If there is strong antibody binding to an RBC, this may interfere with a typing reagent attaching to the cell and cause a false-negative, i.e. a “blocking” antibody. Such cells may interfere with the indirect antiglobulin test IAT, i.e. the antibody screen. The autocontrol and direct antiglobulin test DAT will be strongly positive.
The manufacturer’s instructions should be strictly followed for using its reagents in the presence of a strongly positive DAT. If there is no reaction with the typing reagent, the result must be indeterminate.
One could try a (relatively) nondestructive elution method such as gentle-heat elution to remove some of the antibody and then retype the cells. I have found this to be a simple and effective method for my staff to use. Just remember that despite being “gentle,” there will still be some hemolysis present, but here it is the cells we are trying to save.
Usually, we find this situation in a neonate born of a mother with anti-D. The baby has a strong DAT but the D typing is negative. Check the D control carefully: if it is positive, the result is indeterminate, try another method. Usually gel/glass bead methods are subject to less interference. Finally, there is always the classic saline anti-D!
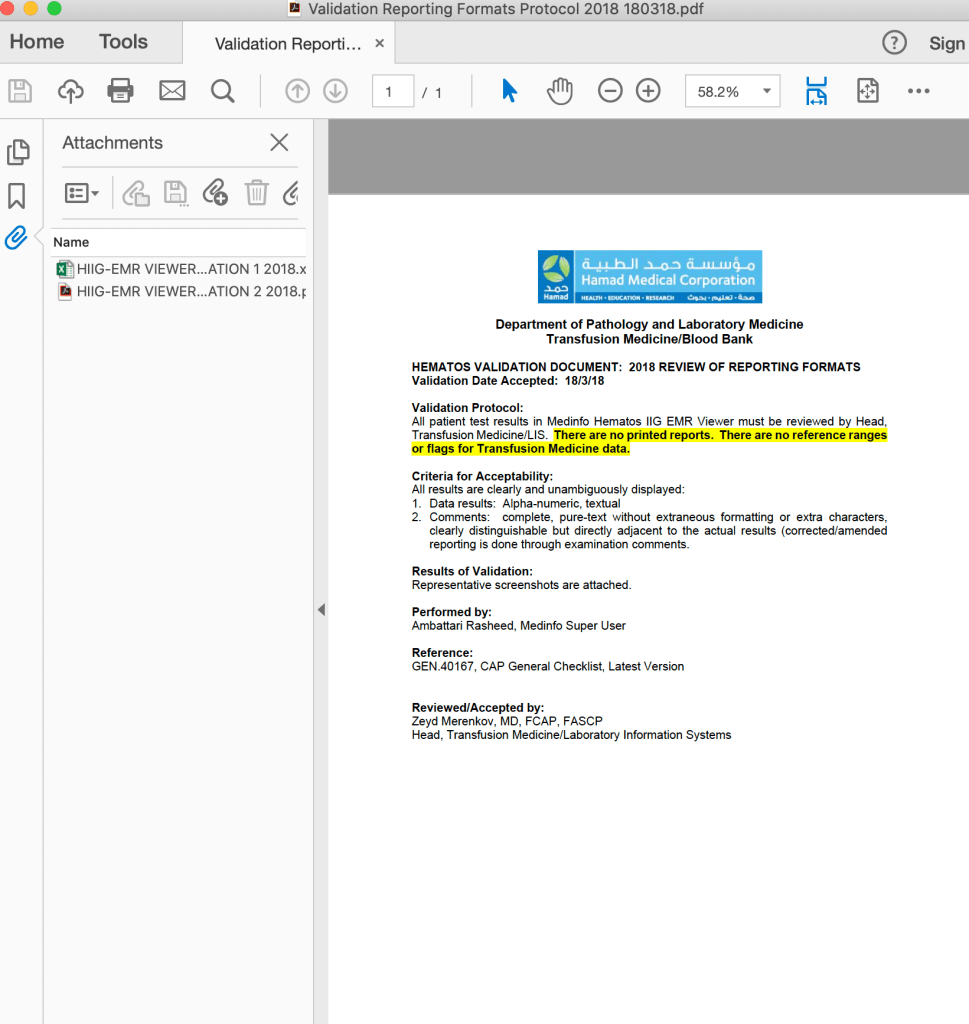
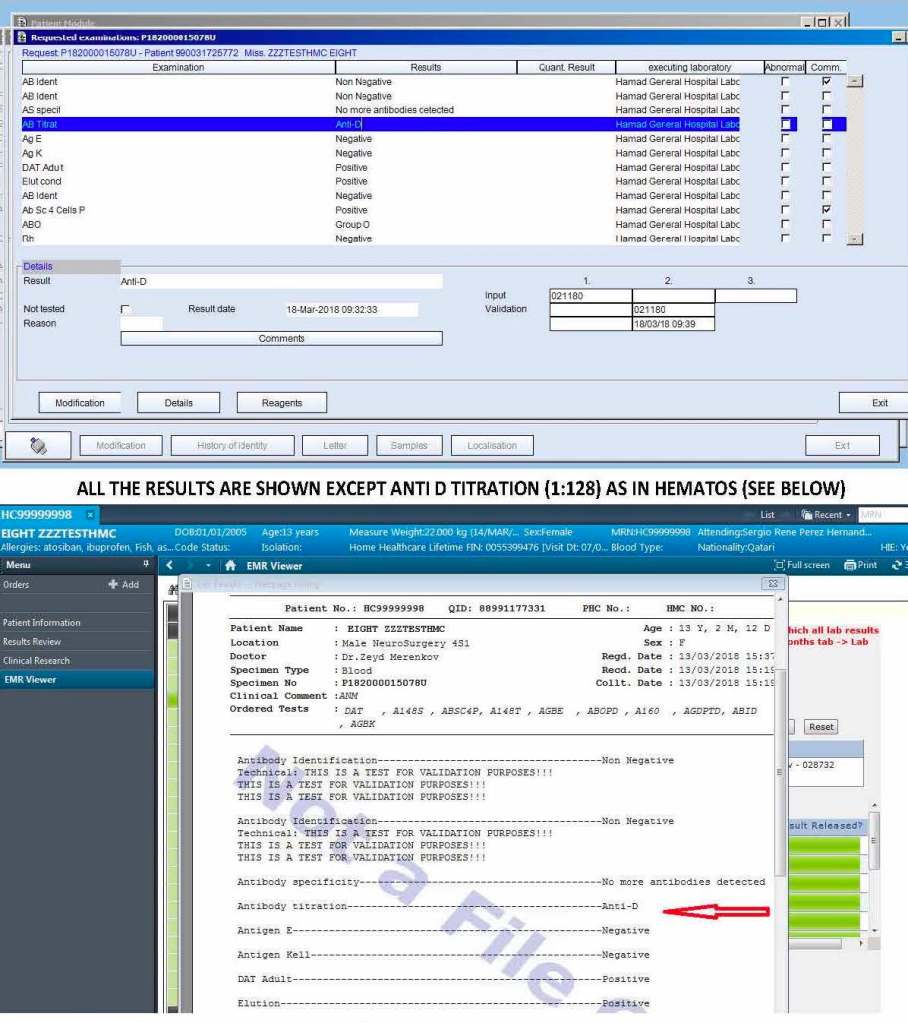
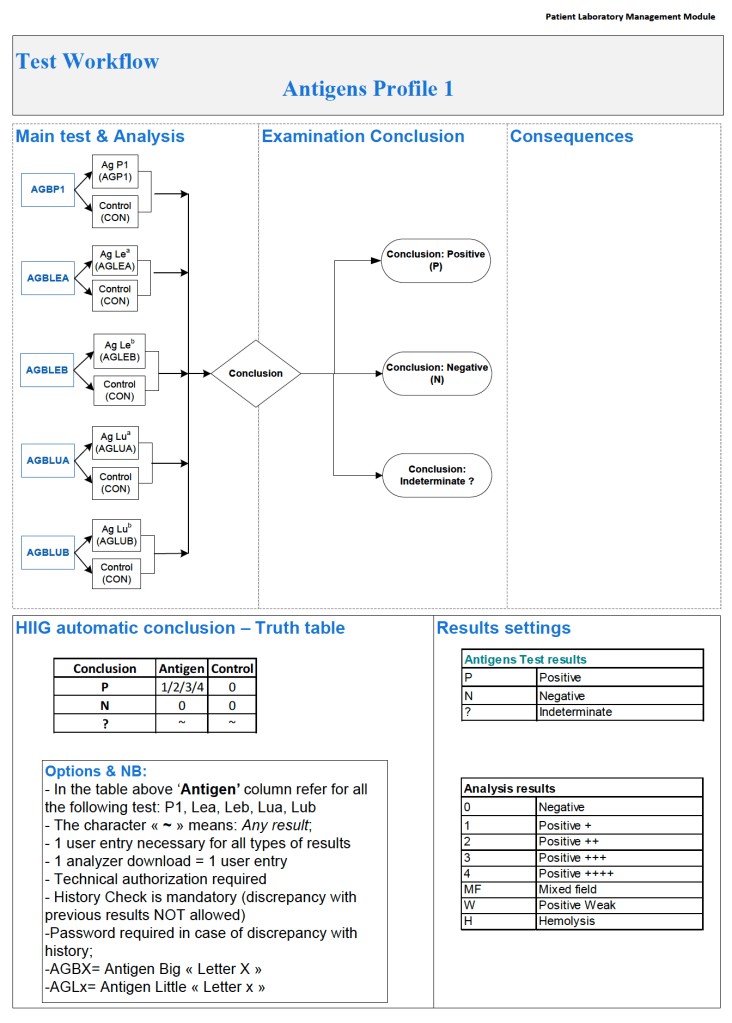
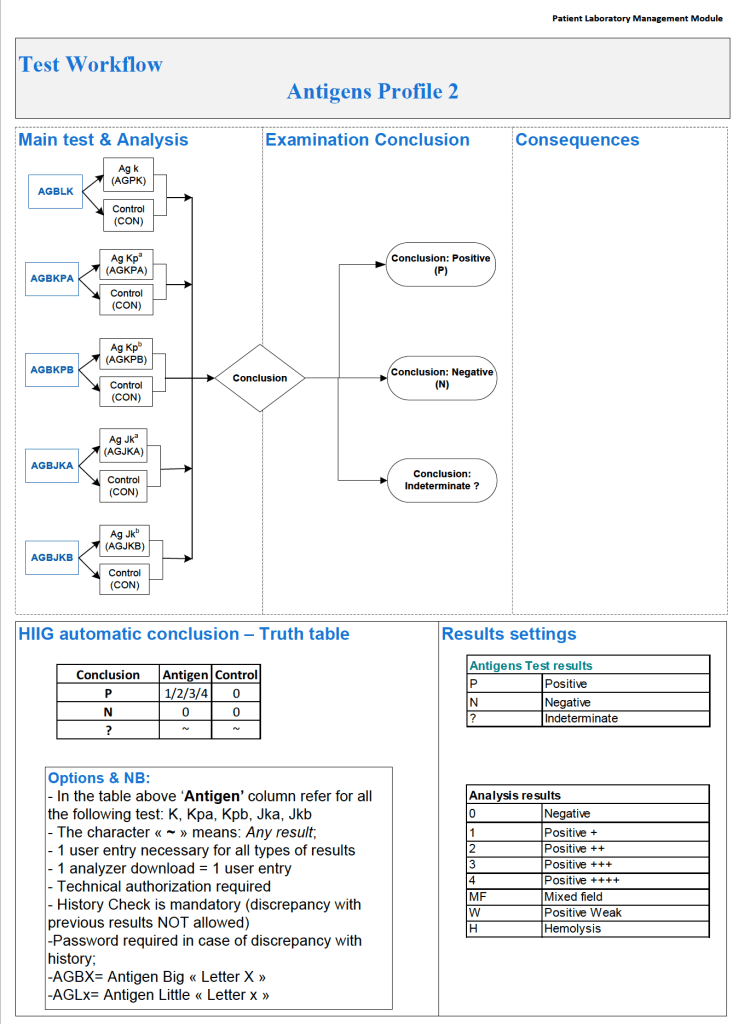
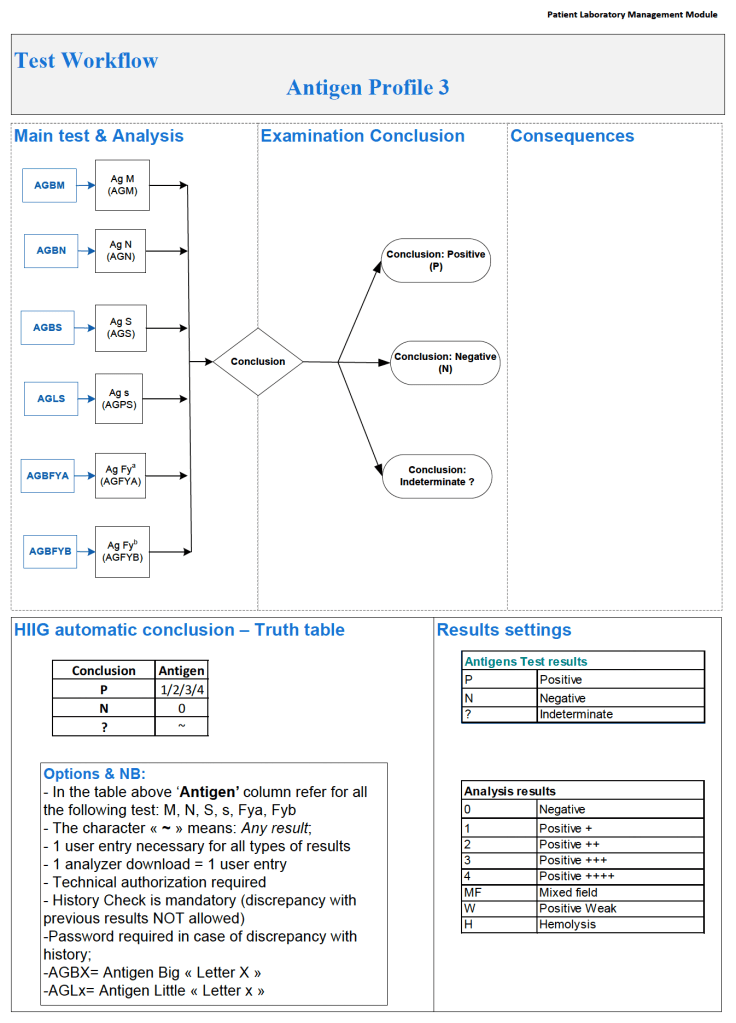
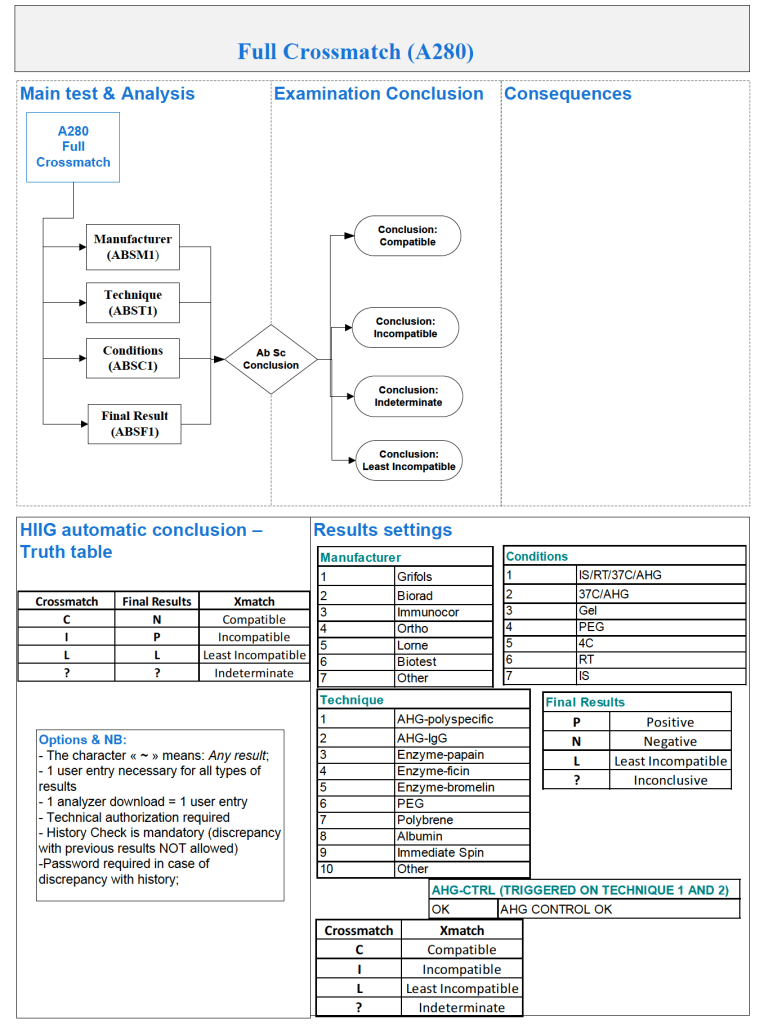
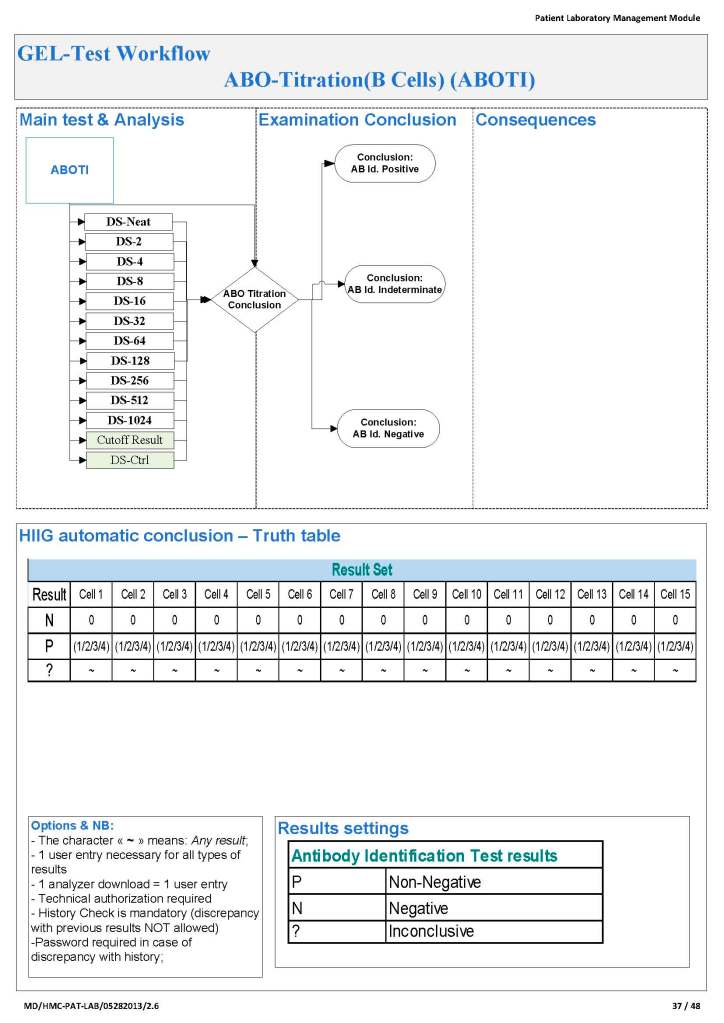
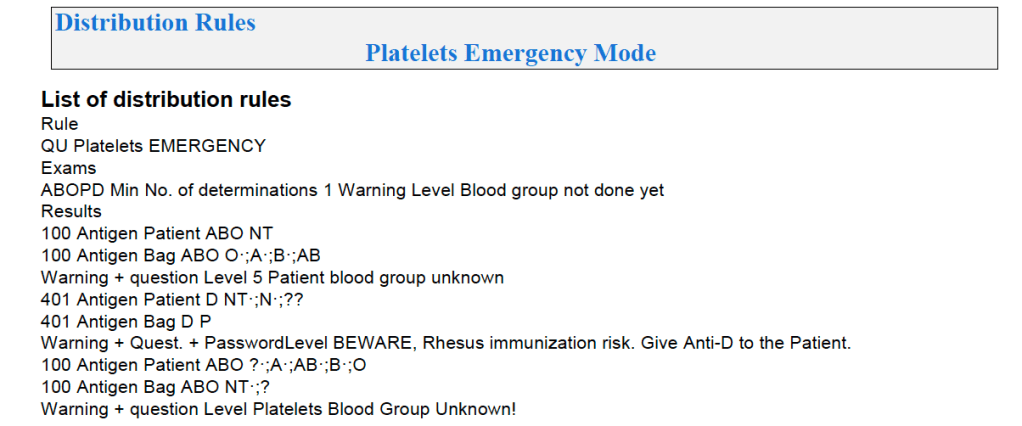
In Medinfo software with a blocking antibody, a nonnegative control will trigger a manual review of the results. There will be no automatic release.
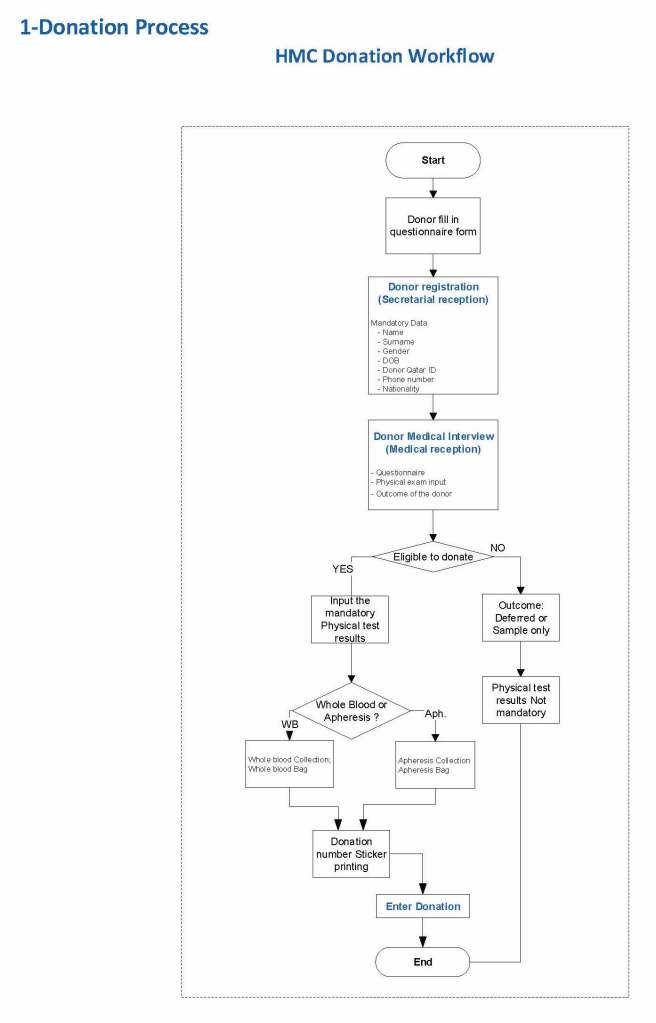
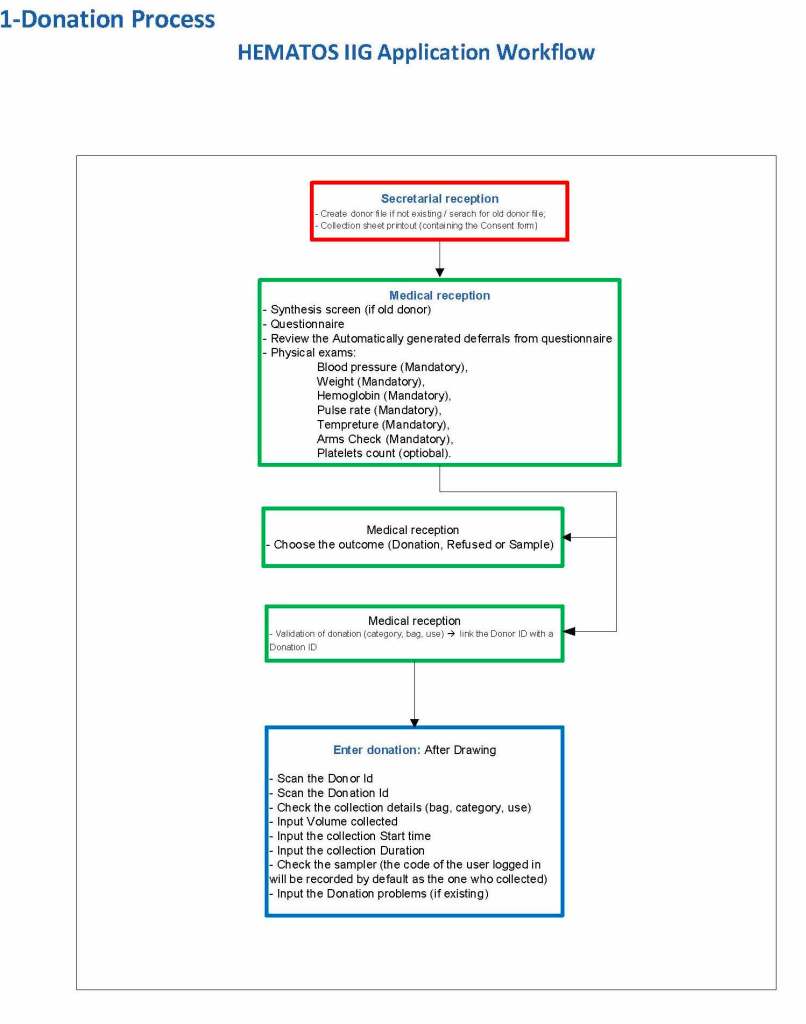
Here is my process for handling blocking antibodies, which I set up for HMC Doha:
INTERIM POLICY: ANTIGEN TYPINGS IN PRESENCE OF STRONGLY POSITIVE DIRECT ANTIGLOBULIN TEST (DAT): RULE OUT BLOCKING ANTIBODY
Principle:
Antigen typing of cells with large amounts of coating antibody (i.e. strongly positive DAT 3-4+) may not always be possible because the bound antibody may block available antigen sites. This policy is to clarify how to recognize and handle such situations.
Policy:
- Always follow the manufacturer’s instructions for the use of the typing reagent.
- In particular, note whether a control must be run with the test (e.g. D-control, D-diluent, etc.) or if it is included in the gel or glass bead card.
- If a control is required, use exactly what the manufacturer recommends.
- DO NOT SUBSTITUTE ANYTHING ELSE AS THE CONTROL!!
- In particular, note whether a control must be run with the test (e.g. D-control, D-diluent, etc.) or if it is included in the gel or glass bead card.
- Interpret the reactions exactly as the manufacturer indicates.
- If the test is invalid because of the control or any other reason, report the antigen typing as indeterminate and send for Transfusion Medicine Physician review.
- If the DAT is 3-4+ and the antigen typing shows no reaction (apparent negative), send the case to the Transfusion Medicine Physician for review and final interpretation. DO NOT ENTER THE RESULT AS NEGATIVE UNLESS THE TMP INSTRUCTS YOU TO DO THIS!!
- To rule out a blocking antibody, a special elution to gently remove the coating antibody may be needed so that the RBCs can then be typed (not acid glycine technique—rather, gentle heat elution.) The Transfusion Medicine Physician will decide whether to do this additional testing.
References:
- Standards for Blood Banks and Transfusion Services, Current Edition, AABB, Bethesda, MD, USA
- Technical Manual, Current Edition, AABB, Bethesda, MD, USA
- Guidelines to the Preparation, Use, and Quality Assurance of Blood Components, European Committee (Partial Agreement) on Blood Transfusion (CD-P-TS), Current Edition