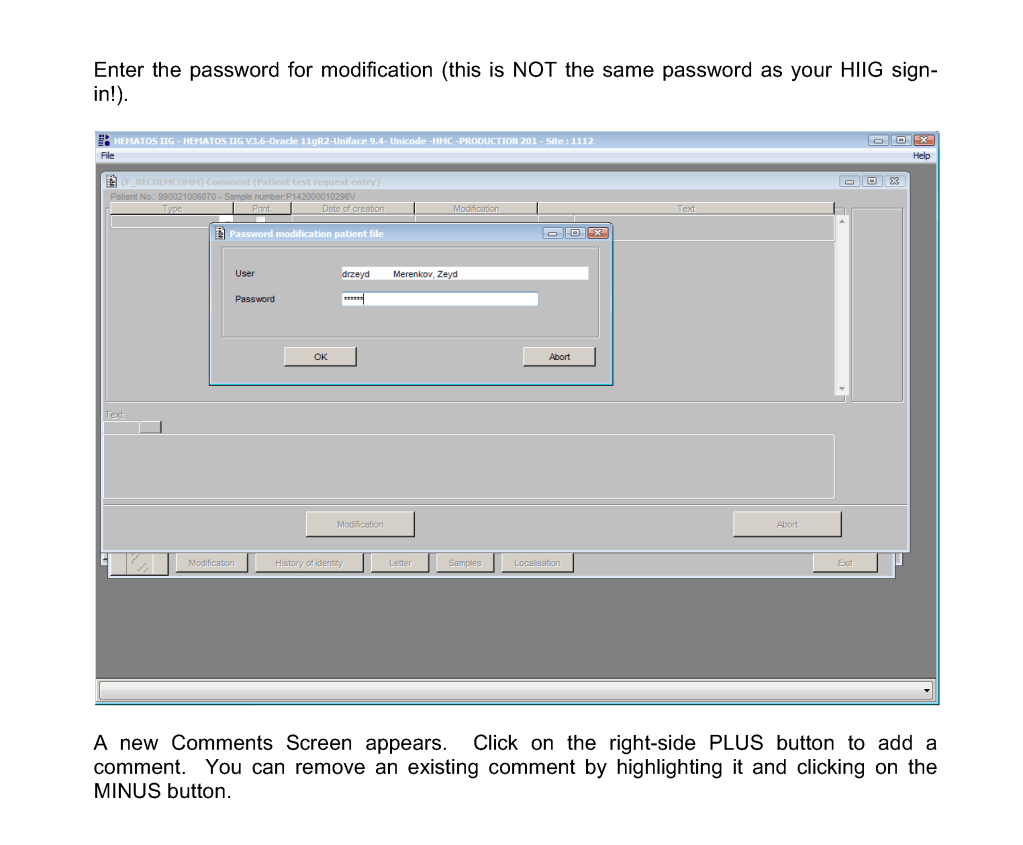
There are several different types of comments in HIIG:
Donor Global
Patient Global
Analytical Comments
Result Comments
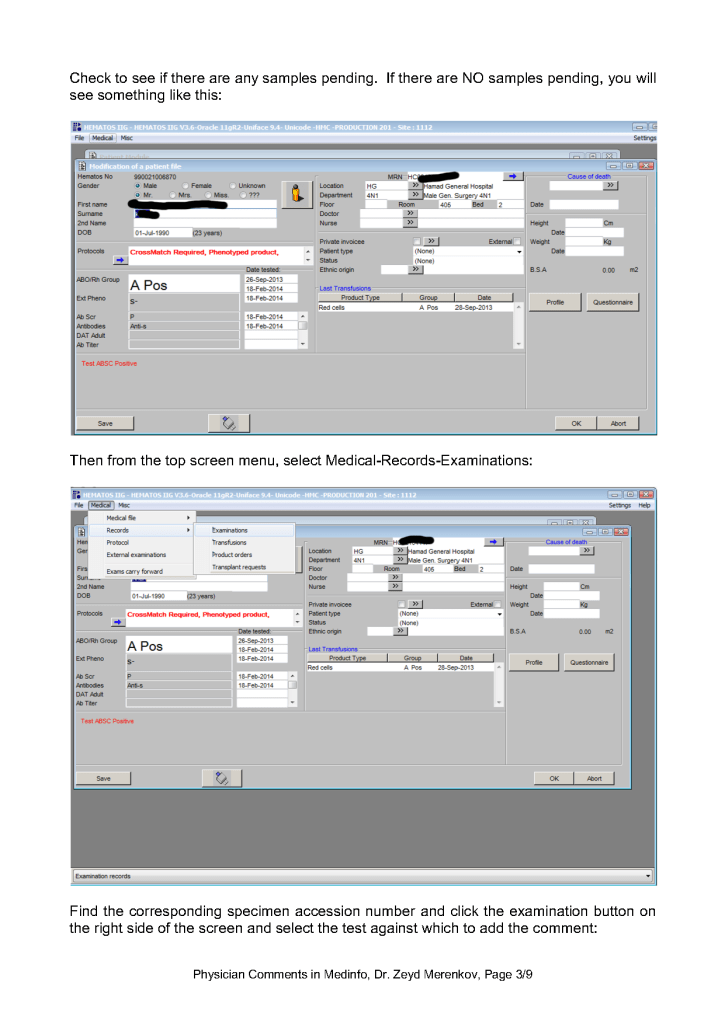
Physicians may enter any of these comment types. Comments may be entered before or after a test is authorized/verified. If entered after authorization, the test must be modified to accept the comment. Only result comments are visible in the patient’s medical record.
Policy:
Physicians should use comments in the following situations:
Interpretations of DAT, antibody identification, ABO discrepancies
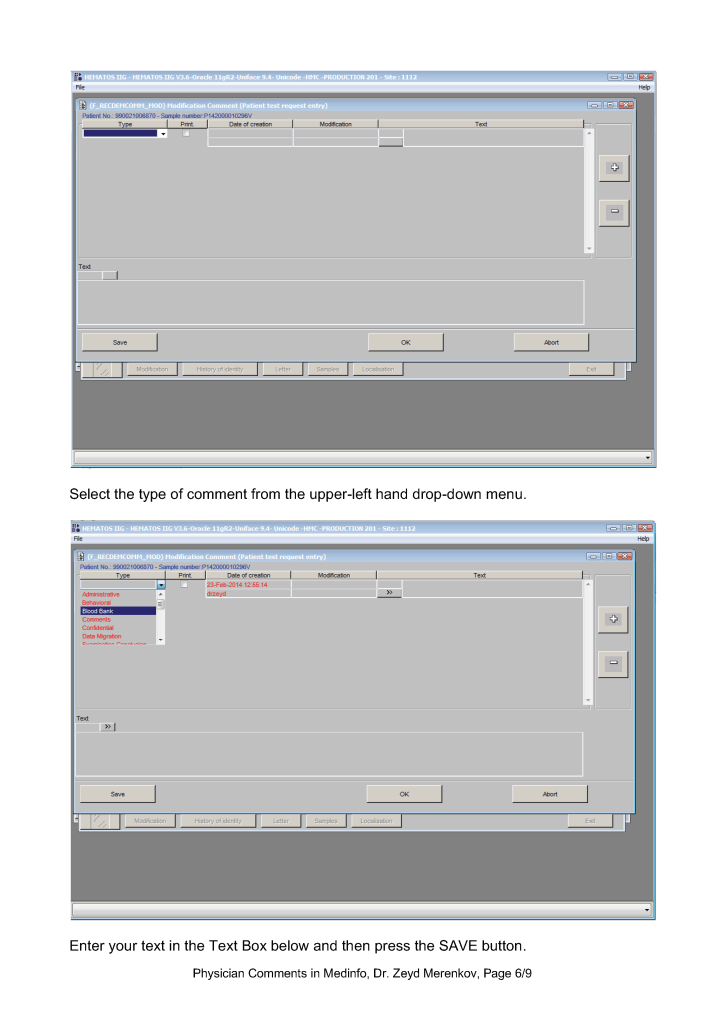
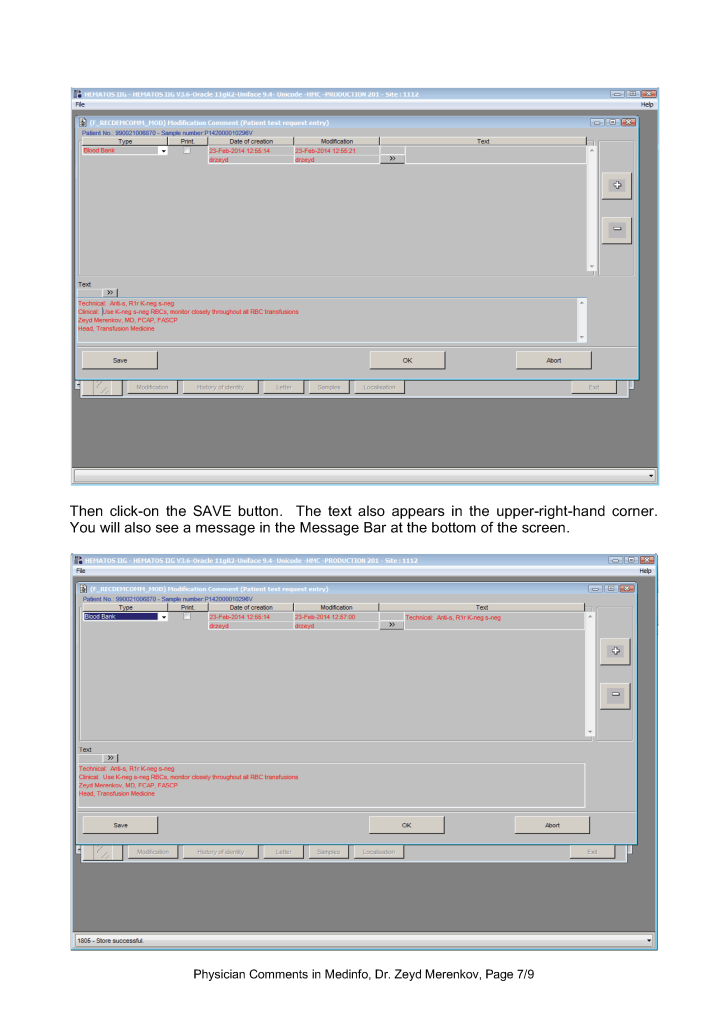
Instructions for the selection of specific and/or modified blood components
Donor eligibility issues (e.g. donor marker testing abnormalities and disposition)
Donor reactions
Telephone call documentation
Donor counseling documentation
Any special instructions to staff
Any other situation where the transfusion physician determines it is desirable to enter a comment
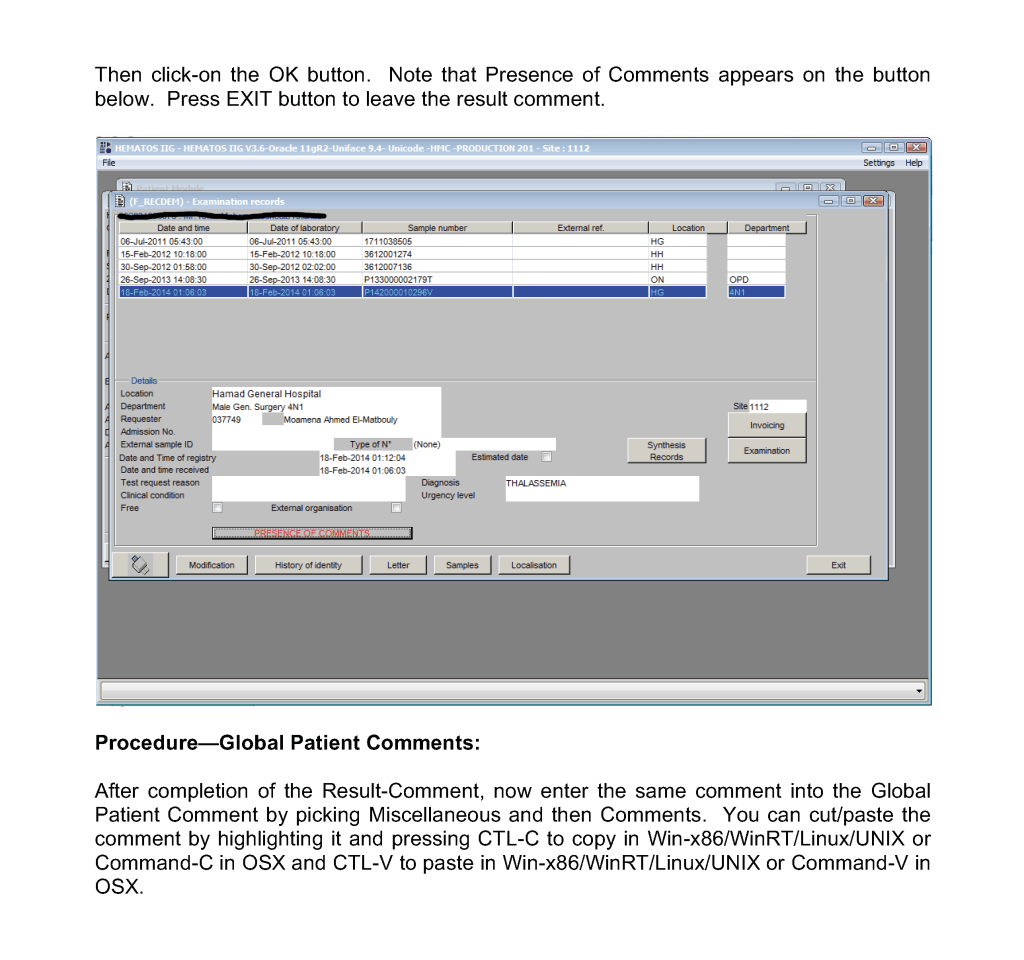
Copy all result-comments and also enter then as global comments against the patient or donor record as applicable.
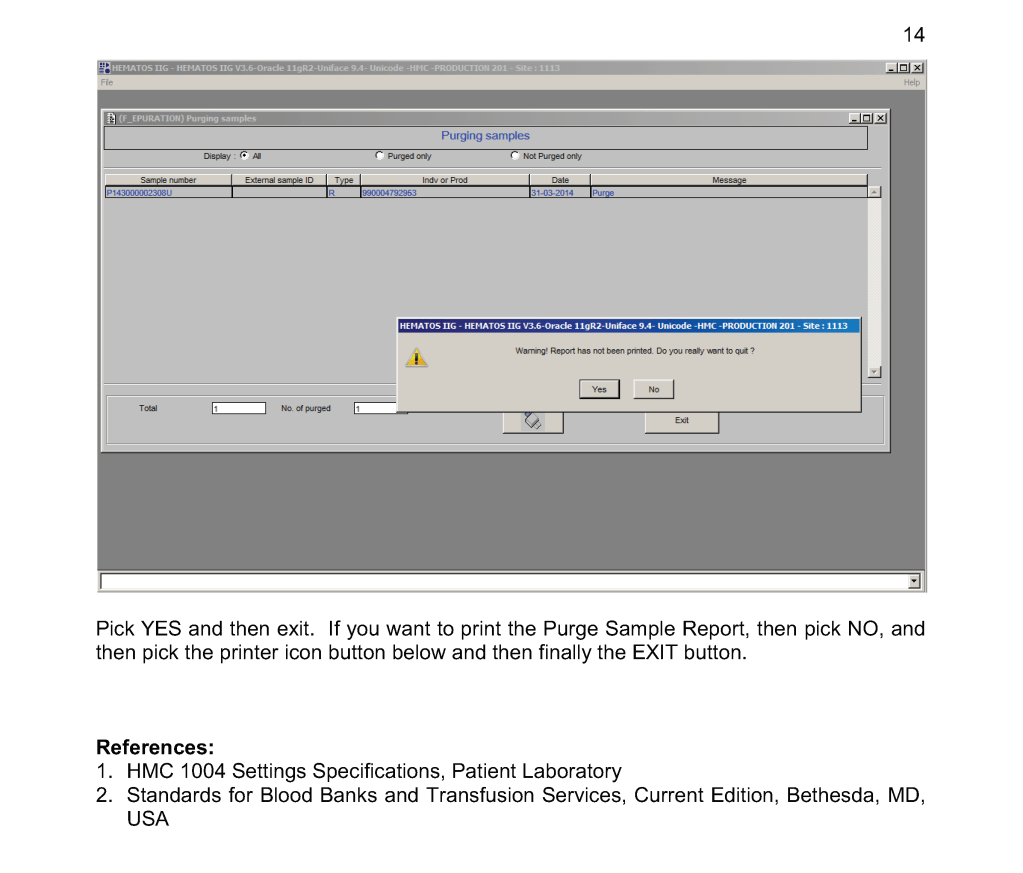
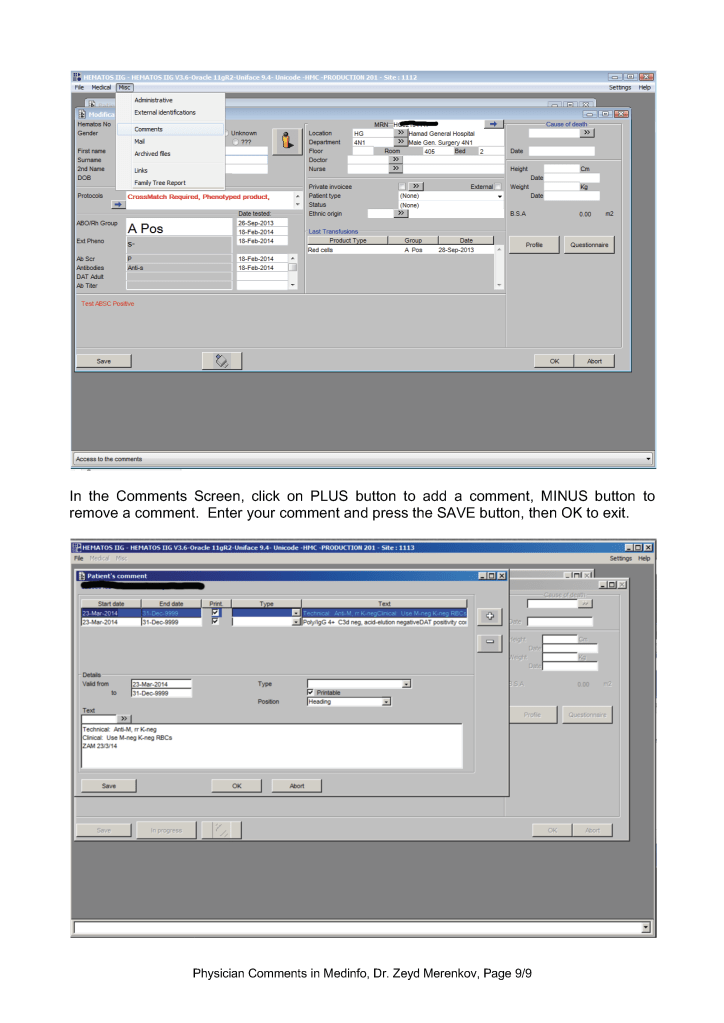
Procedure—Patient Result Comments After Results are Authorized/Verified:
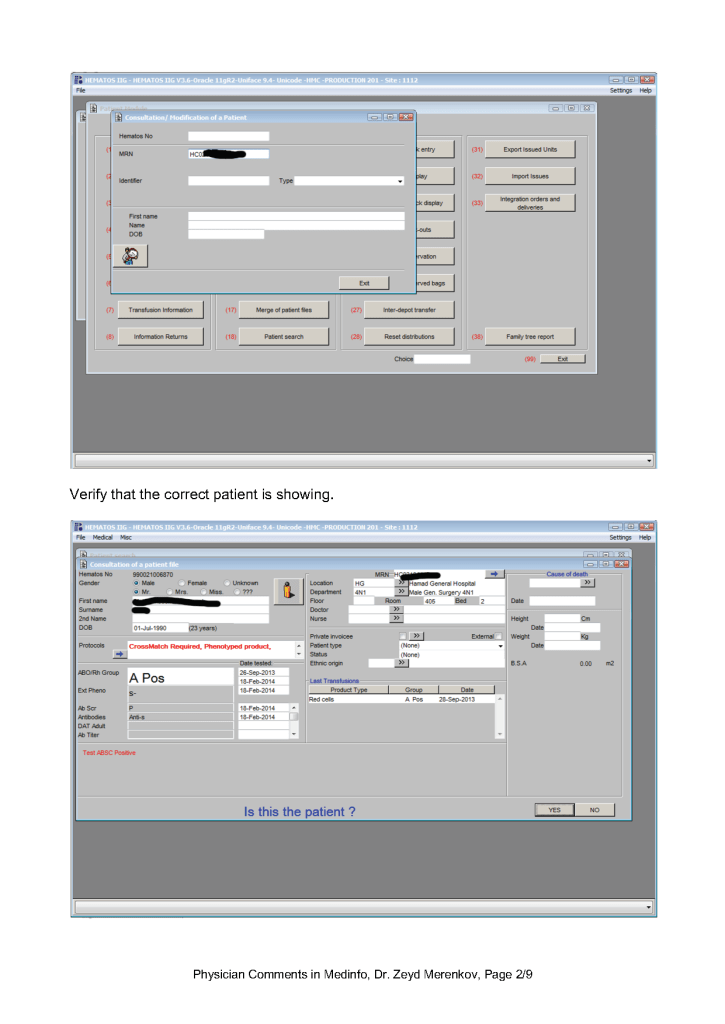
Sign into HIIG and select Patient module, Patient Consultation, and enter the patient hospital HC number.
This post is the policy for using comments in Medinfo software. A subsequent post will show the process of entering comments.
Principle:
There are several different types of comments in HIIG:
Donor Global
Patient Global
Analytical Comments
Result Comments
Contraindication Comments
Global Comments appear on the first main screen of either the donor or patient record. The presence of comments is indicated by a bar at the bottom of the screen (in yellow or blue saying Presence of Comments. Double-clicking opens the list of entered comments.
Examination/Results Comments appear only when you open the result to which it is attached. You must know in advance to which result they are linked to find them.
Contraindication Comments appear when entering a donor deferral code
At HMC, we will enter examination/results comments again as global comments (donor or patient) so it is easy for staff to retrieve them and see them with all other comments. You can do this by cut and paste.
Physicians may enter any of these comment types. Comments may be entered before or after a test is authorized/verified. If entered after authorization, the test must be modified to accept the comment and require a special password (not the user sign-into HIIG). Only results/examination comments are visible in the patient’s medical record. Global, analysis, and contraindication comments are visible only in HIIG! Donor comments are only visible in HIIG.
The presence of comments documents physician review of abnormal results as required by the various accreditation standards.
Policy:
Only designated staff may enter comments.
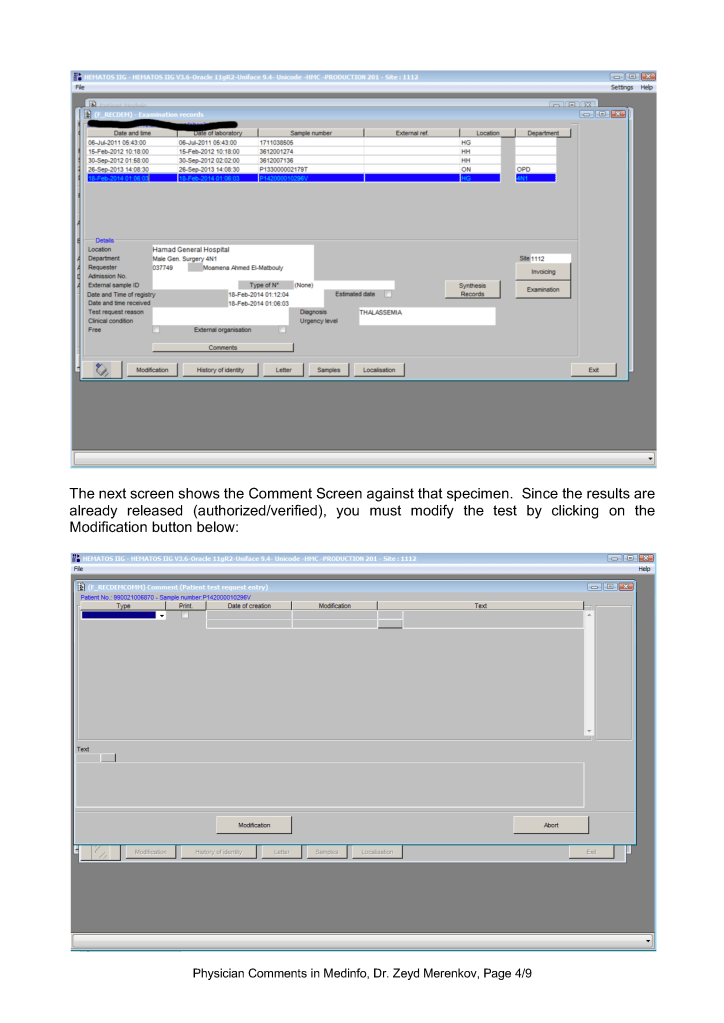
Comments entered after authorization/verification of results will modify the donor/patient record and require a special, high-level password distinctly different from the normal user password.
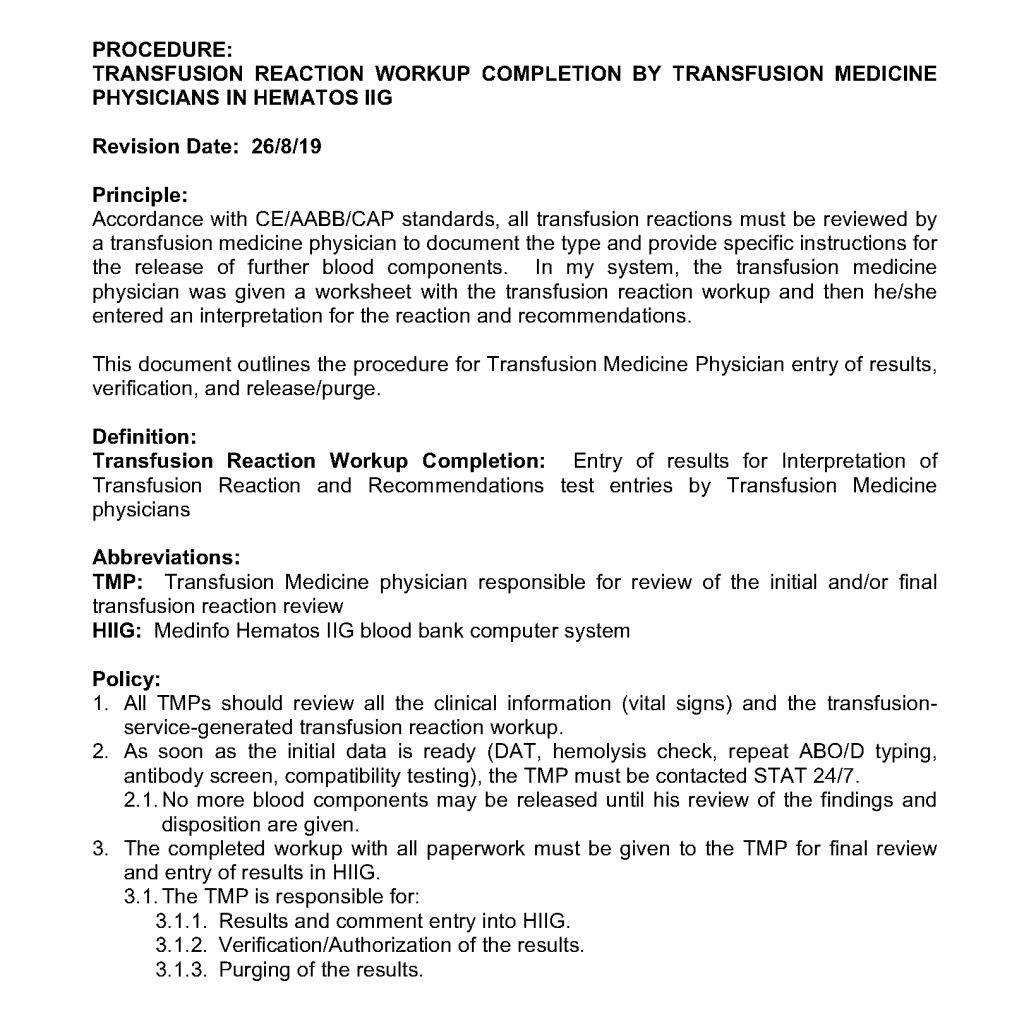
International accreditation standards require physician review of certain abnormal results such as transfusion reaction and antibody workups. This post describes how such review is documented in Medinfo Hematos IIG dedicated blood bank software.
In general there are three main ways to do this:
User ID associated with each transaction
Comments against results, analysis, or globally
Physician direct entry of results (e.g. transfusion reactions)
This applies to all modules of Medinfo, including donor and patient.
User ID:
The system records the User ID of the staff member who performed an action—this includes the authorized transfusion physicians This covers everything in the system, donor or patient. However, it may require a specific query by user ID to list all of that person’s transactions. This is not easy to show an external assessor/inspector unless the query is performed in advance.
Comments:
For those cases requiring review, comments can be placed with the results, which will be visible to anyone viewing that record. Additionally, internal comments can be added to the analysis and globally within the record.
Direct Physician Entry of Results and Interpretations:
For transfusion reaction workups, physicians may directly enter their interpretations and results in the system.
Subsequent posts will show how comments and direct physician entry of results are performed in the system.
In my time at the Saudi National Guard Health Affairs and at HMC Qatar, I offered the pediatric fellows a series of lectures of 1-2 hours duration. The following list has been updated to cover current topics of interest, including COVID-19 convalescent plasma.
Transfusing blood components for physicians—what do you need to know
Recognizing and treating adverse effects of transfusion
Blood components and derivatives—what you need to know
Blood filters, irradiation, aliquoting, and washing blood components
Pathogen inactivation and platelet additive solutions
COVID-19 and the blood supply, COVID-19 convalescent plasma
Indications for blood components and monitoring efficacy
Patient blood management: minimizing transfusions
Blood group serology and compatibility—what you need to know
Adult vs. pediatric transfusion medicine: special considerations for the pediatrics