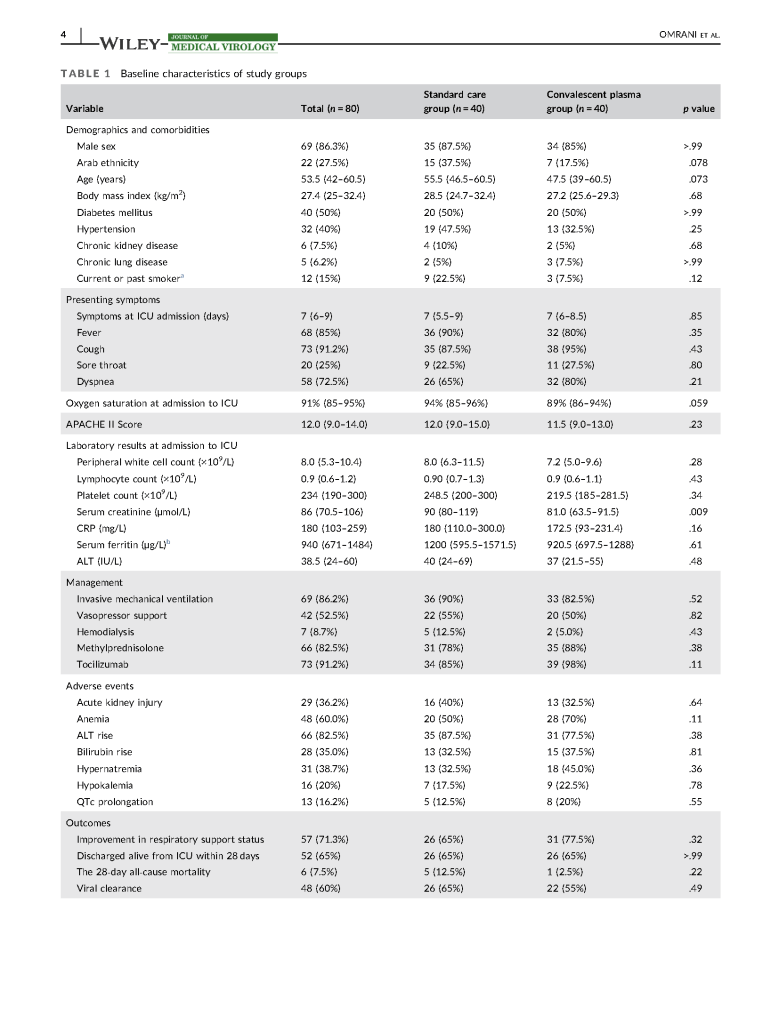
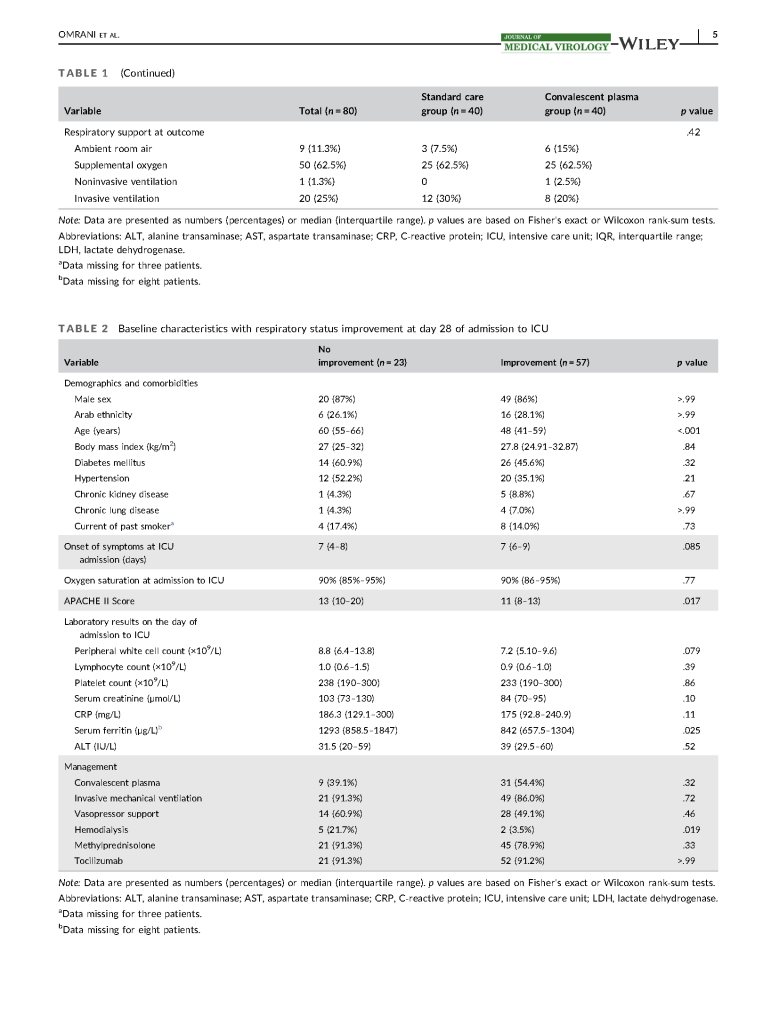
In February 2020, I established COVID-19 plasma collection and distribution for the state of Qatar. Here is a research paper prepared in conjunction with the Qatar Communicable Disease Center about using it for patients there.




Includes therapeutic and donor apheresis
In February 2020, I established COVID-19 plasma collection and distribution for the state of Qatar. Here is a research paper prepared in conjunction with the Qatar Communicable Disease Center about using it for patients there.
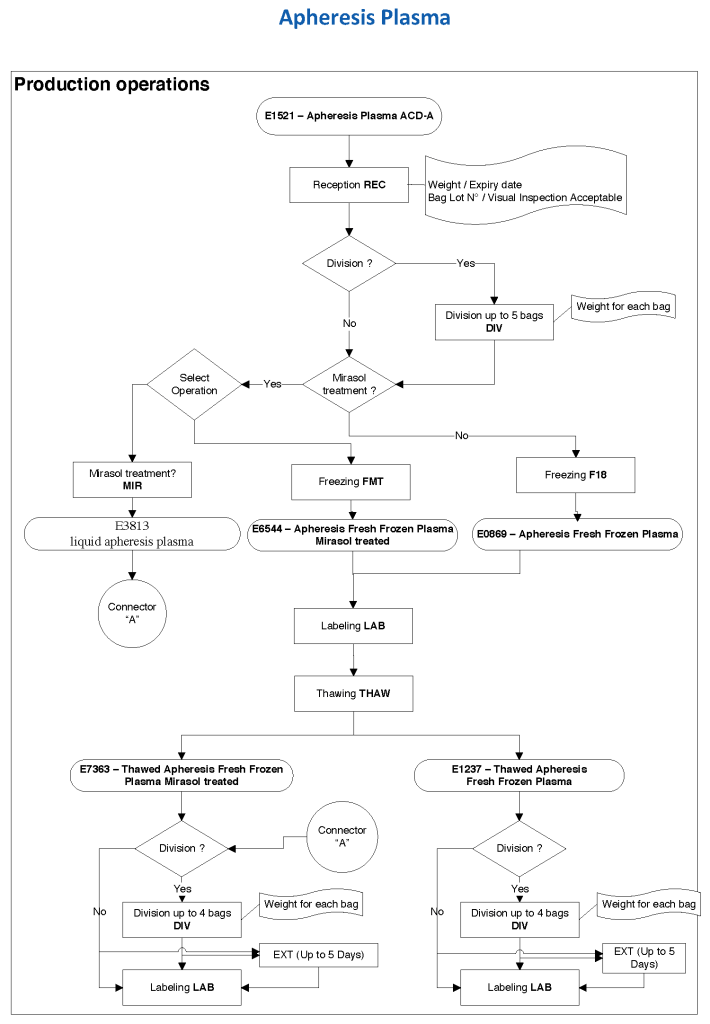
At HMC during my tenure, all plasma products—whole-blood and apheresis-derived were pathogen inactivated with riboflavin (Mirasol). In our software processes, I had options to release both Mirasol-treated and untreated (the latter in emergencies) and to aliquot either as needed. The same processes applied to COVID-19 convalescent plasma CCP except that they were performed in a quarantine production area. There were specific ISBT codes for CCP.
24/9/20
Principle:
Under AABB and FDA rules in the Uniform Donor History Questionnaire, unlicensed, investigational vaccines have a 12-month deferral or as indicated by a responsible physician. In light of the anticipated vaccination trials for COVID-19, this policy gives interim guidance until more definitive information is available.
For COVID-19 Convalescent Plasma CCP donation, investigational vaccine recipients should not donate COVID-19 convalescent plasma until further information is available about their antibody profile.
Policy:
Any donor who has received a COVID-19 (SARS-CoV-2) vaccine will be deferred as follows:
Reference:
Text from the AABB Weekly Report:
Novel Coronavirus Update, Regulatory Update: Investigational Vaccines and Deferral for Donor of Blood and Convalescent Plasma, AABB Weekly Report, 7 August 2020
“FDA recognizes AABB’s DHQ which includes unlicensed (experimental) vaccines on the medication deferral list as a 12-month deferral or as indicated by the responsible physician.
“For routine blood donation, the responsible physician may wish to consider the potential infectious risk associated with the vaccines, and the use of short deferral periods (e.g., 14 days) for live attenuated vaccines and no deferral for non-replicating, inactivated or RNA-based vaccines.
“We agree that no deferral is necessary for routine blood donors who might have received the mRNA-1273 Moderna vaccine.
“At this time, we suggest that individuals who have received a COVID-19 investigational vaccine should not donate COVID-19 convalescent plasma until further information is available about their antibody profile.”
Principle:
New rules have been approved by US FDA CBER for body fluid exposure, tattooing, body fluid exposure, and body-piercing. By similar logic we will extend this also to HIJAMA. We will not make any changes to our sexual history/practices or history of sexually transmitted disease treatment.
Policy:
Reference:
Revised Recommendations for Reducing the Risk of Human Immunodeficiency Virus Transmission by Blood and Blood Products, Guidance for Industry, U.S. Department of Health and Human Services, Food and Drug Administration, Center for Biologics Evaluation and Research, April 2020
Principle:
Kidneys have strong expression of ABO type and must be matched the same way as RBC components. In the case of ABO-incompatible renal transplants, we must not give significant amounts of plasma incompatible to the ABO type of the donor kidney. Plasma must also be compatible with the patient’s ABO type for RBC transfusions. The amount of residual plasma in PRBCs is limited since we use an additive solution SAGM. Likewise, platelet components are suspended in platelet additive solution with only minimal residual plasma. Cryoprecipitate has only minimal plasma and is given without regard to the patient’s ABO type.
Policy:
References:
This is a policy I made for NGHA Jeddah many years ago but is still useful today.
Principle:
All technical staff are required to read and understand the manufacturer package inserts that apply to the procedures that they perform. This policy establishes a means of documenting compliance with this requirement.
Policy Details:
Insert Review Form
| Type of Insert: New Revised |
| Product Name: |
| Date of Insert: |
I have read this insert and understand its contents and accept responsibility for following its instructions and directions.
| Staff Name & Badge #–PRINT! | Signature | Date |
Reading Assignments:
Study Questions:
Revised:
29/8/20
Objectives:
Clinical Responsibilities (after proven competence):
Assessments:
Working Hours:
Reviewed 17/8/20
Transfusion Medicine TM:
Cellular Therapy Laboratory:
Most Responsible Physician:
Ward/Clinic Nursing Responsibilities:
Note:
Principle:
All therapeutic apheresis procedures are potentially life-threatening and must only occur by an order from a transfusion medicine physician with experience/competence in such procedures.
Definitions:
Policy:
References:
