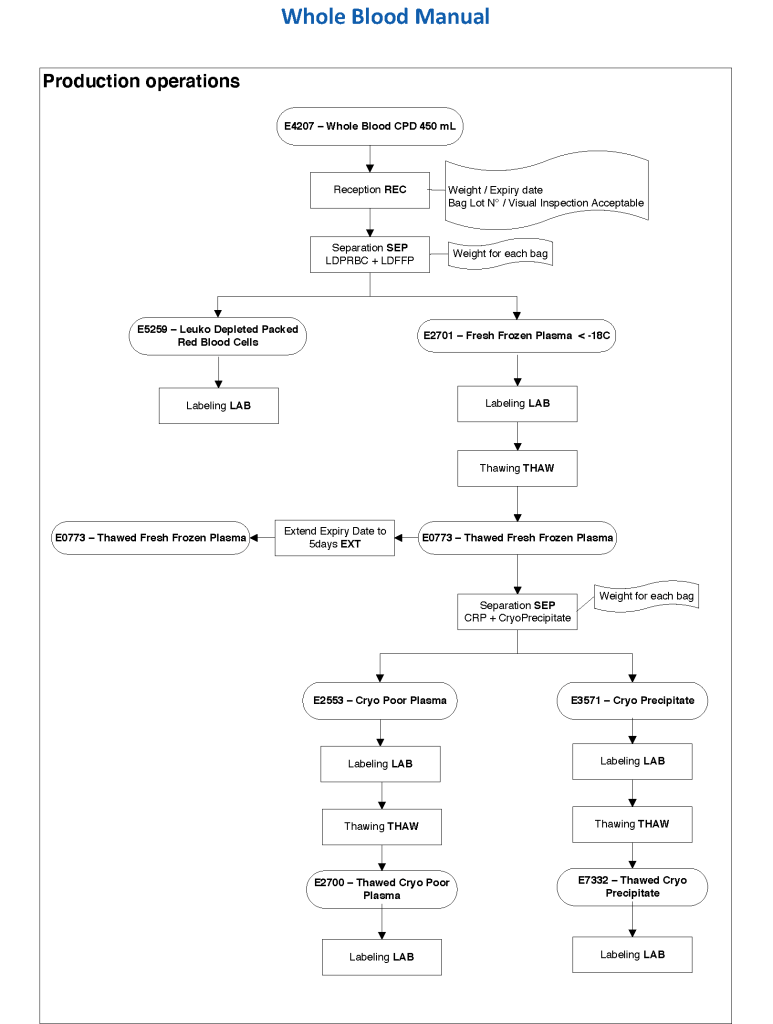
This was the HMC methodology for manual whole blood processing to prepare packed RBCs, plasma, cryoprecipitate, and cryo-poor plasma using blood bank centrifuges (not Reveos). It did not include preparing platelets since we did not have manual buffy coat processing equipment. In this algorithm we did not specifically release whole blood as a final product (although we did have the capability of activating this in emergency situations).
Maintaining an adequate blood supply and expedited compatibility testing are critical in disaster planning. This plan is assuming that the Blood Donor Center is functional and can process donors and make components.
Medinfo Hematos IIG System is critical to monitoring inventory, preparing blood components expeditiously using Good Manufacturing Processes, and distributing blood components in a timely controlled manner.
Policy:
Determinate total available blood supply across all locations by using the Cumulative Stock Display program in Medinfo Hematos IIG.
Recheck stock at least every hour during the disaster.
At each transfusion service site, in conjunction with the Transfusion Medicine Consultant:
Cancel reservations for elective surgical and non-emergency medical cases of affected ABO/D types.
Retain reservations for antigen-matched, oncology, NICU, and high-risk obstetrical cases.
Inform Manager for Donor Recruitment/Logistics to send SMS, radio, and television messages for blood donors—all types.
Contact ALL staff and have them report to duty.
At Blood Donor Center, the Head Nurse, Recruitment Manager, Supervisor, Component Processing, and Supervisor, Marker Testing will contact their respective staff.
At various hospital blood bank transfusion services, the site supervisor will contact all staff.
Process blood components using automated component technology (Reveos).
Perform all donor marker testing including single-well NAT.
Abbreviation of donor testing is only at the discretion of the Head, Transfusion Medicine.
Send blood components using Inter-Depot Transfer function of Medinfo.
Transfusion Services:
Release blood component according to the various protocols as needed:
Massive transfusion protocol
Emergency release
STAT
Priority
Routine
Compatibility testing will be electronic, immediate-spin, or full AHG as per our protocols.
References:
Standards for Blood Banks and Transfusion Services, Current Edition, AABB, Bethesda, MD, USA
Guidelines to the Preparation, Use, and Quality Assurance of Blood Components, European Committee (Partial Agreement) on Blood Transfusion (CD-P-TS), Current Edition
As a transfusion medicine physician, I must know if I can trust my staff’s interpretation of immunohematology testing. I may be called at night and they will provide me with results and I must use these to make a medical judgment. If their interpretation is flawed, I might make a decision that harms the patient.
I really don’t like multiple-choice questions, but nowadays this is often the norm. For my staff, especially senior staff and those who want to be promoted to senior staff, I have developed a series of projective exercises to help me understand their thought processes.
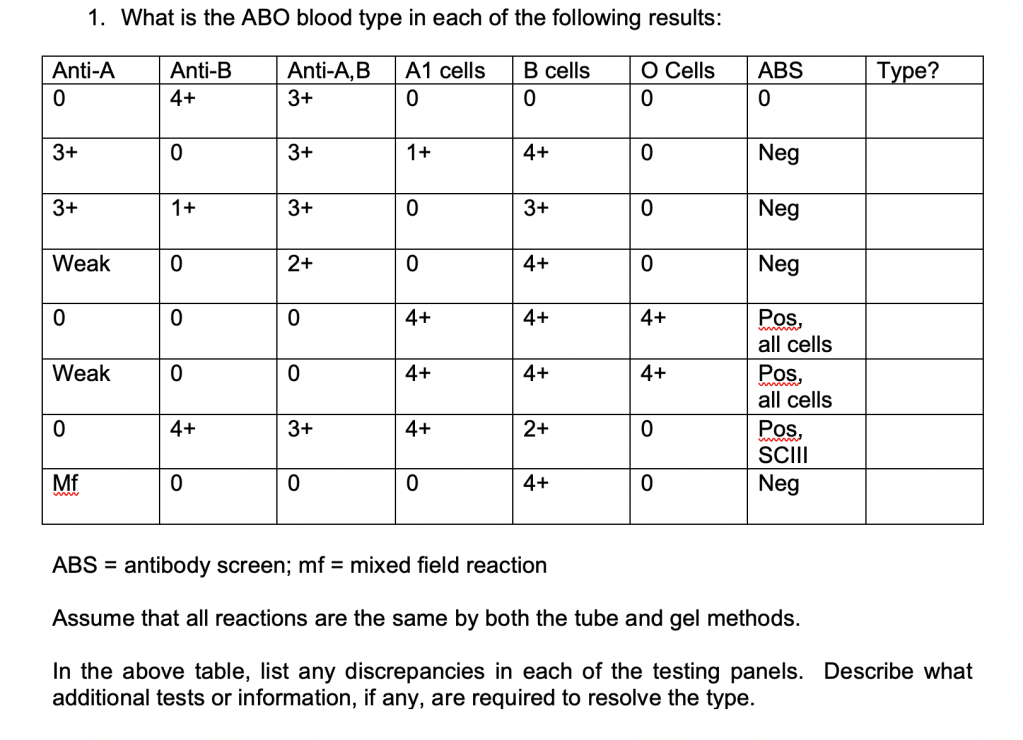
Here is another series of exercises, usually given to advanced technologists and supervisor candidates. I want them to tell me what they need to assess each scenario. Can they definitively diagnose solely on the information provided?
These are open-ended and may have more than one possible interpretation:
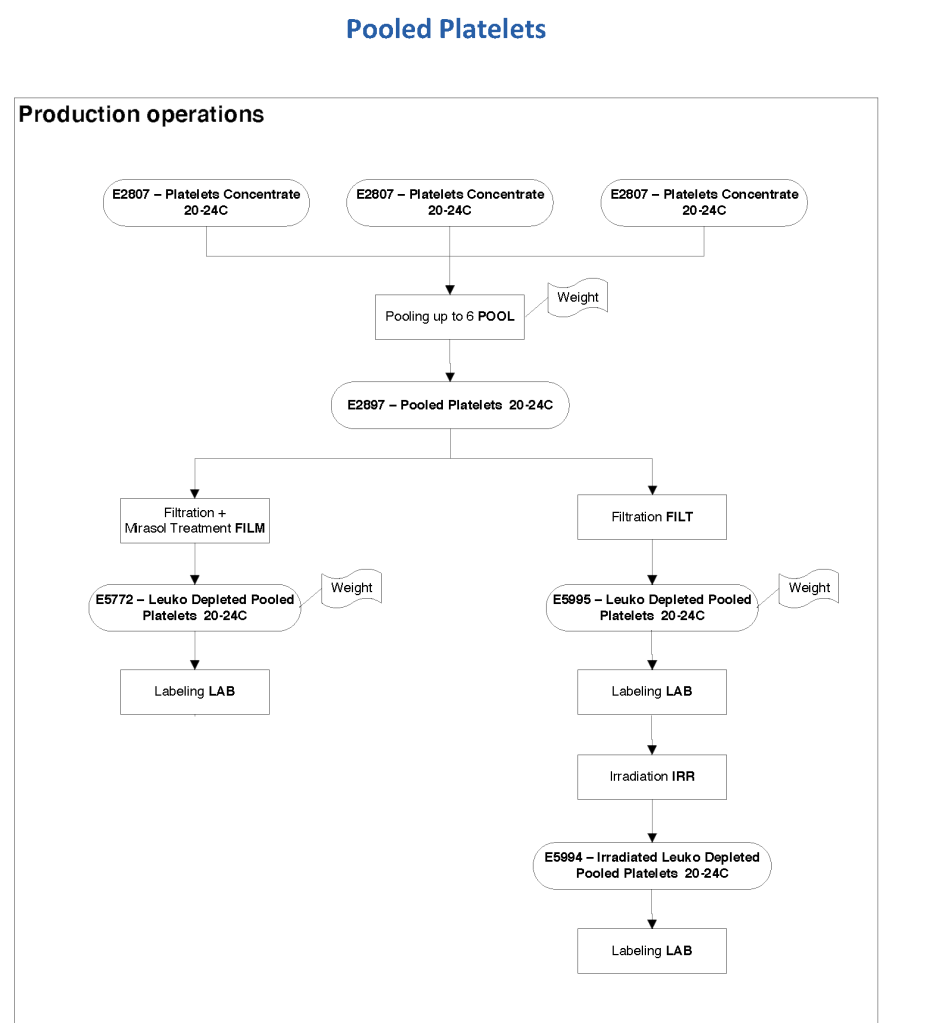
Outside the USA, platelet pools stored at room temperature may be valid for up to 7 days, especially if pathogen-inactivation is used. The following workflow shows both Mirasol pathogen-inactivated and standard platelets. The standard platelets are then irradiated. Both types can be aliquoted.
A major advantage in using a specific blood bank computer software is to enforce the Good Manufacturing Process. Medinfo is merciless: there are no exceptions without authorization and that is restricted by the security policies.
In the recent Reveos post, the upper and lower platelet volume specifications were discussed. The platelets are weighed and the volume is calculated. If a manual or another method for preparing platelets is used, then the according values can be specified.
HMC Blood Donor Center is implementing a policy to limit or help limit iron deficiency in its blood donors (whole blood and/or apheresis). The reasons for this are:
Development of iron deficiency in some donors
Progression of iron deficiency that occurs with frequent blood donation
Potential adverse effects of iron deficiency
Definition:
Donors high-risk for iron loss include:
Females—all, regardless of age
Males donating three or more times within a 12-month period
Apheresis donors giving 5 sessions in an 8-week period
Donors after one RBC apheresis dual-unit donation
Males and females with borderline low hemoglobin levels:
Males with hemoglobin <= 13.5 g/dl
Females with hemoglobin <= 13.0 g/dl
Donors with low ferritin level (below current lower limit of reference range)
Policy:
Donors will be provided with information regarding iron-deficiency from donation.
High risk donors (as defined above) will be offered a prescription for iron supplementation equivalent to 18 mg of elemental iron daily for 30 days.
During the iron supplementation period, the donor will be deferred for donation.
If a donor does not take the iron supplement, then he/she is limited to 2 donations/year.
We will offer donors to test ferritin in the following categories:
Apheresis donors after their fifth donation of plasma or platelets within 8 weeks
Whole blood donors after three donations within a 12-month period
Donors after dual-unit (2-unit) RBC apheresis donation
All female donors otherwise meeting donor criteria before donation
Donors with low ferritin levels will be deferred until ferritin levels are normal (based on reference range currently in effect)
References:
AABB Association Bulletin #17-02, Updated Strategies to Limit or Prevent Iron Deficiency in Blood Donors, 26/3/17
Normally, outside donor campaigns still connect to the main server via wireless 4G/5G with a VPN. However, if there is a “dead” spot, Medinfo can provide a local area network using one of the PCs/laptops to serve as a server. The local server receives an uploaded image of the donor database. Upon return to the donor center, the local server’s data is uploaded and synchronized.
When you cannot establish a direct link to the live Medinfo program, you must arrange for Medinfo/VHT to create a local server that will have the current Medinfo donor database for use at outside campaigns where the internet connection cannot be used. This can also be used if for some reason the Blood Donor Center link is down in order to register donors and check the donor deferral database.
Policy:
For each outside campaign, there should be a pre-campaign visit to verify the availability of internet to connect to Medinfo.
If the internet connection is working, use Medinfo using the 4G/5G access points. Otherwise:
If none, inform Medinfo/VHT to prepare a local server—at least ONE DAY in advance of the campaign.
Provide Medinfo/VHT one of the portable computers to download the database and software. This will be the offline server for the campaign.
Link the offline server to the other portable computers for the campaign (see the corresponding Medinfo job aid).
Use the local network (offline server and other portable computers) for registering donors.
Upon return to the Blood Donor Center, upload the data as indicated in the Medinfo job aid.
This is a policy I made for NGHA Jeddah many years ago but is still useful today.
Principle:
All technical staff are required to read and understand the manufacturer package inserts that apply to the procedures that they perform. This policy establishes a means of documenting compliance with this requirement.
Policy Details:
Technical staff are defined as anyone who uses the reagent in the performance of a procedure or process or anyone reviews or supervises that process or procedure. This includes the supervisor, medical technologists, medical technicians, nurses, phlebotomists, and assistants.
All technical staff are required to read and understand ALL product inserts for each procedure applicable to the section(s) that they work in—apheresis, donor room, component preparation, and/or transfusion service.
If they have any questions about a particular insert, they should refer it to the supervisor, senior technologist (Med Tech 1), or in the latter’s absence, the blood bank medical director/section head.
Each staff member must sign the Manufacturer’s Package Insert Review Form for that particular policy/procedure, including his signature, employee identification number, and date.
Each Manufacturer’s Package Insert Review Form will be retained with a copy of the package insert by the Blood Bank Supervisor in a special file while the material is being used and for at least five (5) years after a new or revised manufacturer package insert is applicable.
A new Manufacturer’s Package Insert Review Form should be used for each revision of the insert.
Insert Review Form
Type of Insert: New Revised
Product Name:
Date of Insert:
I have read this insert and understand its contents and accept responsibility for following its instructions and directions.
As a transfusion medicine physician, I must know if I can trust my staff’s interpretation of immunohematology testing. I may be called at night and they will provide me with results and I must use these to make a medical judgment. If their interpretation is flawed, I might make a decision that harms the patient.
I really don’t like multiple-choice questions, but nowadays this is often the norm. For my staff, especially senior staff and those who want to be promoted to senior staff, I have developed a series of projective exercises to help me understand their thought processes.
Here is another exercise, usually given to physicians. I give them the following scenario:
There is a major trauma on an unidentified young adult male patient. We do not know the transfusion, medical, or medication history. They need six units RBCs STAT.
What blood type do you select? How do you release the blood?
You give the 6 units and receive a specimen back. The patient’s typing reactions are:
Forward type: Anti-A, anti-B both negative
Reverse type: 4+ reaction with A1 and B cells
About 15 minutes later, your technologist tells you that the antibody screen is 4+ in all cells and all panel cells react 4+ both at AHG and enzyme phases. What do you tell the treating clinician? What do you do?
The technologist in panic has been performing AHG crossmatches but all 4+ incompatible.
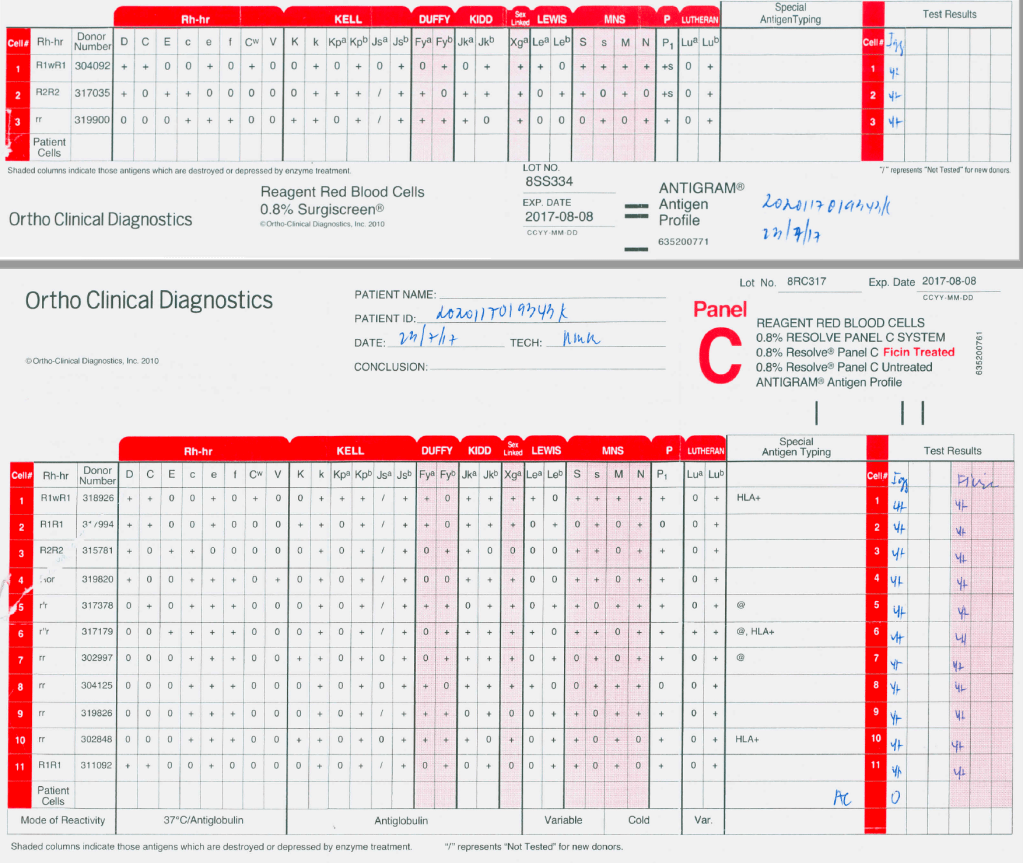
Here is the panel:
I have them review this panel and tell me to interpret it
What further testing would you do, if any?
What blood type do you release now?
What is the significance of the negative autocontrol when there is panreactivity?
What if the enzyme panel results are all negative?
What if the autocontrol is 4+?
The smart ones will ask for a full extended phenotype (e.g. Diamed/Biorad’s three profile cards) and for anti-H.
I tell them the clinician is very angry and demands you release more group O blood immediately? How do you respond?
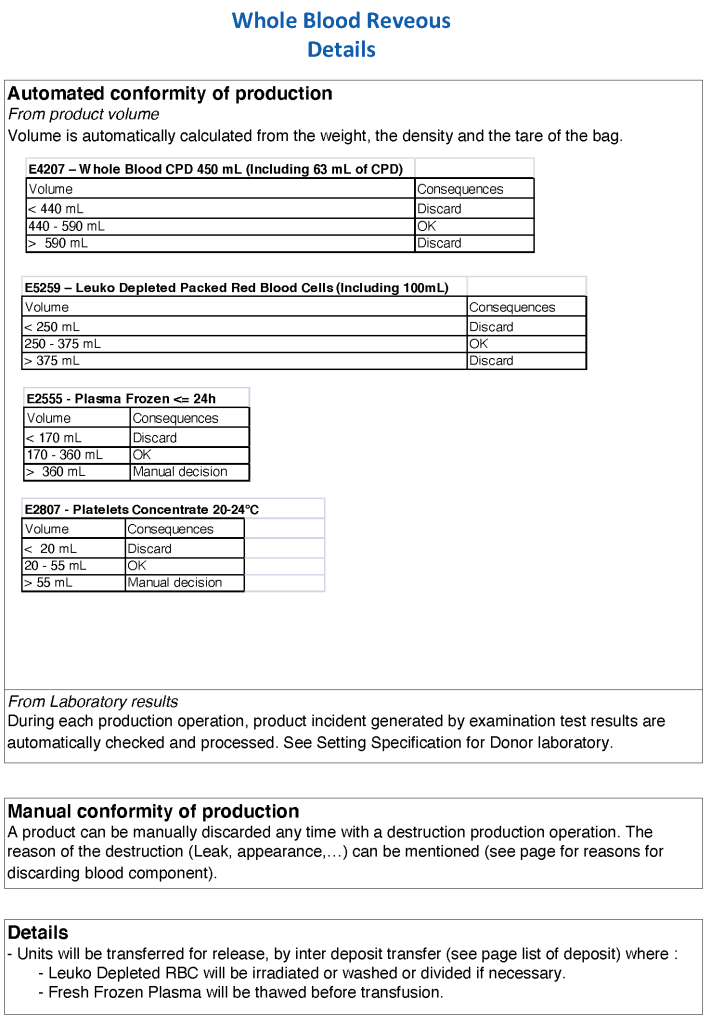
A major advantage in using a specific blood bank computer software is to enforce the Good Manufacturing Processes. Medinfo is merciless: there are no exceptions without authorization and that is restricted by the security policies.
The following tables show the values established at HMC Doha during my tenure. These values were recommended by the Terumo BCT Reveos engineer after his direct, hands-on set-up of the equipment.
The minimum and maximum volumes for platelets are specifically designed to work for pooling the buffy coats before Mirasol pathogen inactivation. There are different settings for platelets suspended in plasma versus those suspended in platelet additive solution PAS.
Similarly, there are specific volume ranges for plasma so that pathogen inactivation can be performed according to Terumo BCT recommendations.