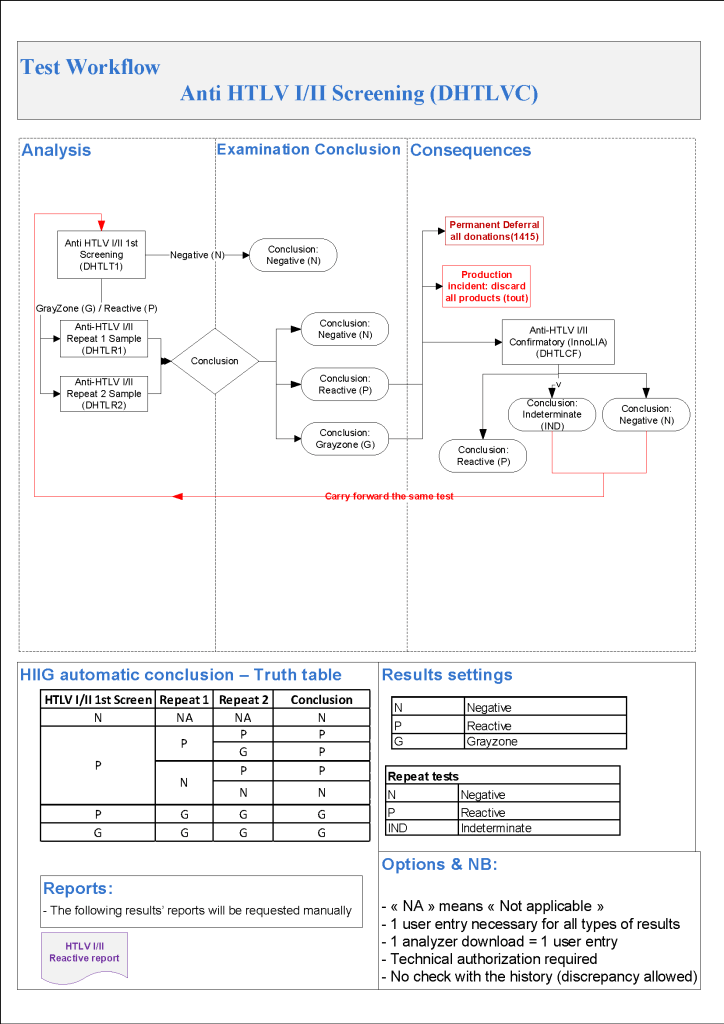
As I designed in Medinfo, this is a much simpler algorithm than HCV and uses an HTLV-1/HTLV-2 screening test and a confirmatory linear immunoblot assay LIA that can discriminate between type 1 and type 2. If there is an indeterminate result, a repeat test is ordered after 6 months:
HTLV 1/2 Testing:
HTLV Antibodies positive, then do HTLV-InnoLIA:
HTLV InnoLIA positive for HTLV-1 and/or HTLV-2: refer to Infectious Disease clinic
HTLV InnoLIA indeterminate or negative, repeat HTLV Ab and HTLV InnoLIA testing after 6 months
Repeat HTLV Testing After 6 Months:
HTLV 1/2 antibodies positive, permanent deferral and do HTLV InnoLIA
HTLV 1/2 antibodies indeterminate, permanent deferral and do HTLV InnoLIA
HTLV InnoLIA positive for HTLV-1 or HTLV-2: refer to Infectious Disease clinic
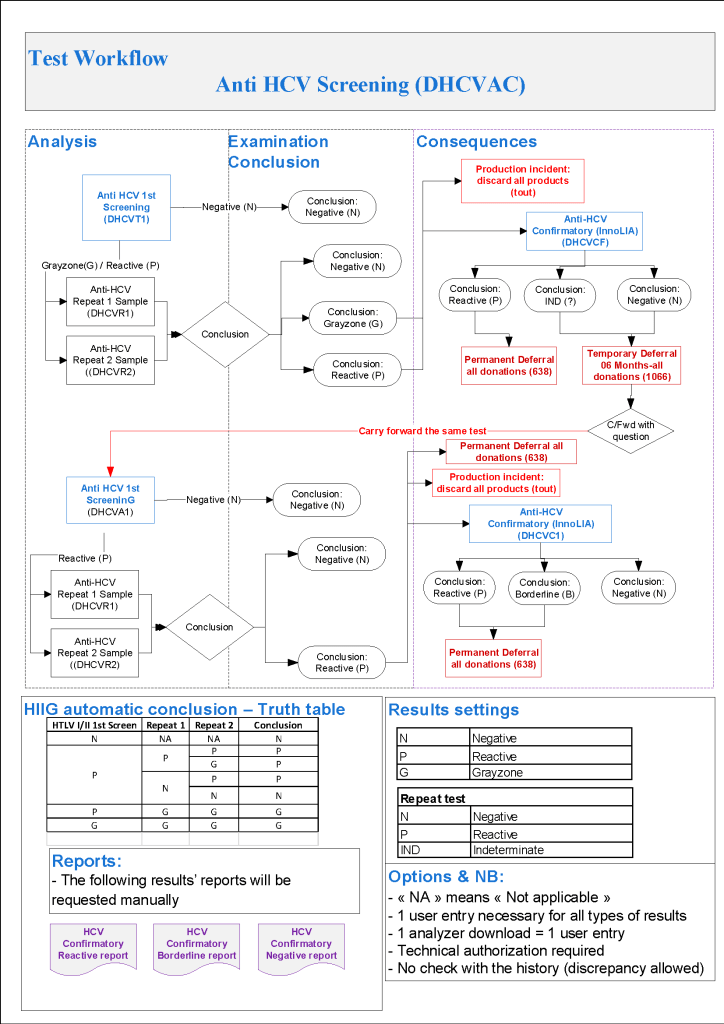
The testing algorithms may trigger additional testing, repeat of current testing at some future date, or permanent deferral. One of the most complex processes is for HCV testing. The following criteria are based on US FDA CBER guidelines, but are modified for the availability of test methodologies not licensed in the USA.
For HCV, we use the following testing in all donors:
HCV antibody EIA
HCV NAT
If any of the tests are non-negative, then we do the HCV LIA immunoblot assay.
HCV LIA is more sensitive than RIBA-3 (now no longer performed in the USA) but is not available in the USA. This test has been incorporated into the testing algorithm from CBER:
Hepatitis C:
HCV-RNA positive confirmed, regardless of other HCV results: permanent deferral, refer to Infectious Disease clinic
HCV-RNA borderline: repeat all HCV testing after 6 months
HCV-InnoLIA positive, regardless of other HCV results: permanent deferral, refer to Infectious Disease clinic
HCV-InnoLIA indeterminate: repeat all HCV testing after 6 months
HCV-Ab positive, HCV-RNA negative, do HCV-InnoLIA:
If HCV-InnoLIA positive, permanent deferral, refer to Infectious Disease clinic
If HCV-InnoLIA indeterminate or negative, repeat all HCV testing after 6 months
Repeat Hepatitis C Testing After 6 months:
HCV-RNA or HCV-InnoLIA positive: permanent deferral, refer to Infectious Disease clinic
HCV-RNA or HCV-InnoLIA borderline: permanent deferral, HCV infection not confirmed
HCV-Ab positive or borderline without positive HCV-RNA or positive HCV-InnoLIA: permanent deferral, HCV infection not confirmed
HCV-Ab negative, HCV-RNA negative, HCV-InnoLIA negative: reenter donor into donor pool
Note that indeterminate HCV results may be carried forward repeatedly by CBER rules but I decided to permanently defer the donor after 2 cycles of indeterminate results. The donor must wait SIX MONTHS before the next round of testing. Should he/she return before that time, those results may not be used for determining donor eligibility (unless the results have become clearly positive).
Donor marker testing algorithms are very complex and serve multiple objectives:
Is the blood safe for the recipient, i.e. minimize likelihood of disease transmission?
How do we to counsel the affected donor? Does he need referral for treatment or follow-up?
Often the donor disposition is unclear based on a single encounter and a temporary deferral must be triggered so the current results may be compared to future ones, usually after 8 weeks, 6 months, or one year—depending on the pathogen in question.
Regretfully, the significance of reactions that do not meet the criteria for positivity may be unclear. It is very difficult to explain to the donor that he has abnormal results and cannot donate but we as physicians do not know what their significance is.
Thus, the testing algorithms may trigger current additional testing, temporary deferral with repeat of testing at some future date, or permanent deferral.
At my previous positions, I started with the AABB/FDA CBER Uniform Donor Questionnaire UDQ and then modified it to include some advanced methodologies not available in the USA.
In the next series of posts I will elaborate on the processes developed for this for each marker.
Transfusion Medicine includes laboratory and non-laboratory functions. The non-laboratory and purely clinical functions are unique and have no analogy within the general laboratory.
The transfusion service/hospital blood bank laboratory is the closest to a laboratory operation, but there is component modification and complex manual testing, especially for reference immunohematology testing. The staff must make detailed manual decisions, the errors for which could be life-threatening for the patient.
The blood donor center manufactures a pharmaceutical, i.e. blood components with collection, donor qualification, donor abnormal results review, infectious disease marker testing, component production, and donor immunohematology testing—all subject to Good Manufacturing Practices. Never forget: Blood is a drug!!
No other laboratory section is directly responsible for treatment of critically ill patients. Therapeutic apheresis is essential for organ and stem-cell transplants, nephrology, neurology, etc. No other laboratory section is directly responsible for treatment of critically ill patients. Transfusion Medicine physicians are functioning as intensivists. There is no hiding in the laboratory from clinical medicine.
There may also be an industrial manufacturing plant to extract various blood derivatives (e.g. factor concentrates, albumin, Rh immune globulin, etc.) This is pharmaceutical manufacturing on a large-scale basis. There is medical, technical, and special administrative expertise.
Many functions may operate 24/7. The transfusion medicine physician may be on-call for donor issues and review of complex immunohematology problems to acutely decide which blood component (and phenotype) should be given as well as review all adverse reactions to transfusion.
The unique blend of clinical skills is unlike anything else in the laboratory. Also, those outside the blood bank rarely have the skills or judgments for the best course of action for transfusion medicine or for its operations.
The clinical transfusion medicine physician must make acute, life-threatening decisions unlike anyone else in the laboratory. The blood bank technologist is at the cutting edge of the battle with his testing and interpretations. No other area of the laboratory is at such risk for injuring or even killing the patient. There is high stress and burn-out.
I have talked with many blood bankers and many seem to share the exasperation that the laboratory does not understand us. The latter looks at blood bank testing like that coming off a hematology or chemistry analyzer—although patients rarely would have severe morbidity or mortality like the blood bank from errors in those analyzers.
No laboratory pathologist has the pressure of the blood bank physician on-call. It really is 24/7 and requires a broad, clinical background to make the right decisions. It is very stressful and does not permit a good night’s sleep.
Thus, I make my case to separate us from the laboratory. We can form our own more effective administrative organization and optimize our own planning. Regretfully, I have never worked in such an administrative structure. I also am a realist that cost-containment nowadays makes it much less likely high administration would permit this change for a mere cost center. This will probably never happen during my career.
Finally, Transfusion Medicine is an essential service. Blood components are essential drugs. The operations and staff must be free of political influences. This is a service for the entire region or country like the fire department, civil defense, etc.
Enforcing Good Manufacturing Process Through A Dedicated Blood Bank Software
Blood components are a drug and like medications must be consistently produced and follow Good Manufacturing Practices GMP. The following system that I set up for HMC Doha Qatar blood collection and processing is an example of the impact of Medinfo donor software on enhancing our safety and GMP compliance. In earlier posts, I provided the Medinfo flowcharts for these processes.
This is an outline of the processes I built in conjunction with the Medinfo software engineers:
Registration:
Read the barcode on the specified picture ID (usually a Qatar Residency/Citizen card).
Retrieve the prospective donor’s demographics in English and Arabic from the Ministry of Interior.
Check the donor deferral database (Qatar has only one), defer if contraindicated according to the rules built into Medinfo.
Choose the type of donation (apheresis or whole blood; volunteer, directed, or autologous).
Print a consent form and ISBT specimen labels for the donation.
Pre-Collection Screening:
Perform the donor questionnaire on-line in English or Arabic: this has contingent fields and could exceed 60 questions depending on the answers provided.
Proceed to donor physical exam (vital signs and arm check).
Collection:
Collect the whole blood or apheresis component and specimen tubes: determine if the collection meets the volume requirement and time limit.
Send the specimens for donor marker and donor immunohematology testing.
Send the raw components for processing.
Donor Marker Testing:
Perform NAT, EIA, and LIA marker testing according to algorithms defined in Medinfo.
Perform follow-up reflex marker testing according to Medinfo criteria.
Component Processing:
Process the raw whole blood in the Reveos machine into PRBCs, leukodepleted plasma, and buffy coat platelets.
Filter/leukodeplete the RBCs.
If marker test results pass:
Pool the buffy coat platelets according to the platelet yield index for a yield of 2.4E11/dose.
Add platelet additive solution PAS and pathogen inactivate (Mirasol).
Pathogen inactivate the whole-blood-derived plasma.
Divide the apheresis plasma into 200-250 ml aliquots and pathogen inactivate.
Divide the apheresis platelets to provide a yield of 2.4E11 in each dose, then pathogen-inactivate (PAS had been added at the time of the apheresis collection).
Donor Immunohematology Testing:
Perform ABO/D testing and antibody screen (identification if positive):
If antibody screening positive, discard the component.
If ABO discrepancy, send for manual review and approval, otherwise discard.
Labelling, Storage, and Transfer:
If all criteria were met, attach the final ISBT label (this can only be printed based on the acceptance of each component).
Place the components into storage (37C, 1-6C, or <= minus 18C).
Distribute to the hospital blood banks using Inter-Depot Transfer function.
I emphasize that only if all criteria across all areas pass is the final ISBT label printed. Medinfo is not a label printing program. It enforces the rules ruthlessly. My technical staff tell me that it is merciless—as it should be for patient safety.
Attachments: None—please refer to earlier posts regarding collection, processing, donor testing, and inter-depot transfer.
When buying equipment while planning/implementing new laboratory software, I originally had a rule not to purchase anything that the vendor did not have a ready interface. Even that was not so clear since some vendors had interfaces listed as alpha, beta, and completed.
Could you use an alpha or beta interface? Was it safe for patient care? What was the development cycle for new interfaces with your vendor—months, years?
Even if the vendor had a completed interface? How “complete” was it? Did it accept all data from the machine? Did the data stream require reformatting? Who would write the transformational script?
Even if the vendor could support it, could your local IT organization and the local agent’s IT staff do it? I had plenty of headaches over this. The best equipment with the best interface that the local agent could not support was worthless to me.
Some finished interfaces took months to install because of connectivity issues? What version of the operating system was used? Was it secure? Did our IT department accept that version (e.g. Windows 7) and the provided malware protection? I have seen malware spread across a network from the interface software installed by the vendor, threatening the entire corporate system.
Did the solution require middleware? What were the implications of having middleware and its affect on the main software program, especially at the time of its upgrade or the main software?
I have seen vendors using Windows 2000 for their interface software as late as 2017. It was difficult for some of them to update to current, more secure versions. Anyway, our corporate IT department gave them all a deadline to update to the current operating system—they all complied or risked losing all connectivity to the network.
Almost every instrument vendor has told me that they can communicate with my laboratory system. I guess that is true: one talks in Russian and the other Sanskrit—they do communicate but is it effective? Talking is not necessarily communication!
I remember one open EIA machine that had a TCP/IP port but it was not functional by the standard protocols. One had to emulate a serial port to get some rudimentary communication. The port’s light blinked, however. I never imagined that someone would put a nonfunctional port as a mere decoration.
On the other hand, I have had excellent experience with another software vendor Medinfo. Even if the vendor did not have the interface developed, they could build it from scratch in a few weeks. Paradoxically, it was faster for these new interfaces than some so-called already interfaces.
I must emphasize: This is a collaborative team effort between the blood bank information system, software vendor, instrument vendor, and your institution’s IT staff. There must be excellent cooperation between them for a successful result.
When installing the Medinfo Hematos IIG software, many of our most important interfaces (the Terumo mixed shaker, Trima, Reveos and its predecessor Atreus, Mirasol illuminator) had no developed interfaces when we started, This was a risk; but actually those interfaces were developed in a few weeks and fully functional. In fact, we were the first site in the world to have those interfaces working—and without any Middleware.
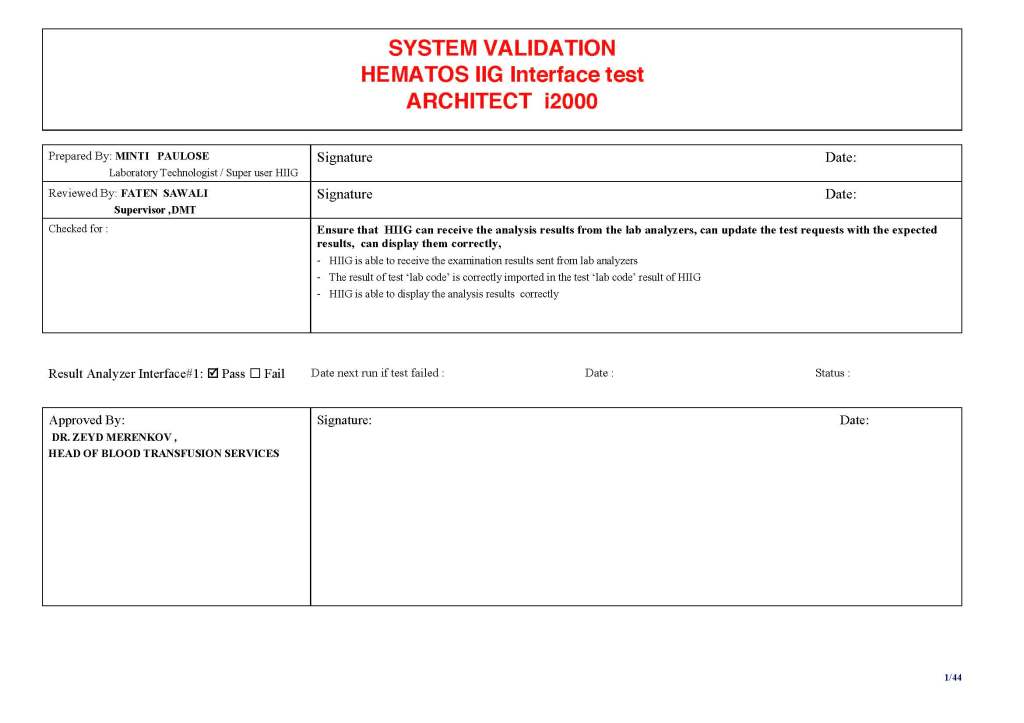
In general, the blood bank software vendor installed the completed interface and did some low-level testing. Then, my blood bank computer team did the testing. The final responsibility for testing and acceptance was with the end-user blood bank team.
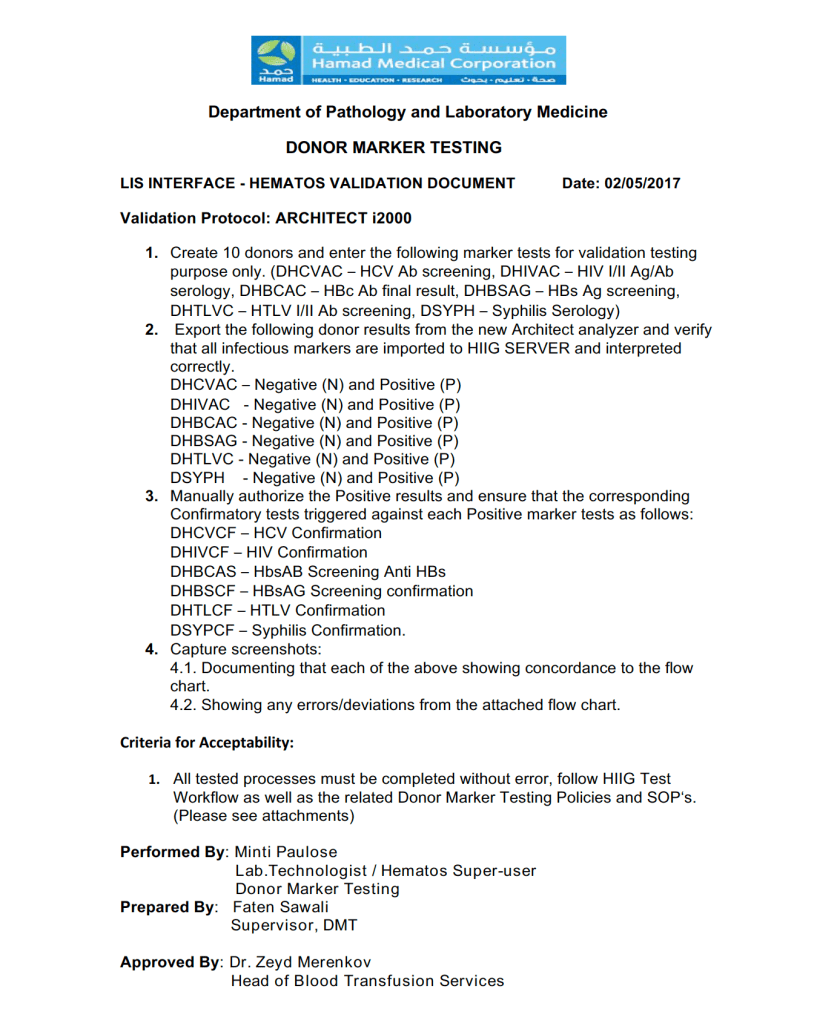
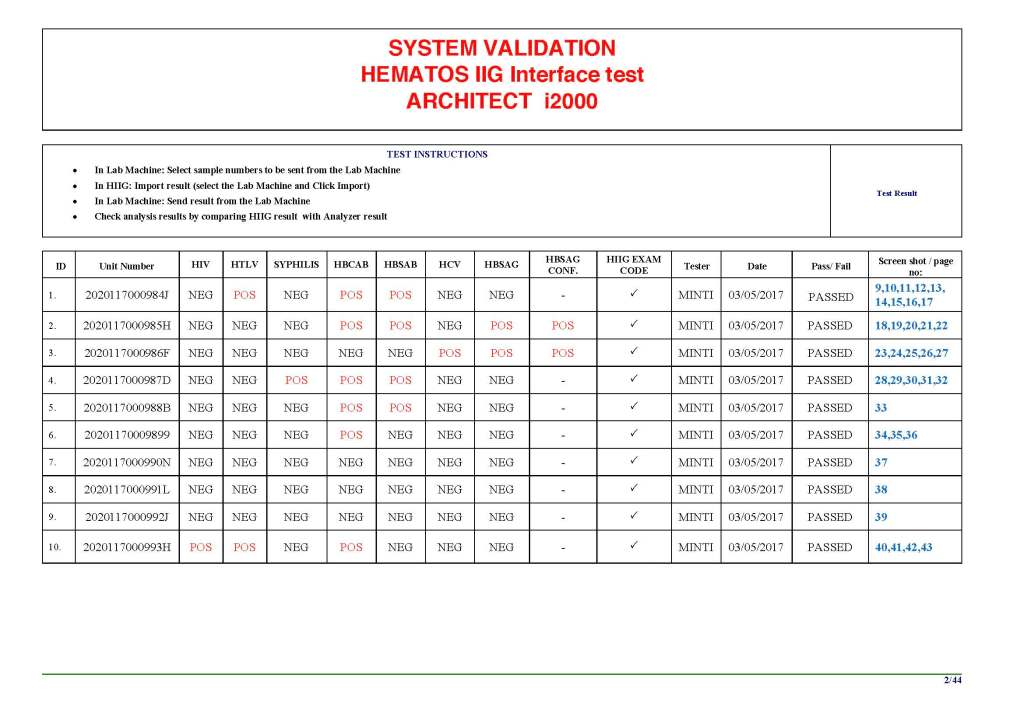
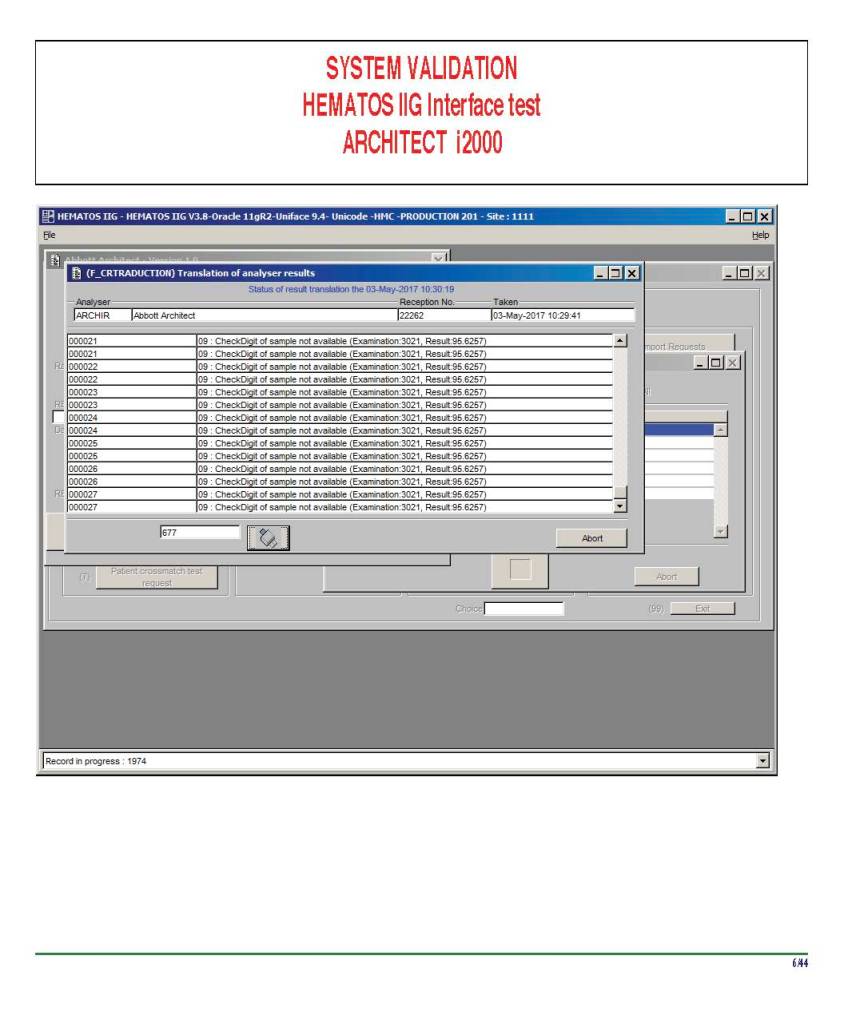
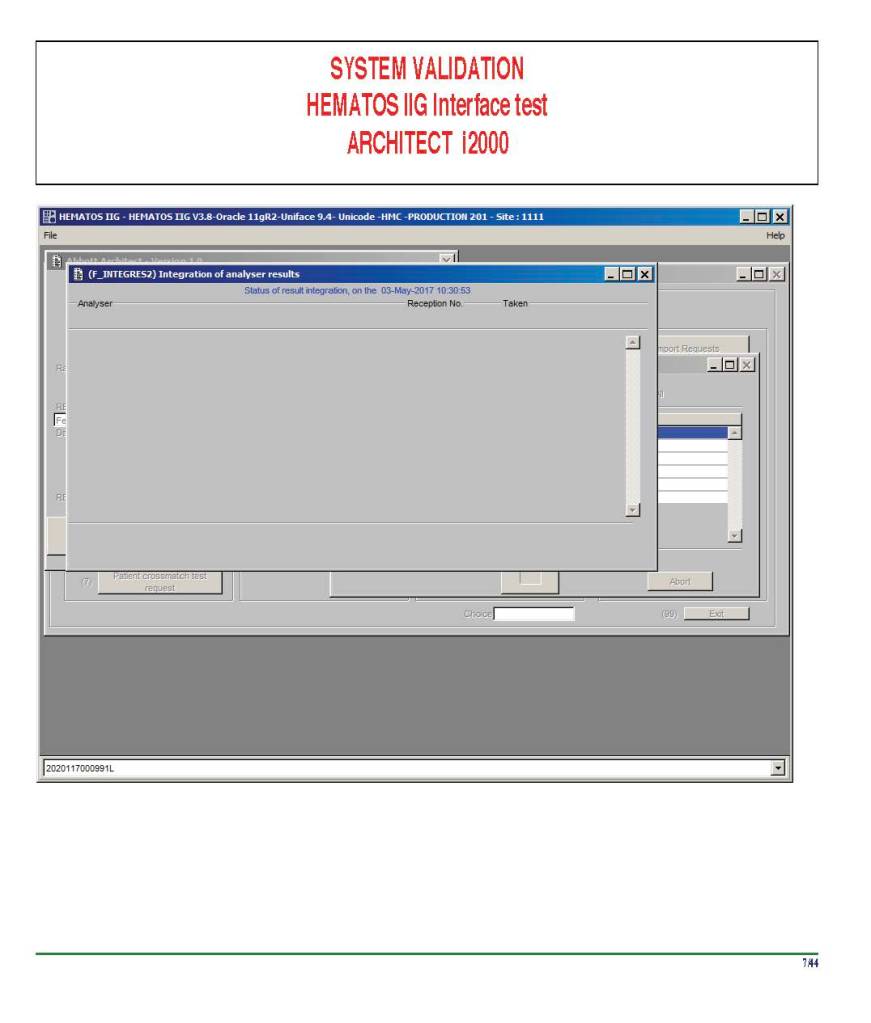
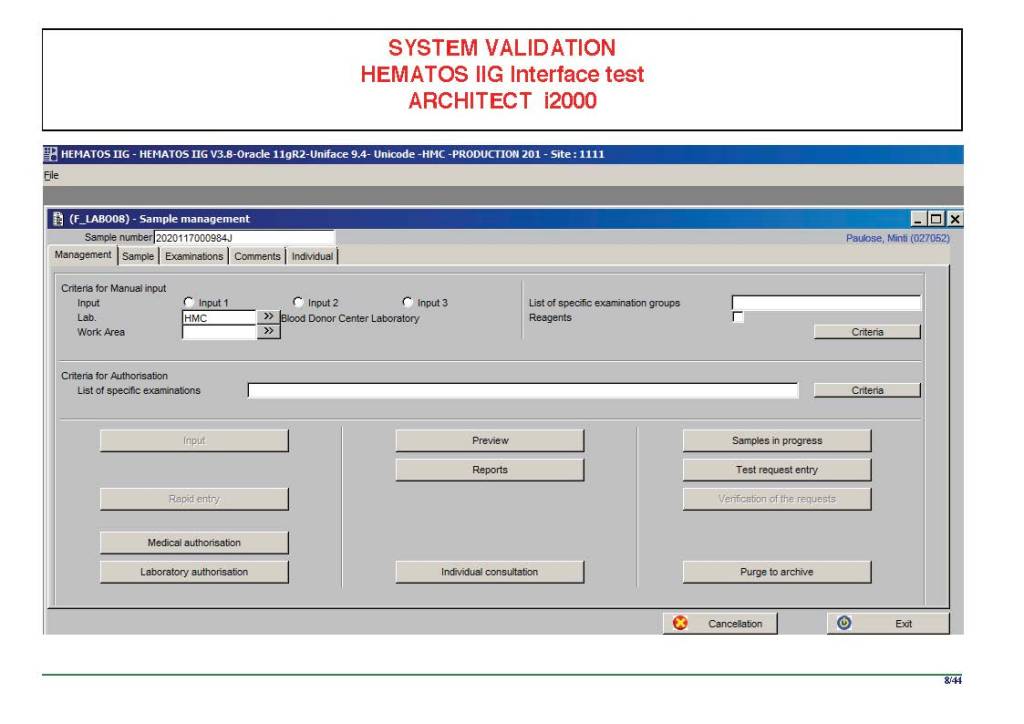
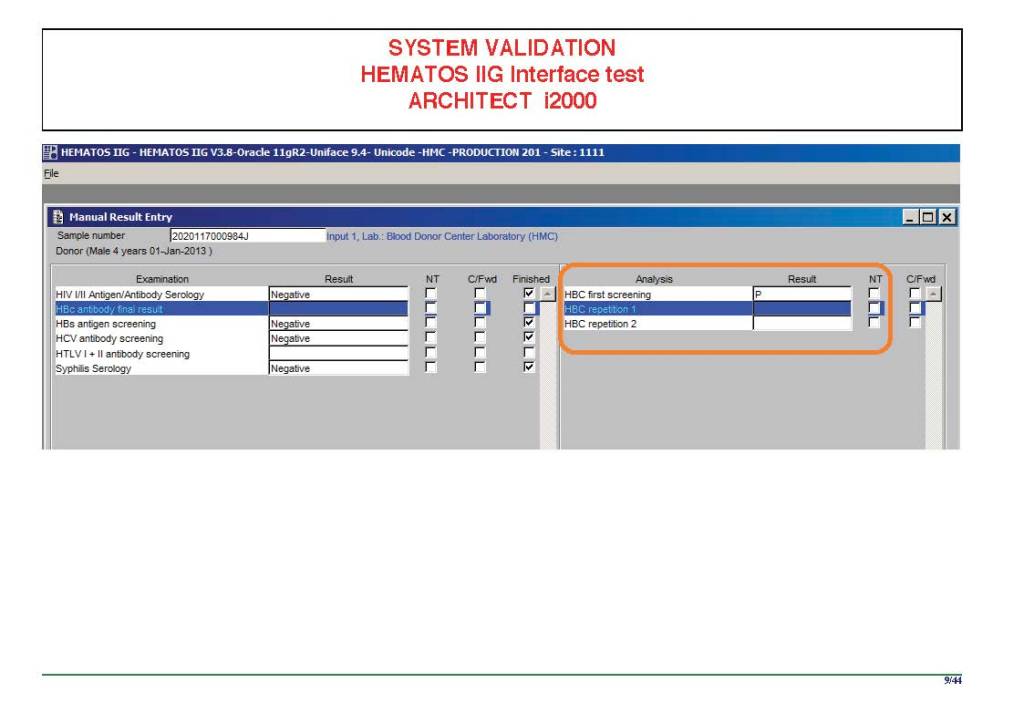
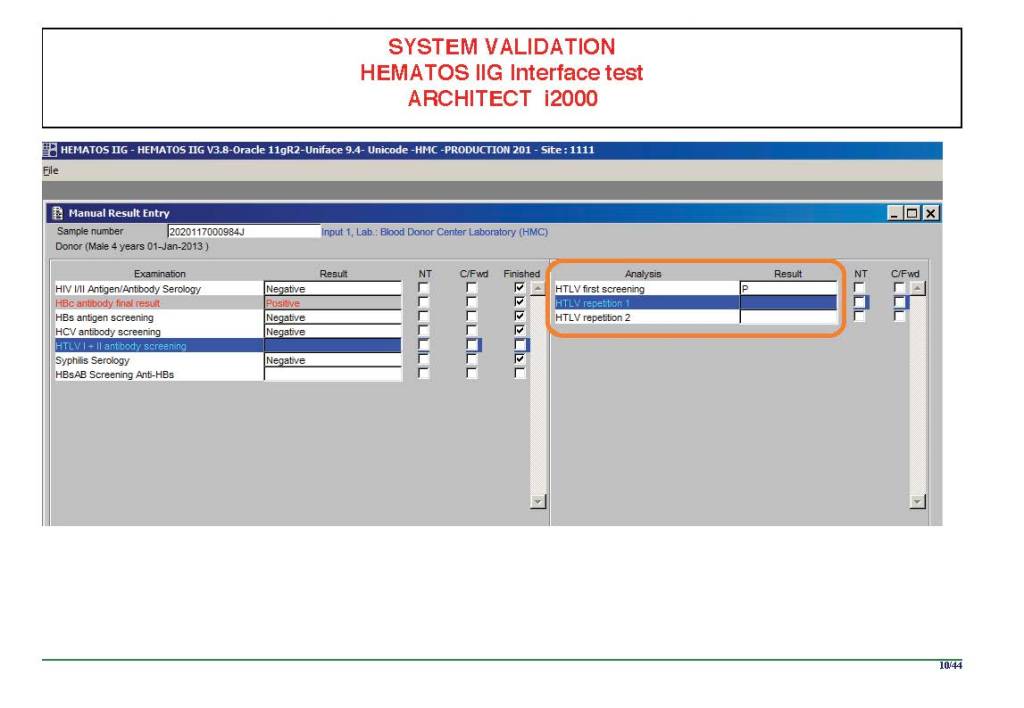
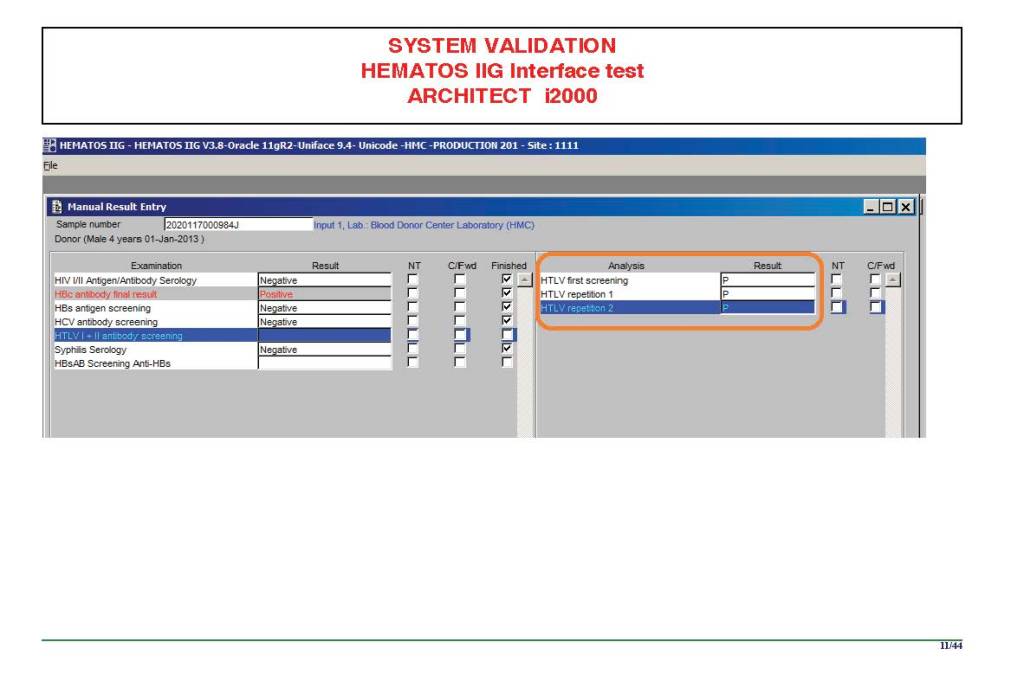
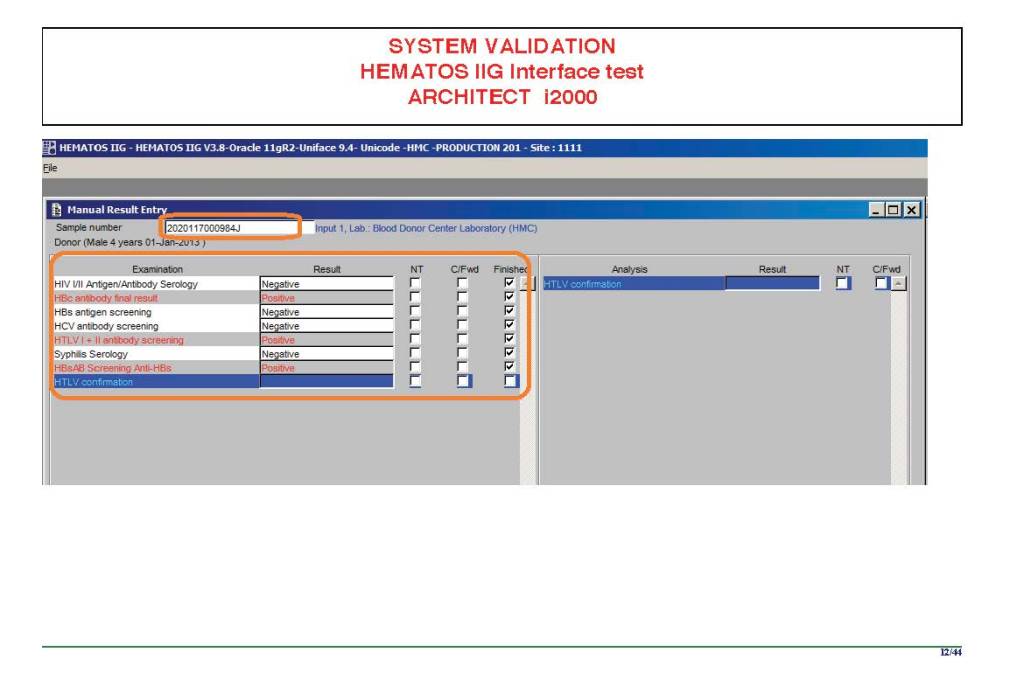
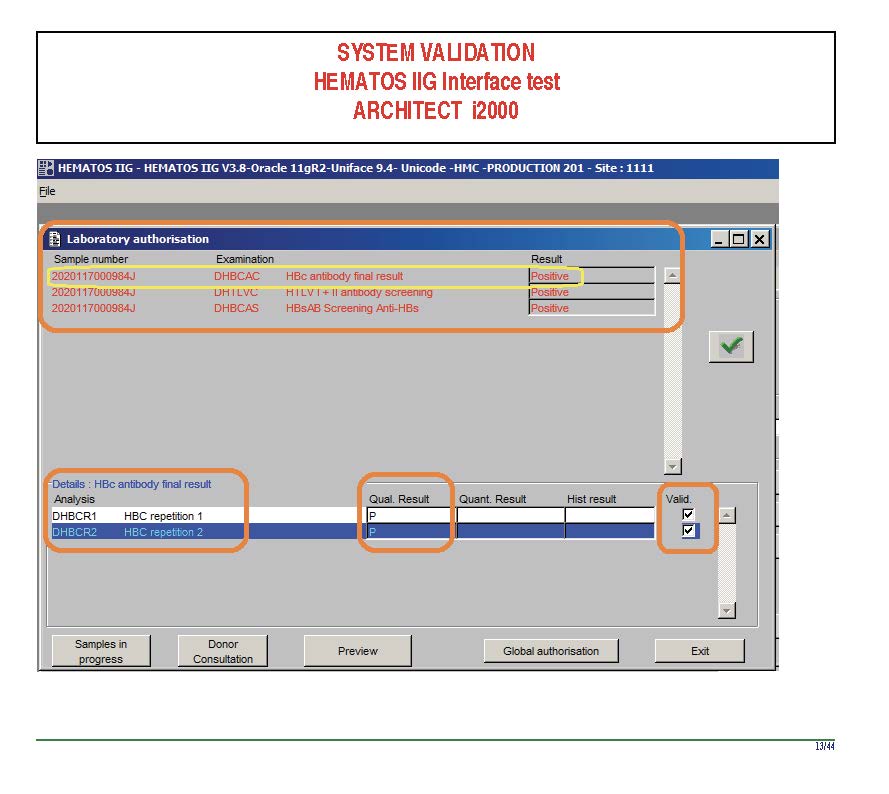
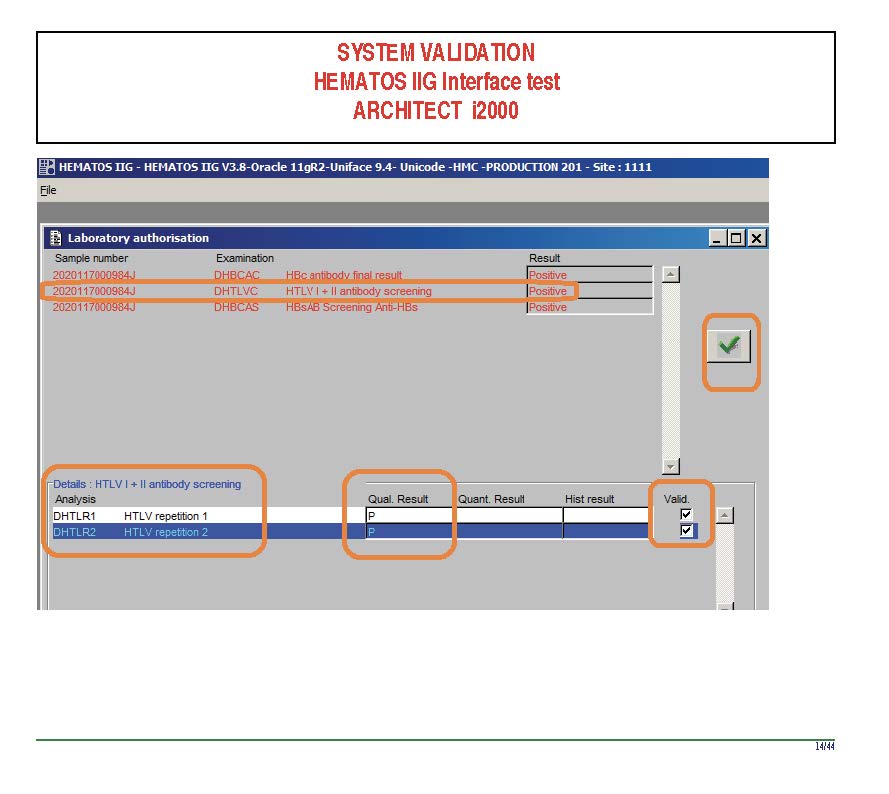
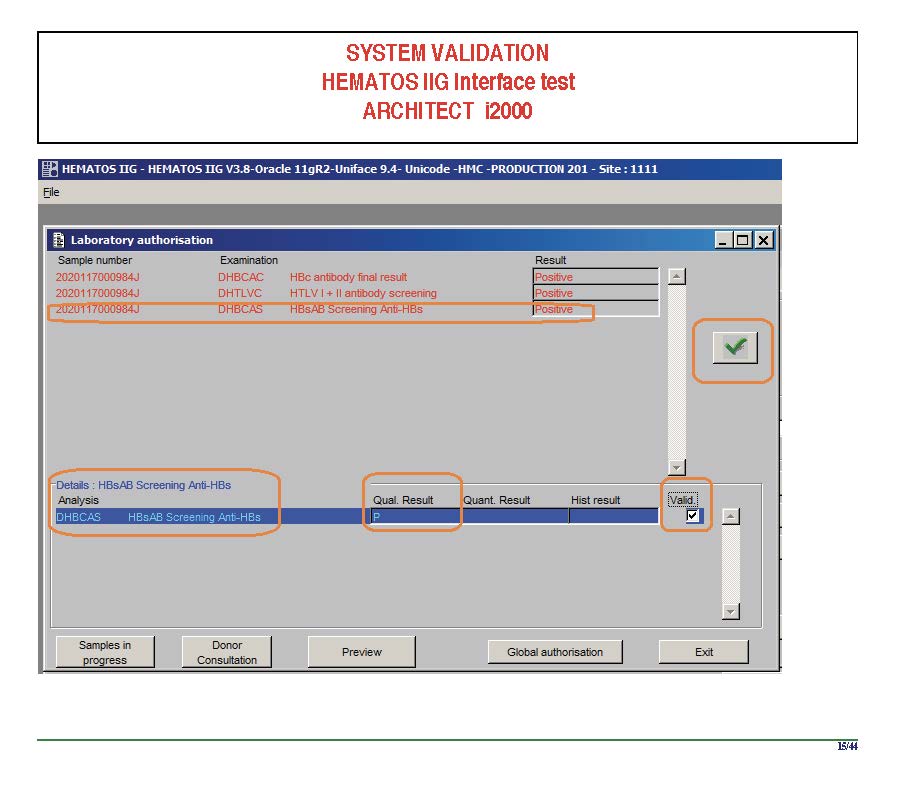
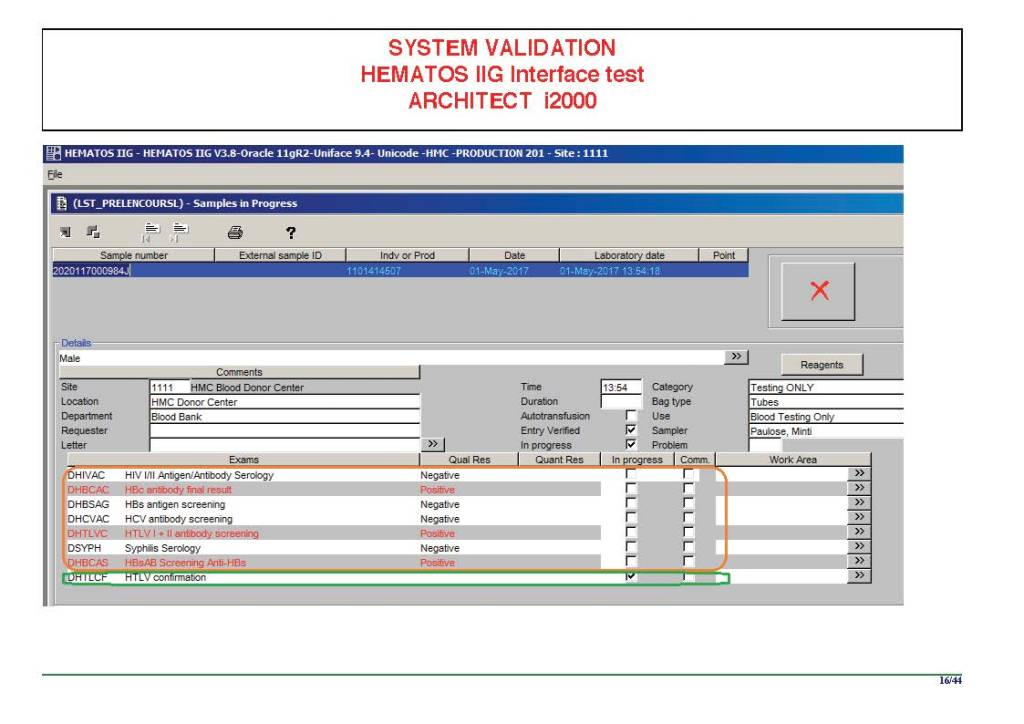
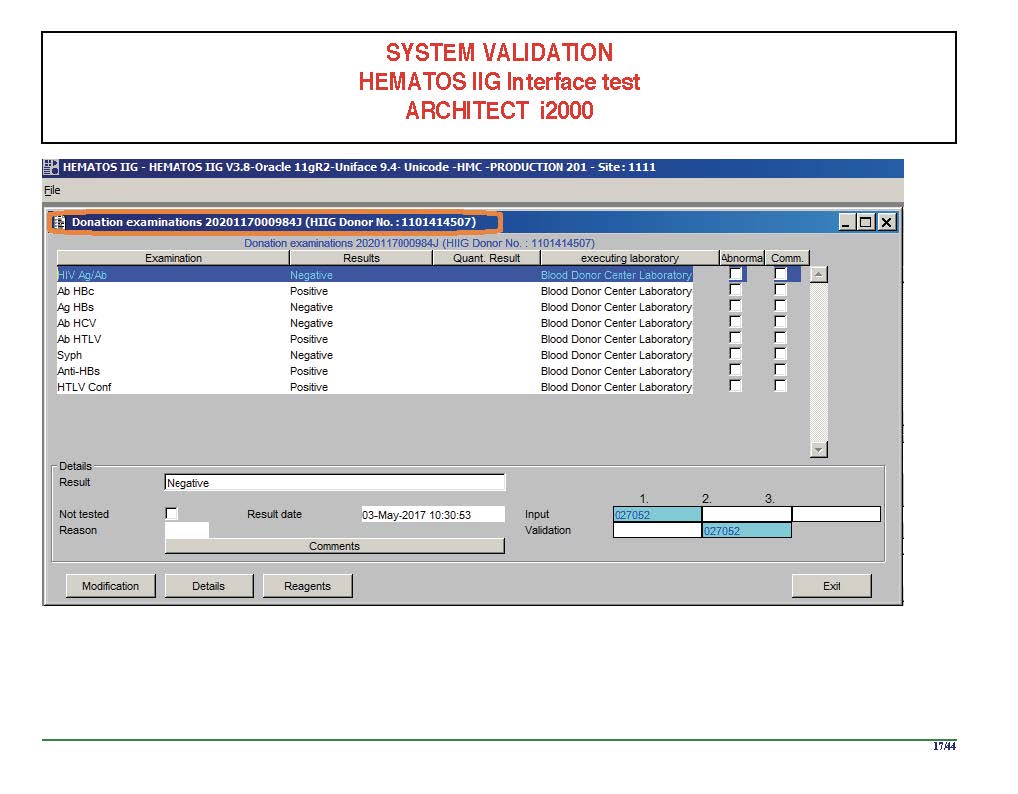
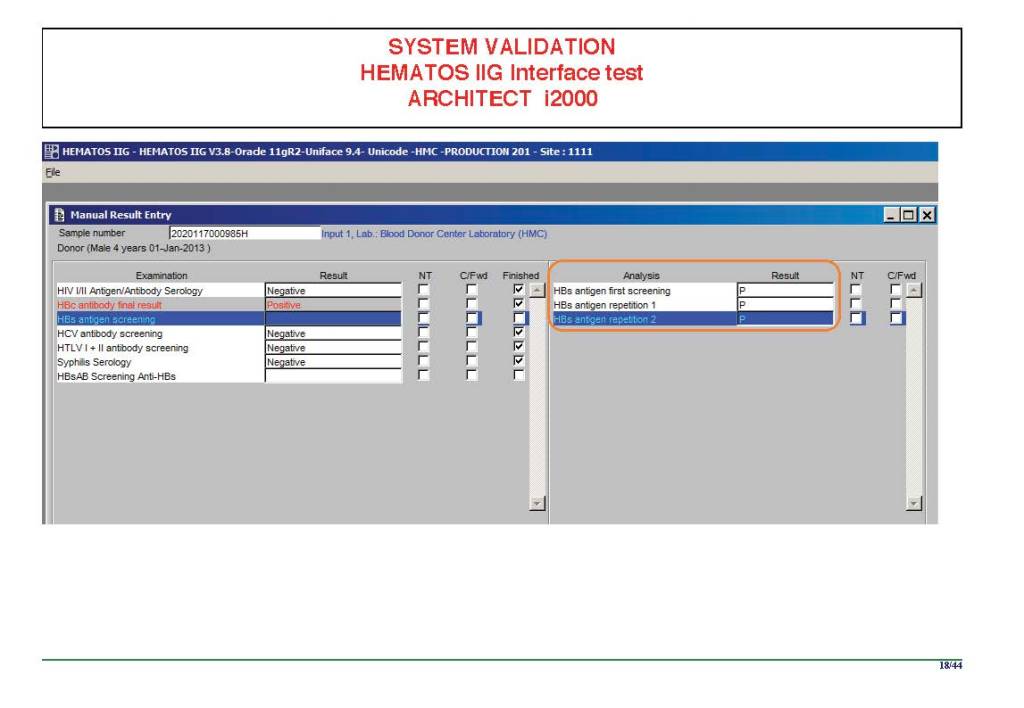
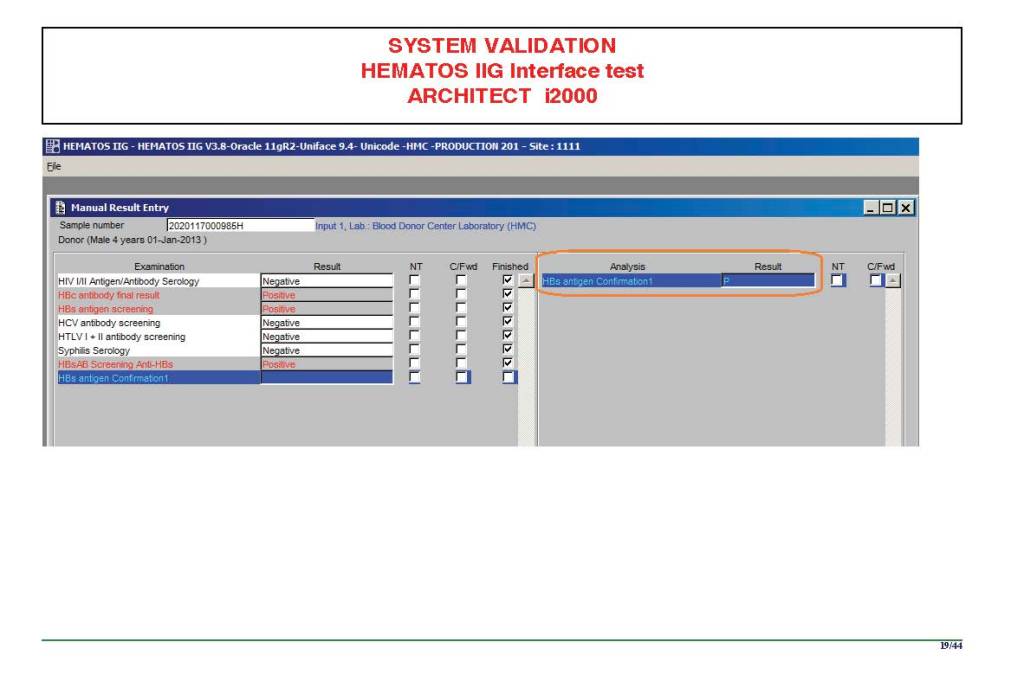
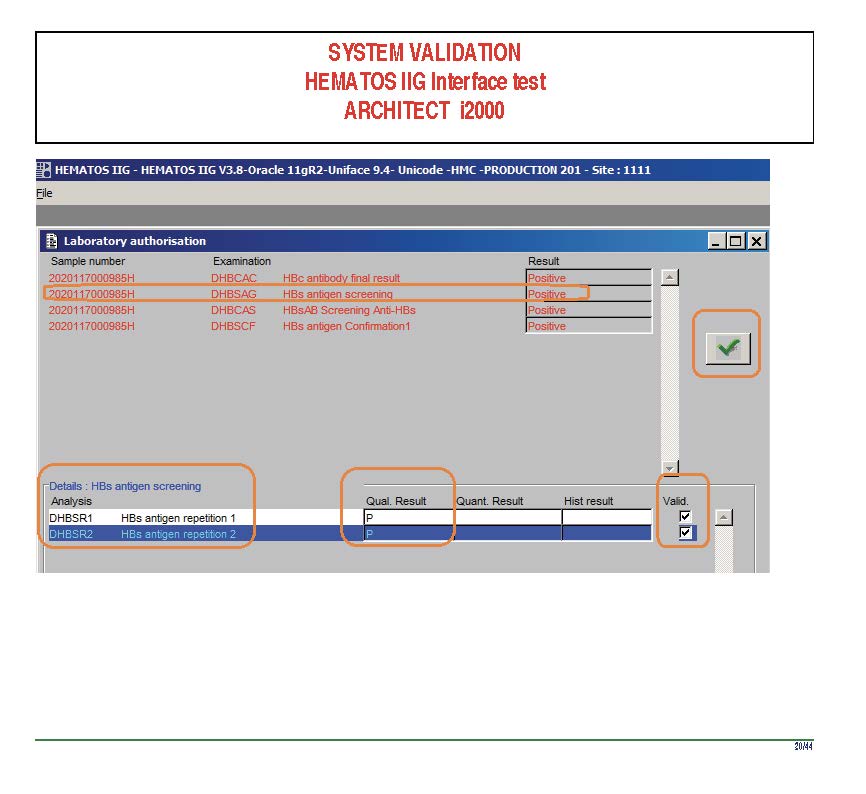
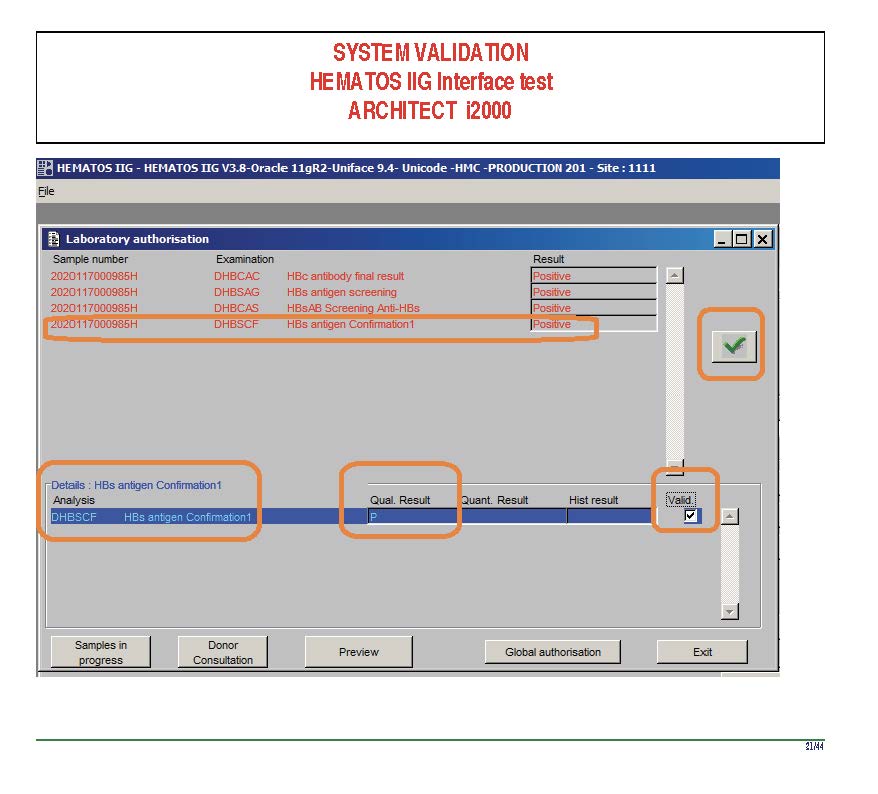
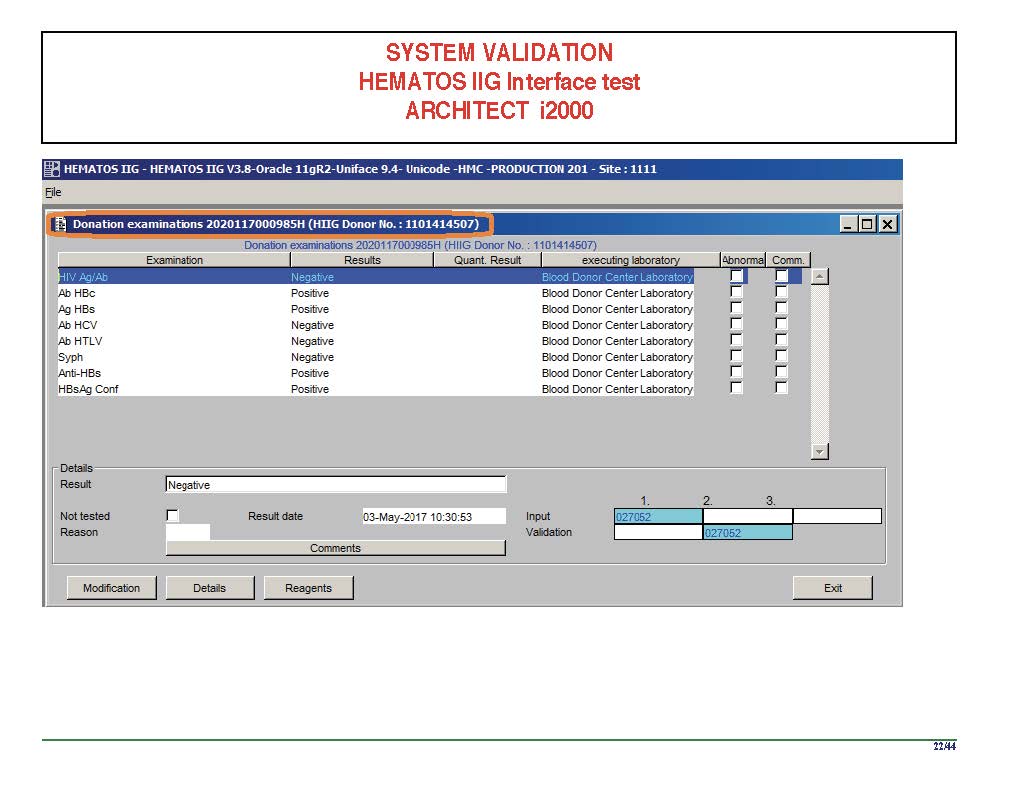
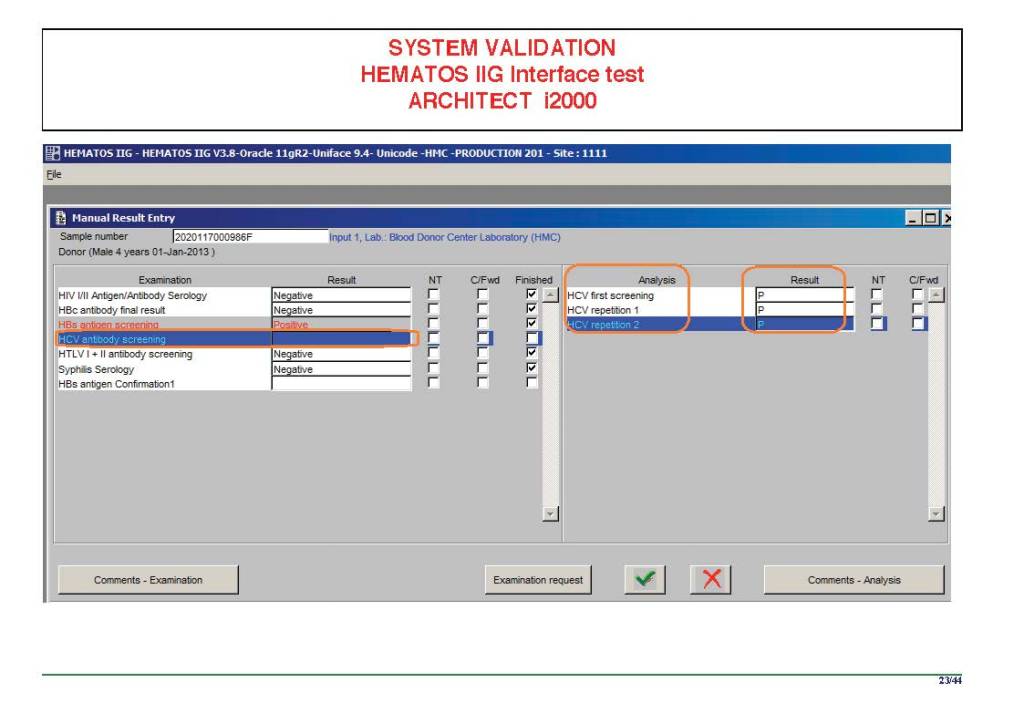
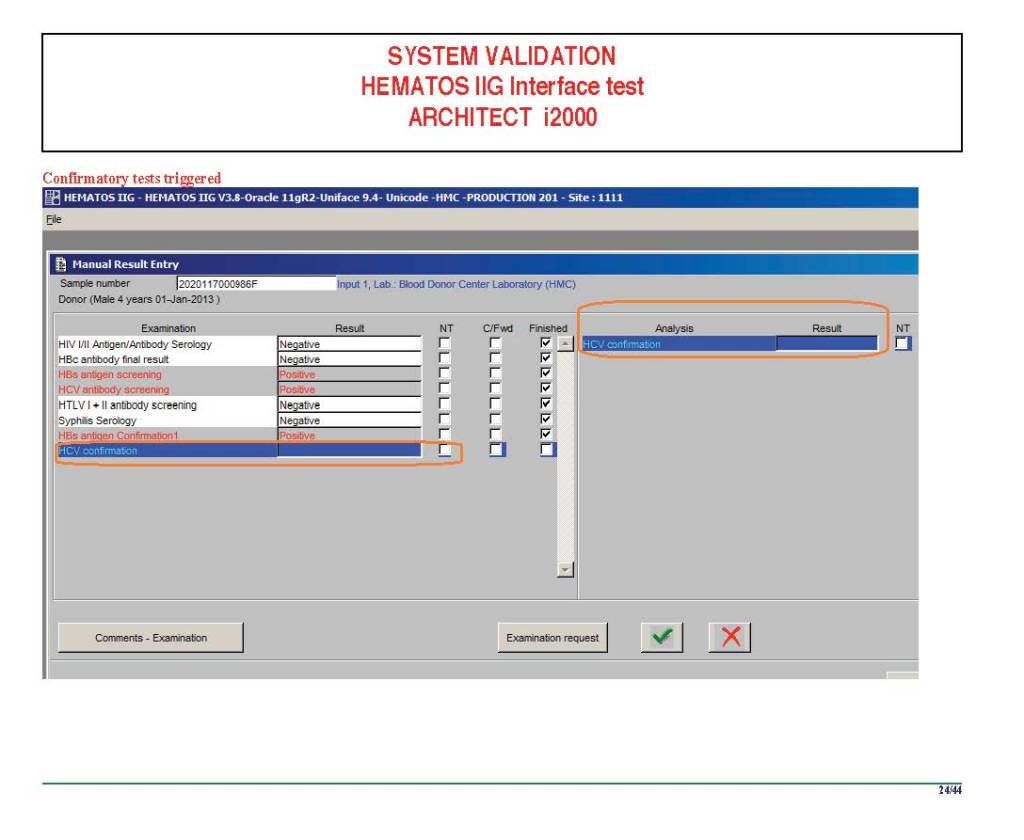
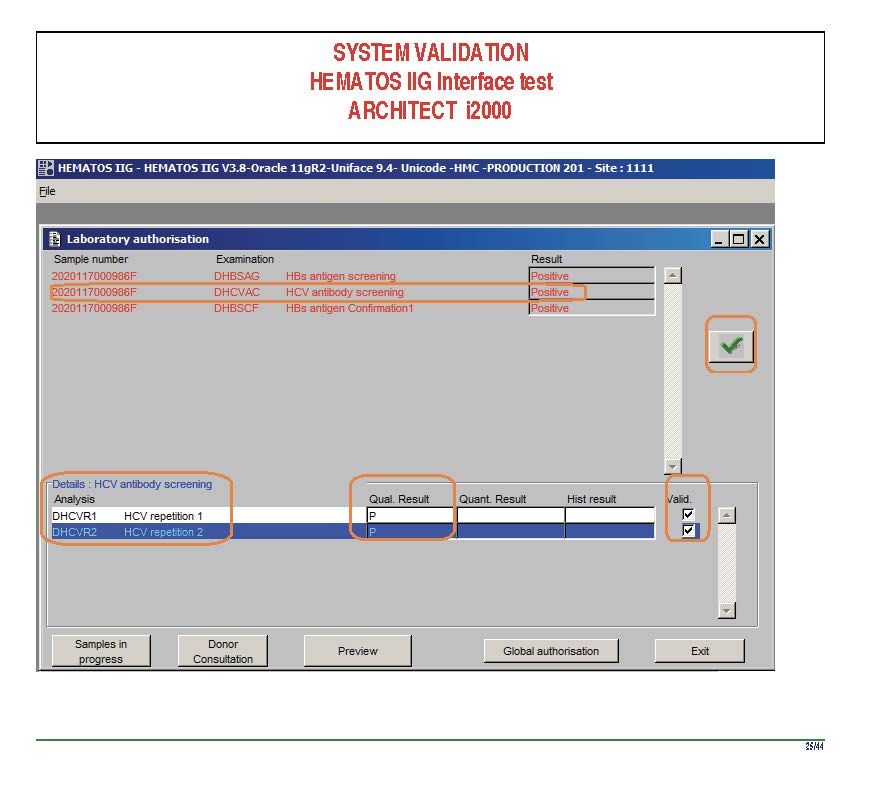
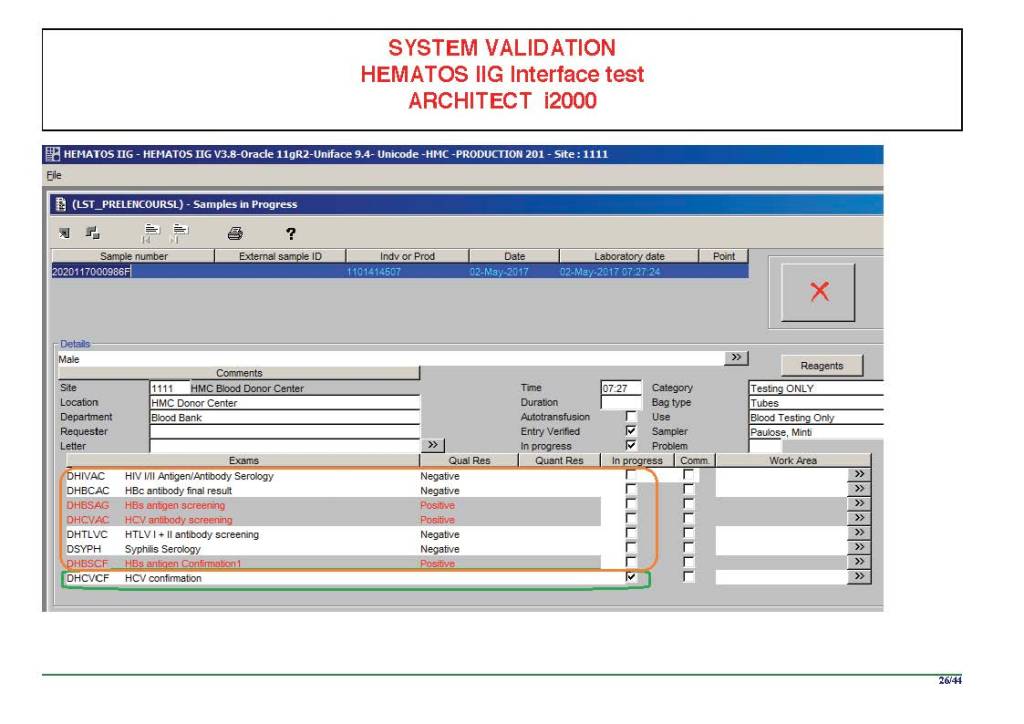
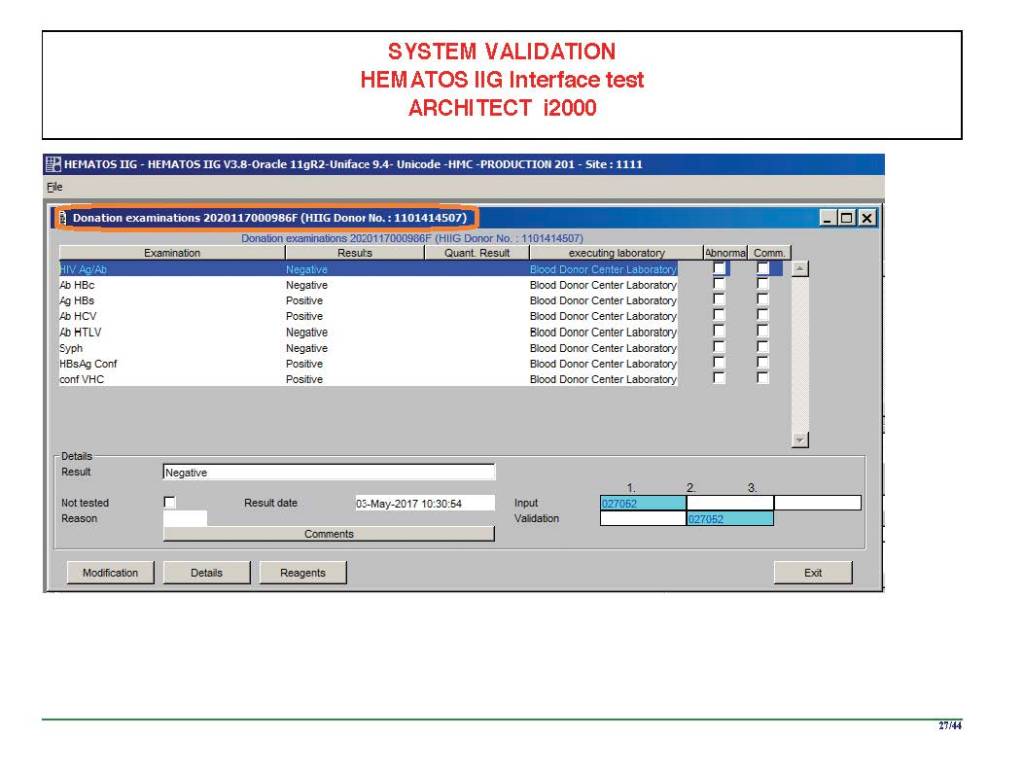
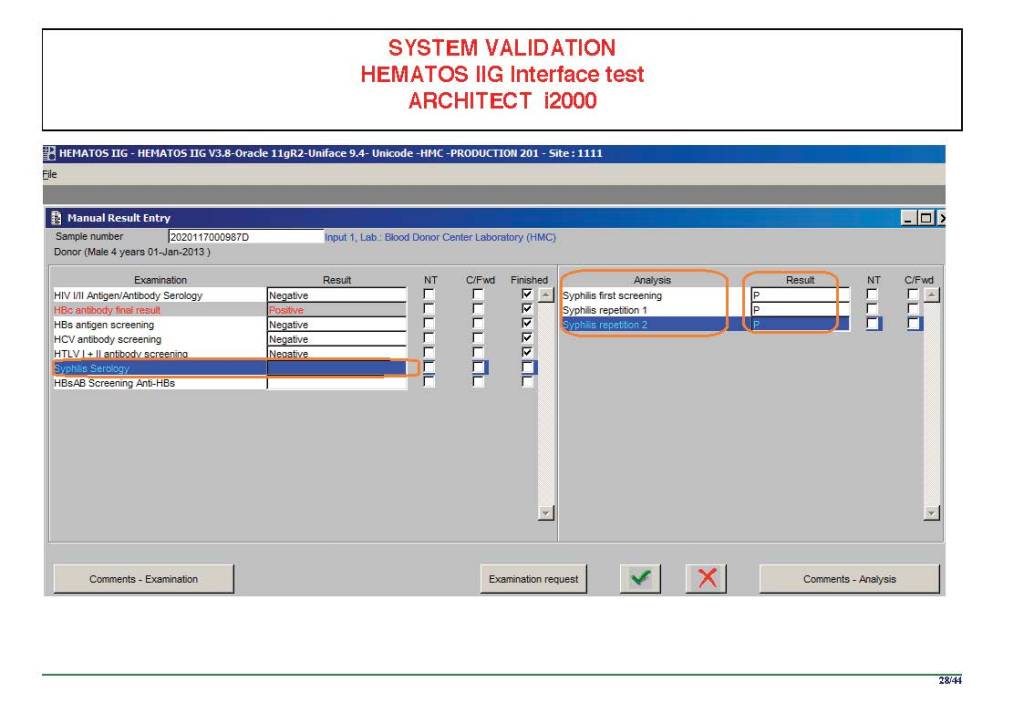
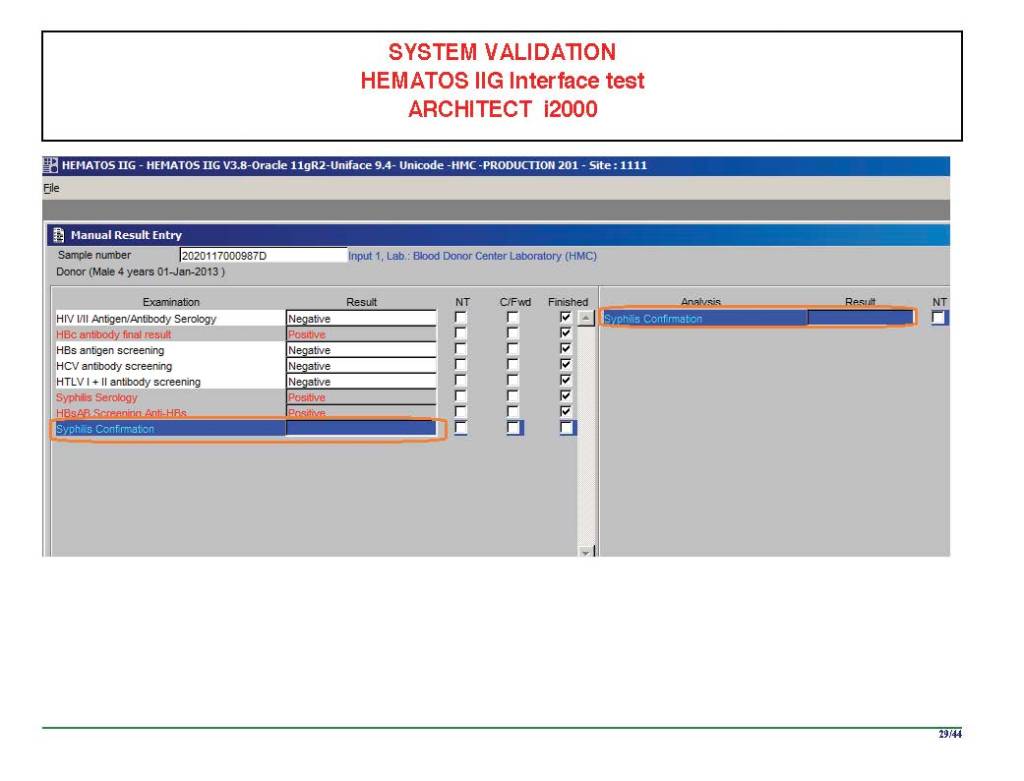
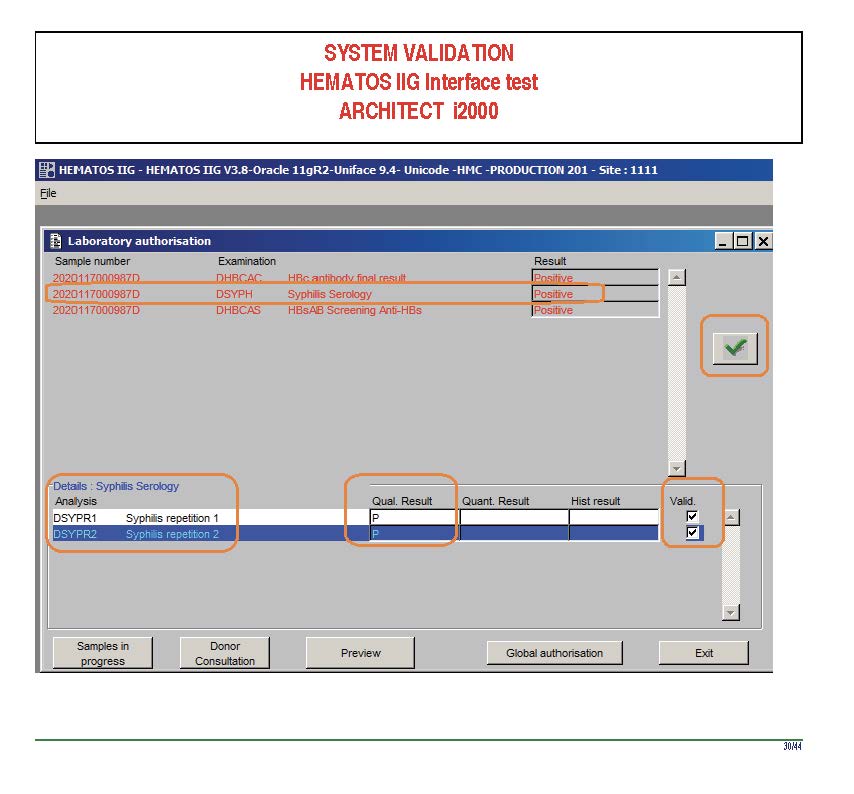
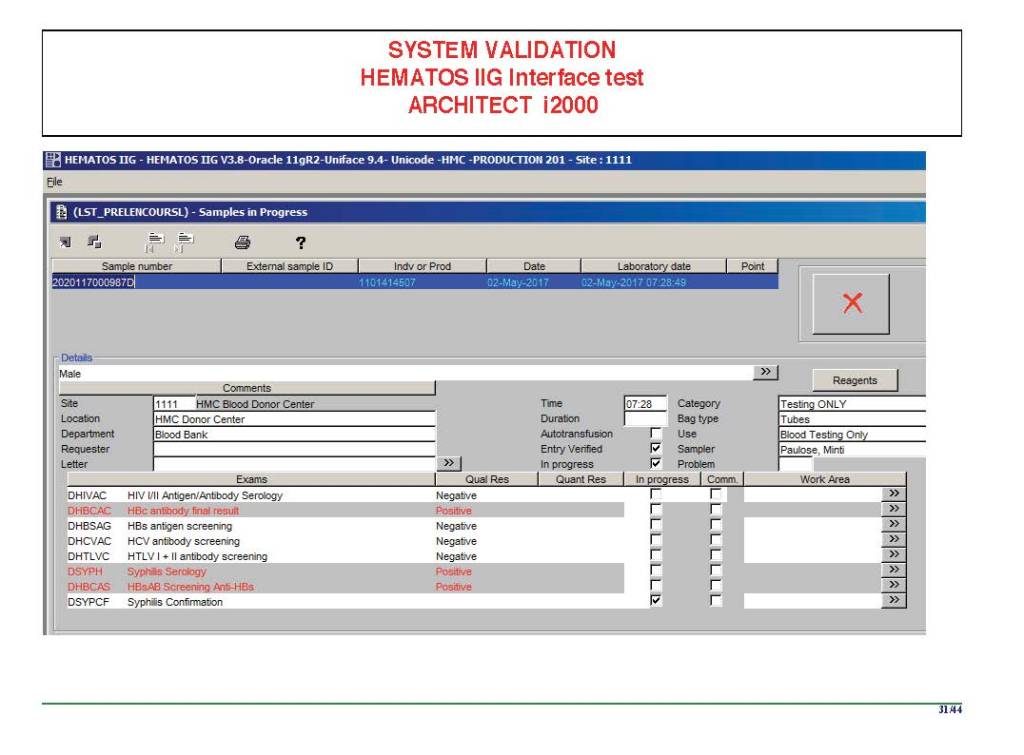
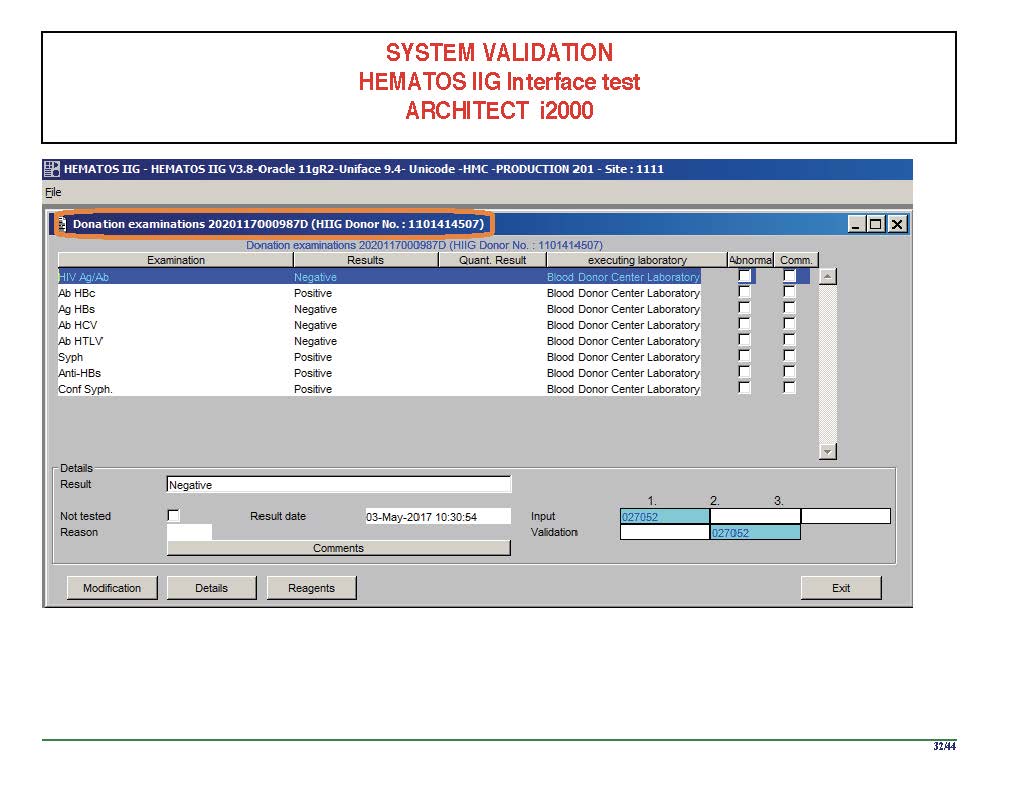
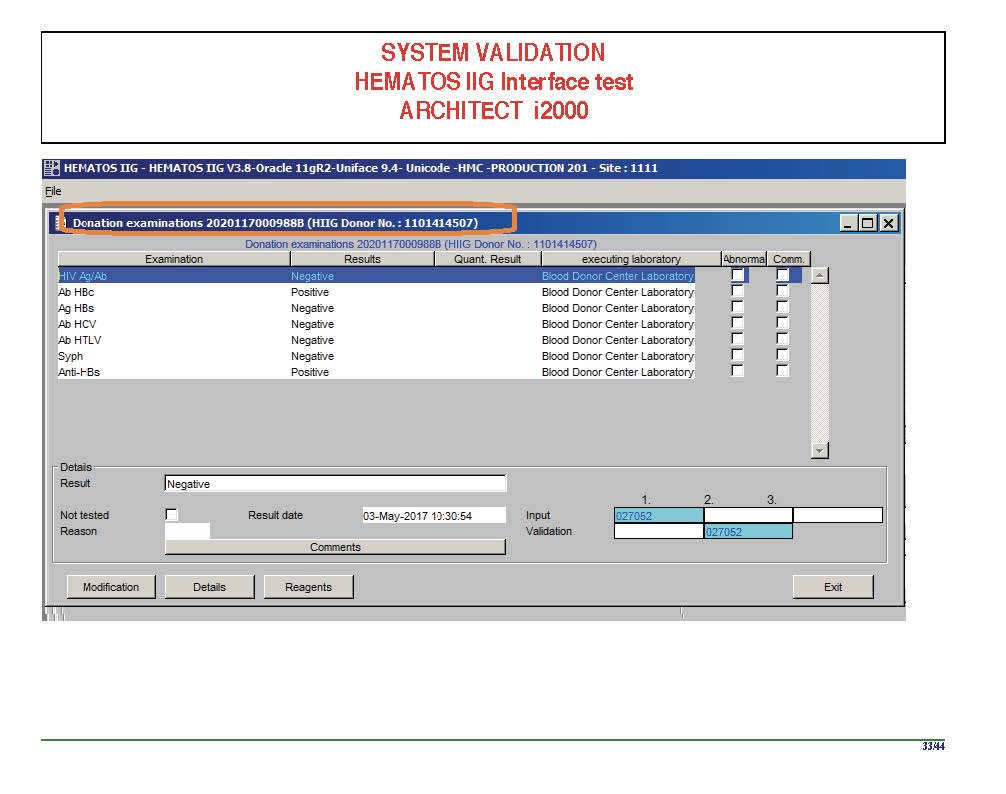
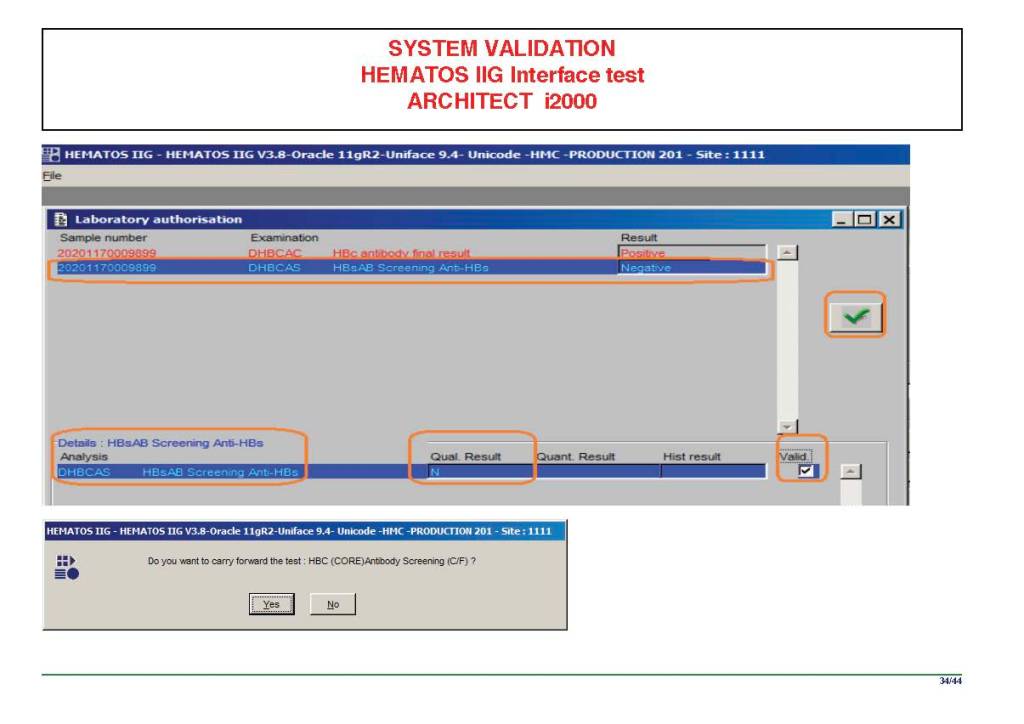
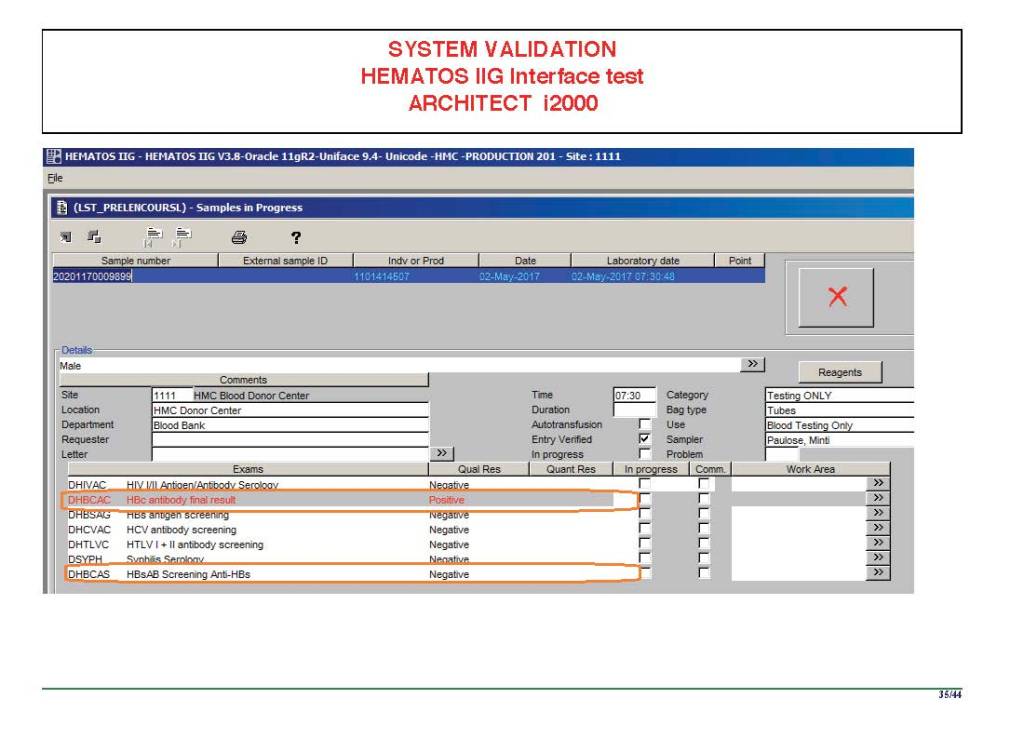
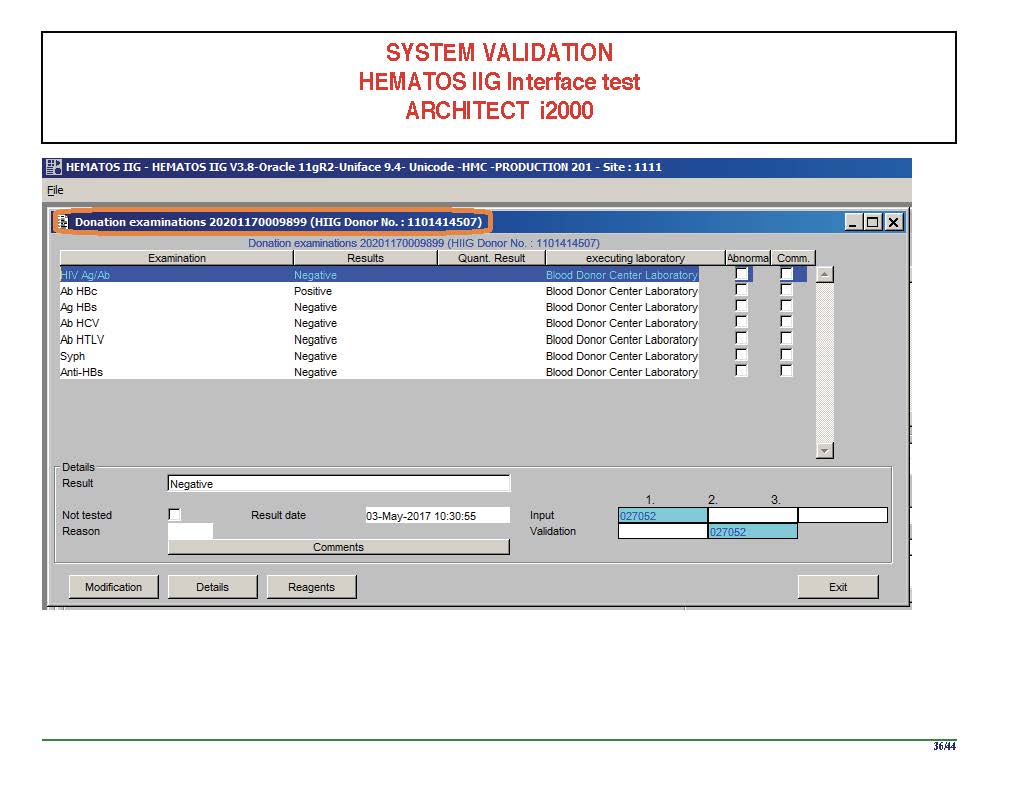
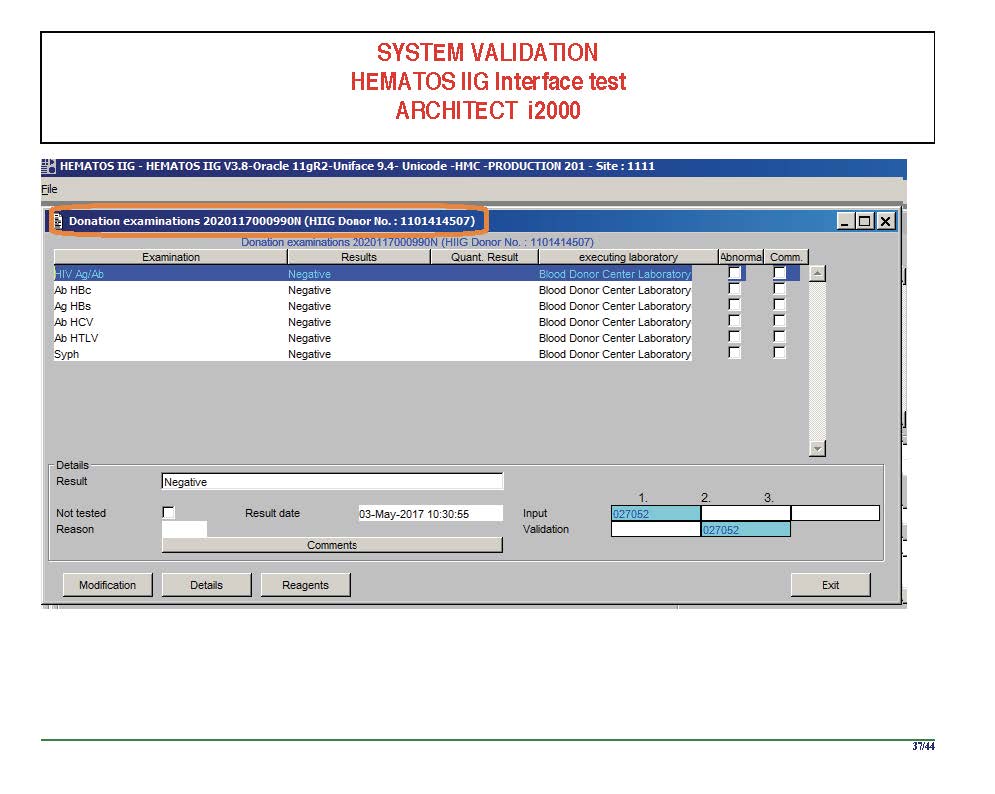
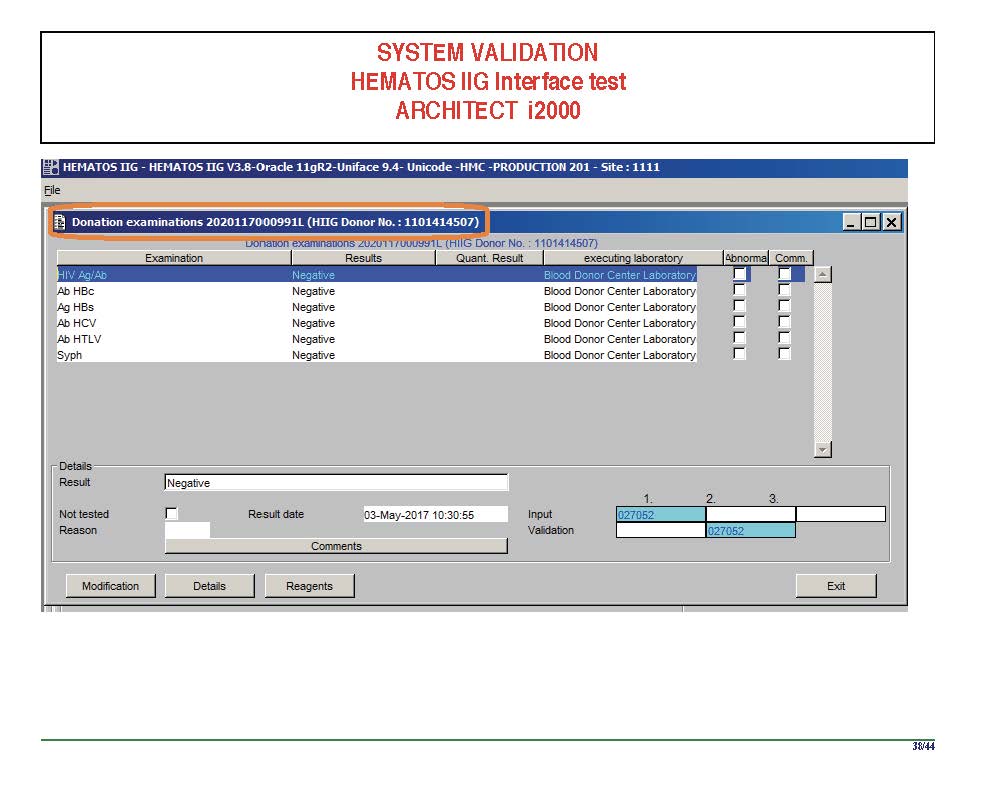
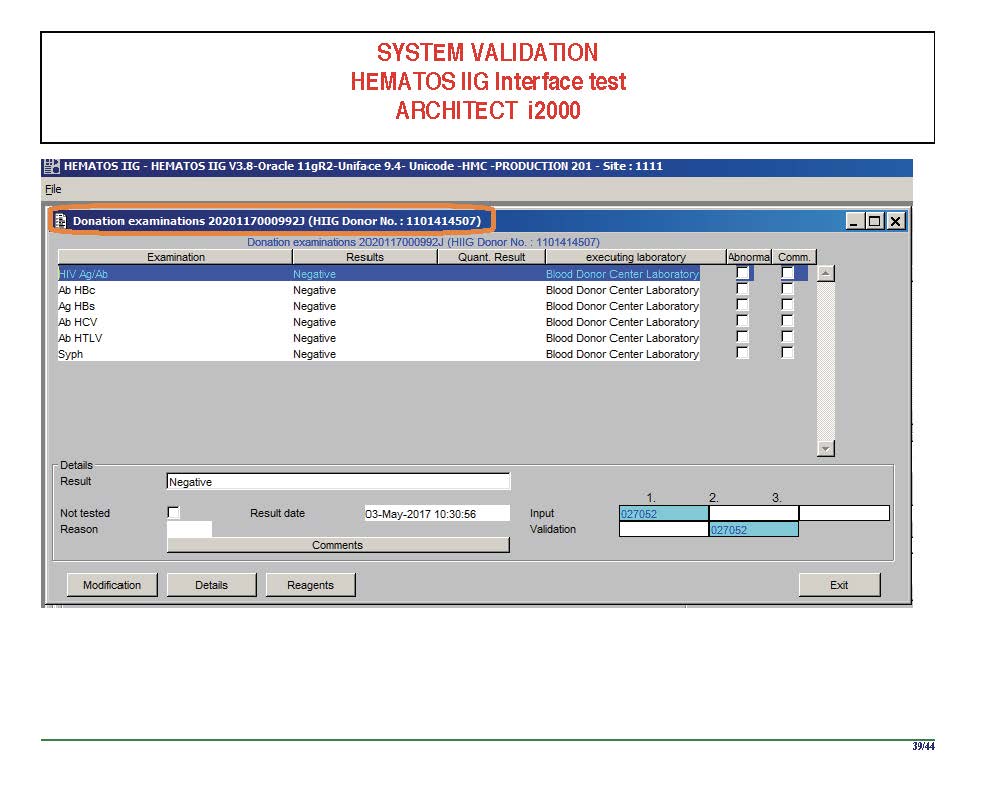
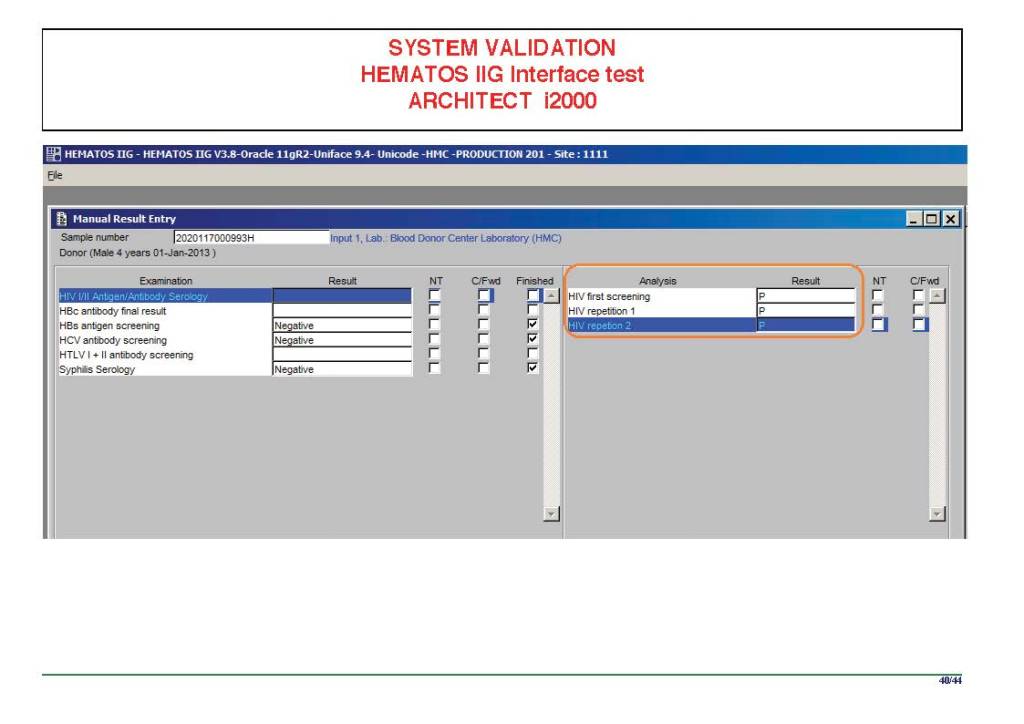
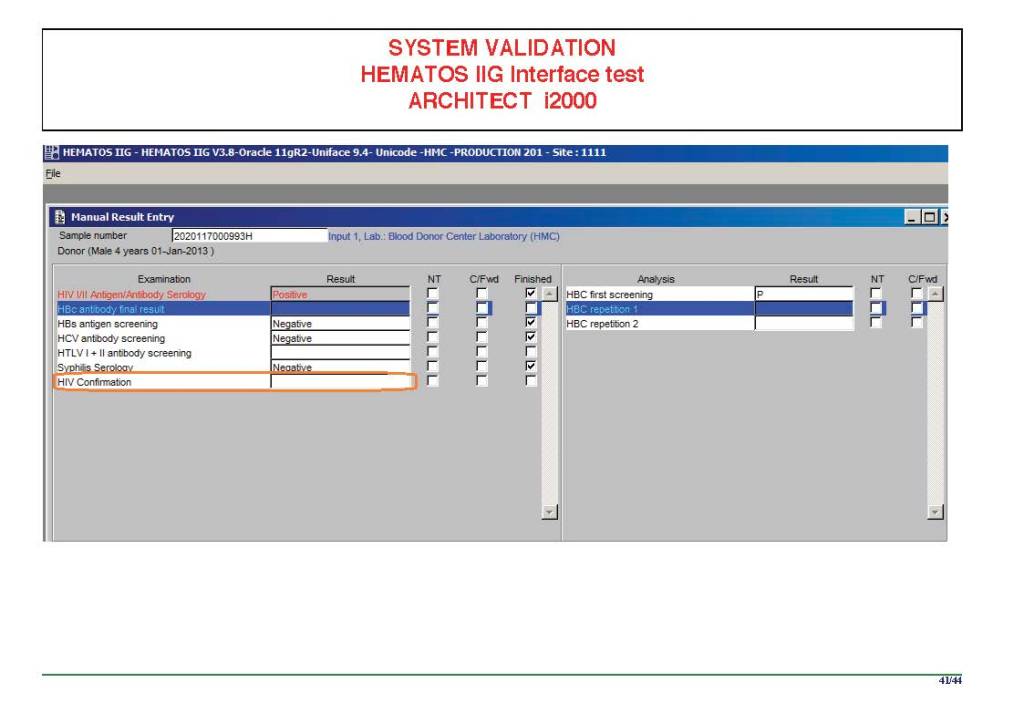
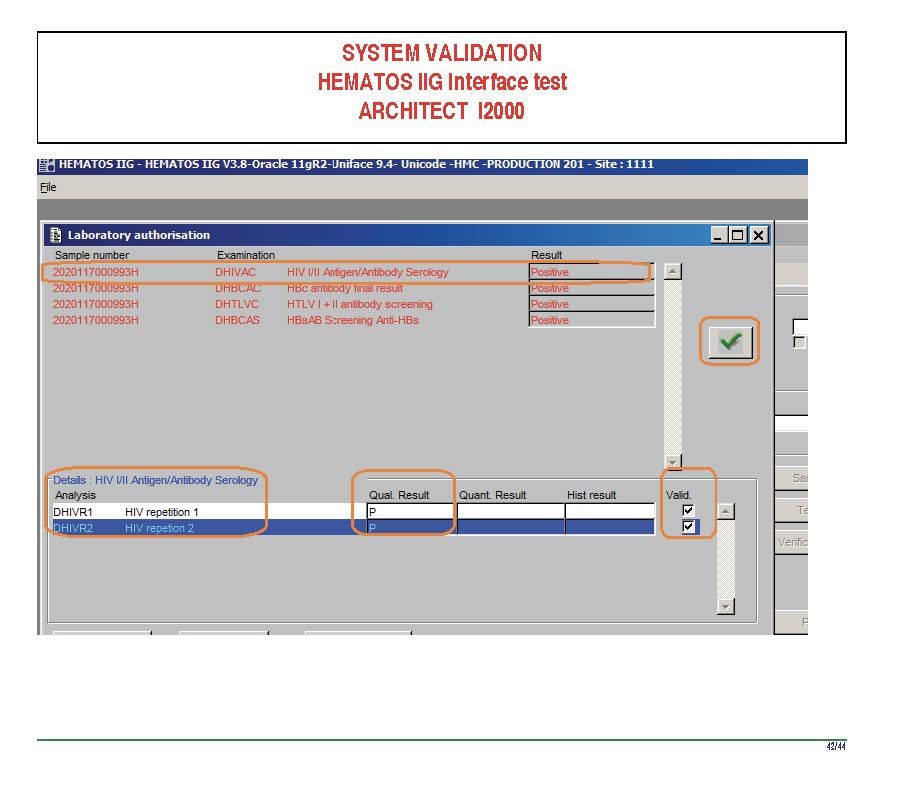
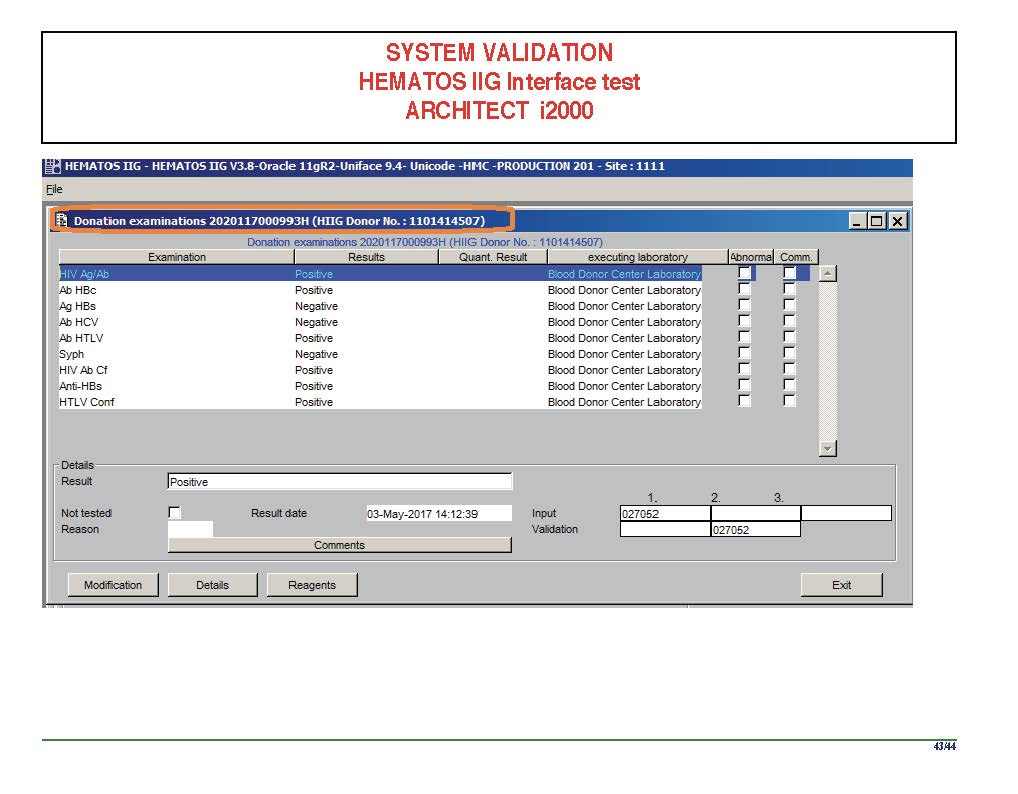
I am attaching a copy of our Abbott Architect interface as updated a few years ago. Again, here I wrote the validation protocol and assigned the tasks to the Medinfo Super Users. To perform this EIA testing, we still had to register donors and collect and then export the specimens to the donor marker testing laboratory before the actual interface testing could begin. This was all done in a special test domain separate from the production domain.
I made the validation criteria and reviewed all data as Division Head of Laboratory Information Systems. Representative screen shots were made. All data was sent to me. My final acceptance was required before the interface could be activated.
Automated component processing (Reveos) and component modification are more complicated and will be covered in a future post.
Yesterday’s post showed my active blood inventory management scheme for my previous position in Qatar. I thought today I would elaborate on how I adjust the inventory based on critical shortages and planning for disasters and other major events.
I always review the critical shortages to check for atypical usage (e.g. a disaster situation) or production issues (equipment breakdown, shortage of donors during holiday period).
If it is due to increased utilization, I try to adjust the critical and desirable inventories upward to cover the shortfall for future events. However, it is not always possible if the event is a one-of-a-kind situation unlikely to recur. Also, I must take into account the available resources (supplies, kits, manpower, equipment) to see if I can cope with the increase.
If it is due to resource issues, I see if I can bolster those by recommending increases or improving utilization of what is available.
Very important is through-put: How quickly can I produce components from whole blood or apheresis components? This was one of the major reasons we shifted away from PCR to other NAT testing with single-well processes since to minimize the need to make additional runs (Grifols Panther System). Also, automated component processing can greatly speed production (one Reveos can process four whole blood units in about 23 minutes or about 12 units in 75 minutes.) Those staff can be busy with other tasks while the machines are working.
In the system I developed in Qatar, we could complete processing into components (RBCs, buffy coat platelet pools, leukodepleted plasma)–Reveos 3C Program, all marker and immunohematology testing, leukoreduction of the pools and RBCs, Mirasol pathogen inactivation, and platelet additive solution in as little as five hours!! There is great need for speed in a place that must be 100% self-sufficient in all blood components. We could even further reduce the total processing time if we only made RBCs and plasma, Reveos 2C Program
In rapid turn-around events, it is most helpful to have a robust blood bank computer system that can scale to the challenge. Also, it must mercilessly enforce all the rules starting with donor qualification, screening, collection through testing and production. At times of emergency, it is difficult to meet Good Manufacturing Processes manually.
After each major shortage, I recommend a “post-mortem” analysis of the situation with senior donor and quality staff to analyze our processes and see if we can further optimize them for the future. A report is prepared and reviewed by me as the Division Head/Medical Director of the Blood Bank. If possible, we implement our recommendations. If not, I request additional resources from the Administration.
As regards Disaster Planning, I always asked Administration how many victims did they want to save? When I got the response, I always try to adjust inventory by two extra RBCs and one adult platelet dose (> 2E11) per salvageable victim. This may come at the expense of increased wastage, especially in a region that cannot export the excess, unused stock.
The exasperating issue is that I didn’t get a clear answer on this last point. What number should I use? I made a spreadsheet showing calculations for a variety of endpoints, e.g. 100, 500, 1000 treatable victims and sent this to Administration to consider.
At the time this was written, West Nile Virus WNV, Chikungunya, Dengue, and Zika virus were not considered as high-risk and no testing was done on the blood supply for them. There were policies to check donor history and ask questions about each of these agents.
Note that we used a linear immunoblot assay for HIV 1/2, HCV, HTLV 1/2, and syphilis.
Definitions:
Positive result for EIA means S/CO ratio >= 1.0
Positive result for LIA (linear immunoblot assay) means particular pattern of bands as defined by the manufacturer
Indeterminate result for LIA means presence of bands not meeting positive criteria
Hepatitis B:
HBsAg non-negative, then:
HBsAg positive with HBsAg confirmatory positive, regardless of other results: permanent deferral, refer to Infectious Disease clinic
HBsAg positive with HBsAg confirmatory borderline or negative, repeat all HBV testing after 8 weeks
HBsAg borderline: repeat all HBV testing after 8 weeks
HBV-DNA positive confirmed, regardless of other results: permanent deferral, refer to Infectious Disease clinic
If HBcAb positive, repeat after 8 weeks
Repeat Hepatitis B Testing After 8 weeks:
HBsAg positive with HBsAg confirmatory positive: permanent deferral, refer to Infectious Disease clinic
HBsAg positive with HBsAg confirmatory borderline or negative: permanent deferral, refer to Infectious Disease clinic
HBsAg borderline, permanent deferral, refer to Infectious Disease clinic
HBV-DNA positive confirmed: permanent deferral, refer to Infectious Disease clinic
HBcAb positive or borderline with negative HBsAg and negative HBV-DNA: review HBsAb level:
If HBsAb level >= 100 mIU/mL (100 IU/L), donor may be reentered
If HBsAb level < 100, then recommend to donor to receive booster HBV vaccine
After HBV vaccine administration, retest after 30 days:
If HBsAb level >= 100, donor may be reentered
If HBsAb level < 100, donor is indefinitely deferred
HBsAg, HBcAb, HBsAb all negative: reenter into donor pool
Hepatitis C:
HCV-RNA positive confirmed, regardless of other HCV results: permanent deferral, refer to Infectious Disease clinic
HCV-RNA borderline: repeat all HCV testing after 6 months
HCV-InnoLIA positive, regardless of other HCV results: permanent deferral, refer to Infectious Disease clinic
HCV-InnoLIA indeterminate: repeat all HCV testing after 6 months
HCV-Ab positive, HCV-RNA negative, do HCV-InnoLIA:
If HCV-InnoLIA positive, permanent deferral, refer to Infectious Disease clinic
If HCV-InnoLIA indeterminate or negative, repeat all HCV testing after 6 months
Repeat Hepatitis C Testing After 6 months:
HCV-RNA or HCV-InnoLIA positive: permanent deferral, refer to Infectious Disease clinic
HCV-RNA or HCV-InnoLIA borderline: permanent deferral, HCV infection not confirmed
HCV-Ab positive or borderline without positive HCV-RNA or positive HCV-InnoLIA: permanent deferral, HCV infection not confirmed
HCV-Ab negative, HCV-RNA negative, HCV-InnoLIA negative: reenter donor into donor pool
HIV Testing:
HIV-RNA positive confirmed, regardless of other HIV results: permanent deferral and do HIV-InnoLIA, refer to Infectious Disease clinic
HIV-RNA borderline: do HIV-InnoLIA
HIV-InnoLIA positive, regardless of other HIV results: refer to Infectious Disease clinic
HIV-InnoLIA indeterminate: repeat all HIV testing after 8 weeks
HIV Ab positive with negative HIV-RNA and/or borderline/negative HIV-InnoLIA: repeat testing after 8 weeks
Repeat HIV Testing After 8 Weeks:
HIV RNA positive and/or HIV-InnoLIA positive, regardless of other HIV results: refer to Infectious Disease clinic
HIV-InnoLIA and/or HIV antibodies indeterminate: permanent deferral, HIV infection not confirmed
HIV Ab negative and HIV-RNA negative and HIV-InnoLIA negative: reenter into donor pool
HTLV 1/2 Testing:
HTLV Antibodies positive, then do HTLV-InnoLIA:
HTLV InnoLIA positive for HTLV-1 and/or HTLV-2: refer to Infectious Disease clinic
HTLV InnoLIA indeterminate or negative, repeat HTLV Ab and HTLV InnoLIA testing after 6 months
Repeat HTLV Testing After 6 Months:
HTLV 1/2 antibodies positive, permanent deferral and do HTLV InnoLIA
HTLV 1/2 antibodies indeterminate, permanent deferral and do HTLV InnoLIA
HTLV InnoLIA positive for HTLV-1 or HTLV-2: refer to Infectious Disease clinic
Malaria antigen test positive, refer to Infectious Disease clinic—defer until 3 years after cessation of treatment
Malaria antigen test negative:
Plasma may be collected
RBCs and platelets must be destroyed.
Repeat malarial antibodies after 3 years:
If malarial antibody test positive, donor must not be used for RBC components but may be used for plasma production
If malarial antibody test negative, reenter donor for all components
Defer donor if he has received malarial treatment (not prophylaxis) for 3 years
Perform both malarial antibody and antigen testing:
Defer based on section 5.2
Syphilis Testing:
Syphilis Ab test positive or indeterminate: do InnoLIA-Syphilis test
InnoLIA-Syphilis test positive: permanent deferral, refer to Infectious Disease clinic
InnoLIA-Syphilis test borderline or negative: defer for 1 year, then repeat all syphilis testing.
Repeat Syphilis Testing after 1 Year:
Syphilis antibody testing negative, reenter into donor pool
Syphilis antibody positive or borderline: do InnoLIA-Syphilis test
InnoLIA-Syphilis test positive: permanent deferral, refer to Infectious Disease clinic
If InnoLIA-Syphilis borderline or negative: permanent deferral, syphilis not confirmed, Guidance for Industry, February 2020
References:
Use of Serologic Tests to Reduce the Risk of Transfusion-Transmitted Human T-Cell Lymphotropic Viruses Types I and II, Final Guidance for Industry, February 2020
Draft Guidance for Industry: Recommendations for Requalification of Blood Donors Deferred Because of Reactive Test Results for Antibodies to Human T-Lymphotropic Virus Types I and II (anti-HTLV-I/II), CBER, September 2018
Guidance for Industry: Nucleic Acid Testing (NAT) for Human Immunodeficiency Virus Type 1 (HIV-1) and Hepatitis C Virus (HCV): Testing, Product Disposition, and Donor Deferral and Reentry, US Department of Health and Human Services, Center for Biologics Evaluation and Research CBER, May 2010
Guidance for Industry: Requalification Method for Reentry of Blood Donors Deferred Because of Reactive Test Results for Antibody to Hepatitis B Core Antigen (Anti-HBc), US Department of Health and Human Services, Center for Biologics Evaluation and Research CBER, May 2010
I am an independent consultant in Transfusion Medicine. Effective 16 April 2020, I am no longer associated with Hamad Medical Corporation or the State of Qatar.
I am willing to consider other opportunities in Transfusion Medicine (donor, patient, apheresis) and blood bank informatics.
Just before leaving HMC, I established the COVID19 convalescent plasma program with full good manufacturing practices using Medinfo Hematos IIG blood bank software.
I have 10 year’s experience in pathogen inactivation and blood component automated production. I established the first site using Terumo Atreus (later Reveos) with Mirasol pathogen inactivation AND platelet additive solution. I established Medinfo interfaces with all production equipment to achieve GMP.
I have worked with laboratory information systems, especially but not limited to blood bank systems (donor, component processing, donor marker testing, pathogen inactivation, platelet additive solutions) and serve as the Head of the Medinfo IIG (Nice, France) Software Users Group.
I was involved with planning for the national plasma fractionation project in Saudi Arabia. I have worked with this industry while I was practicing in the United States.
It is my philosophy to start with an international framework (e.g.FDA, CE) and localize it for the country’s particular needs. My operation sites have served as international reference sites for combined IT and medical/technical processes.