In February 2020, I established COVID-19 plasma collection and distribution for the state of Qatar. Here is a research paper prepared in conjunction with the Qatar Communicable Disease Center about using it for patients there.




Includes compatibility testing (AHG, electronic, immediate-spin), antigen typing, antibody screening and identification, direct antiglobulin testing, elution, transfusion reaction and drug reaction workups, component typing tests upon receipt in hospital blood bank, release and return of components
In February 2020, I established COVID-19 plasma collection and distribution for the state of Qatar. Here is a research paper prepared in conjunction with the Qatar Communicable Disease Center about using it for patients there.
Principle:
The physician on-call for the blood bank requires a certain minimum amount of data to determine the significance of a suspected transfusion reaction and to decide if further testing is required.
Policy:
There are many types of antiglobulin reagent available which have differing specificities to immunoglobulins (e.g. whole molecule IgG, IgG-heavy-chain specific, IgM-heavy-chain-specific, IgA-heavy-chain-specific) and complement fragments (e.g. C3b, C3c, C3d).
For the purpose of antibody identification using the indirect antiglobulin test IAT, normally polyspecific, whole molecule IgG, and/or gamma-heavy-chain-specific reagents are used.
The purpose of antibody identification is normally to detect clinically significant antibodies—NOT ALL ANTIBODIES. In a busy hospital blood bank, I am not routinely interested in detecting cold antibodies that do not react at 37C.
Polyspecific reagents will detect both complement and/or immunoglobulin and are commonly chosen. However, the complement may detect insignificant cold antibodies that may obscure clinically significant IgG antibodies.
A whole-molecule IgG reagent is not really monospecific since it detects both heavy and light chains. The light chains (kappa and lambda) are shared by all classes of immunoglobulin. Thus, an IgM antibody (usually cold) may show weak reactivity—nonspecific cold antibodies may be detected!
My usual choice is to routinely use a gamma-heavy-chain-specific reagent. I have been using this for many years and it expedites the workflow. The likelihood of missing a clinically significant antibody is rare. In my long career, I have only detected a small number of Kidd antibodies that required a polyspecific reagent with complement.
If there is a nonspecific antibody, I will check the Jka and Jkb typings. If either is negative, I will check for an antibody showing dosage and consider using a polyspecific reagent. I have previously reported such an antibody in an earlier post—it is extremely rare!
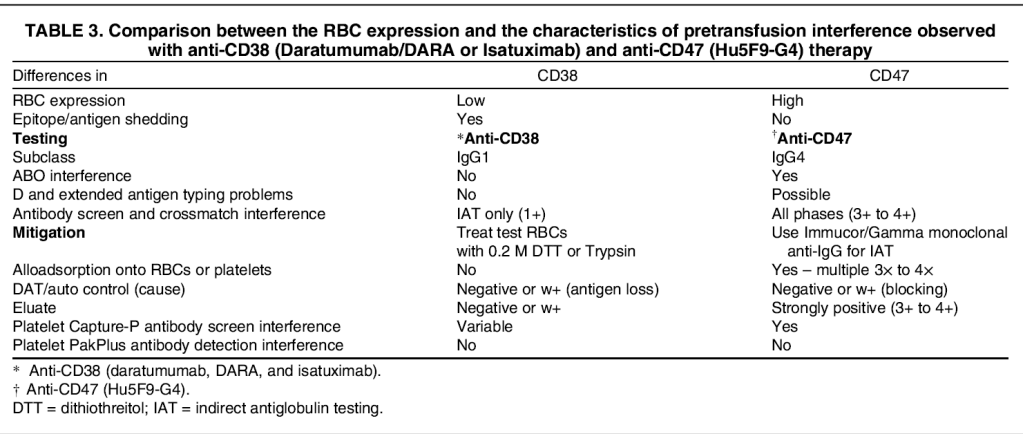
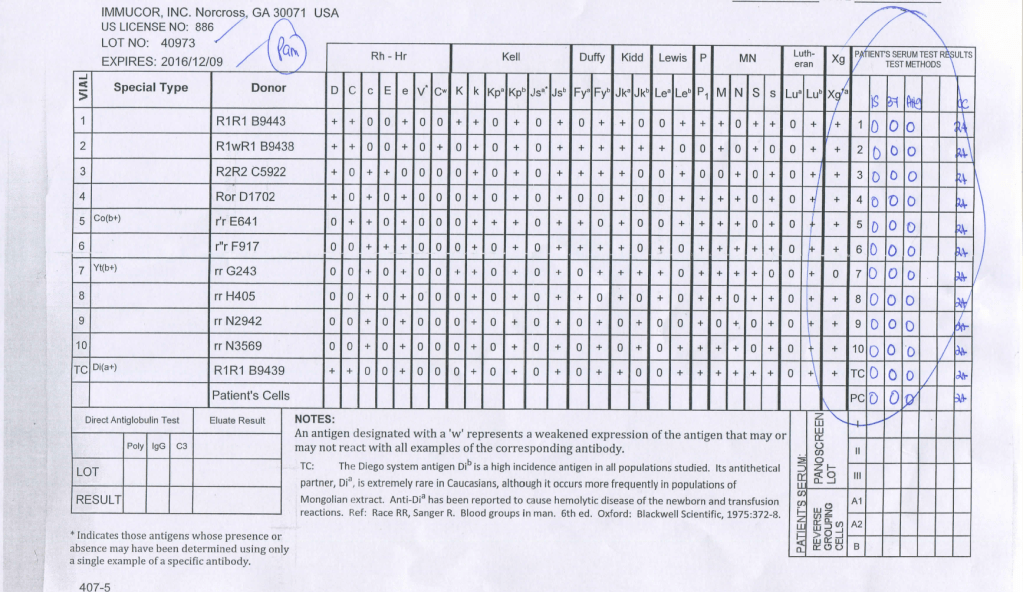
Another consideration is the detection of interference from a new chemotherapy reagent, anti-CD47. This nonspecific reactivity will be eliminated by using a gamma-heavy-chain specific reagent:
This is an example of a nonspecific reagent using whole molecule IgG AHG:
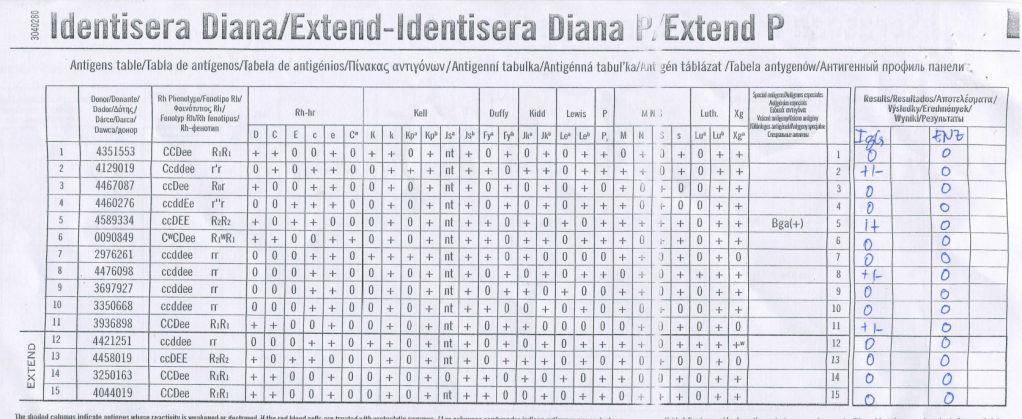
Here is the same sample using gamma-heavy-chain-specific AHG:
4/10/20
Some Possible Explanations:
Always review the transfusion history of all component types, medication history, and the clinical history!! Start with this first.
Can you think of other explanations?
3/10/20
Principle:
Unlike acute hemolysis, delayed hemolysis may be insidious and develop over days to weeks. Likewise severity may vary from asymptomatic but only laboratory-detectable (i.e. delayed serologic reaction) to life-threatening only a few days after transfusion (e.g. an amnestic response to anti-Jka that was undetectable in the compatibility testing several days previously).
Remember that the most severe reactions may occur with weak or negative reactions!!
Policy:
References:
As a transfusion medicine physician, I must know if I can trust my staff’s interpretation of immunohematology testing. I may be called at night and they will provide me with results and I must use these to make a medical judgment. If their interpretation is flawed, I might make a decision that harms the patient.
I really don’t like multiple-choice questions, but nowadays this is often the norm. For my staff, especially senior staff and those who want to be promoted to senior staff, I have developed a series of projective exercises to help me understand their thought processes. I emphasize that I do not want a mere regurgitation of isolated facts: I want integration of the facts into useful information!!
The following is my favorite assessment, offered to advanced staff and candidates for senior technologist, supervisors, and technical manager positions. Usually, these staff have SBB, ART, FIBLS or equivalent qualifications.
You are reviewing abnormal test results and receive the following case:
Anti-A: 4+
Anti-B: 0
Anti-A,B 4+
A1 cells 0
B cells 3+
Anti-D 3+
D-control 0
Antibody Screen: 3+ in SC1 (R1R1), 4+ in SC2 (R2R2), 0 in SC3 (rr)
Antibody Identification: Anti-D
Give possible explanation(s) for this situation. Request any additional information you need.
What blood type will you transfuse?
Solution will follow in a subsequent post.
30/9/20
Principle:
In 1984 effective with the 13th Edition AABB Standards, the requirements for performing a direct antiglobulin test and autocontrol for compatibility testing were eliminated. The DAT is very important to detect delayed hemolytic transfusion reactions, certain autoimmune conditions, and drug-related hemolysis.
Since that time, the immediate-spin crossmatch and now the electronic computer paperless crossmatch may be used for most compatibility testing in place of the classic, antiglobulin-phase (indirect antiglobulin test) crossmatch.
If an antiglobulin phase (IAT) crossmatch is performed, an RBC unit with a positive DAT will cause a false-positive reaction. Since most crossmatching does not include the IAT, it will not be affected by the DAT status of a donor unit.
Policy:
Important: Don’t do a classic AHG/IAT phase crossmatch unless you have to do it (see conditions above.) A donor unit with a DAT is unlikely to be clinically significant and may be transfused safely to the patient in most situations. Patients receiving electronic-crossmatch and immediate-spin crossmatch are receiving units with positive DAT without incident.
References:
As a transfusion medicine physician, I must know if I can trust my staff’s interpretation of immunohematology testing. I may be called at night and they will provide me with results and I must use these to make a medical judgment. If their interpretation is flawed, I might make a decision that harms the patient.
I really don’t like multiple-choice questions, but nowadays this is often the norm. For my staff, especially senior staff and those who want to be promoted to senior staff, I have developed a series of projective exercises to help me understand their thought processes.
Here is another exercise for ABO discrepancies. I offered this to senior technologist and supervisory candidates:
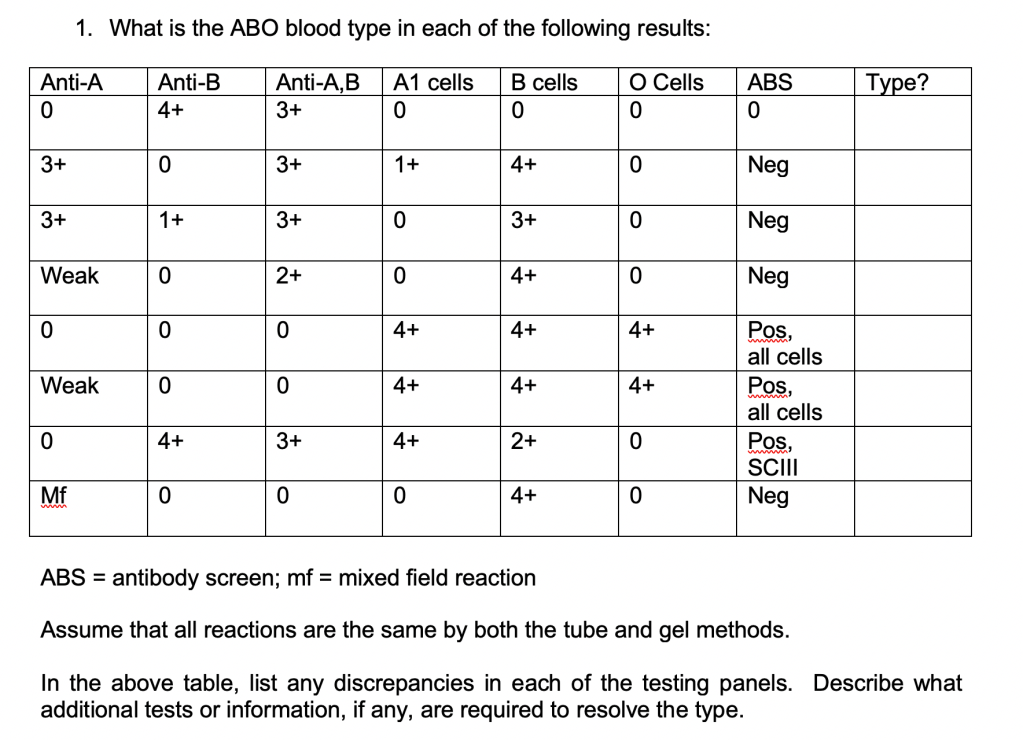
Can they name the conditions that give these results?
23/9/20
Projective Assessment Exercise 6
Zeyd Merenkov, MD, FCAP, FASCP
Independent Consultant in Transfusion Medicine
As a transfusion medicine physician, I must know if I can trust my staff’s interpretation of immunohematology testing. I may be called at night and they will provide me with results and I must use these to make a medical judgment. If their interpretation is flawed, I might make a decision that harms the patient.
I really don’t like multiple-choice questions, but nowadays this is often the norm. For my staff, especially senior staff and those who want to be promoted to senior staff, I have developed a series of projective exercises to help me understand their thought processes.
Here is another exercise using elution:
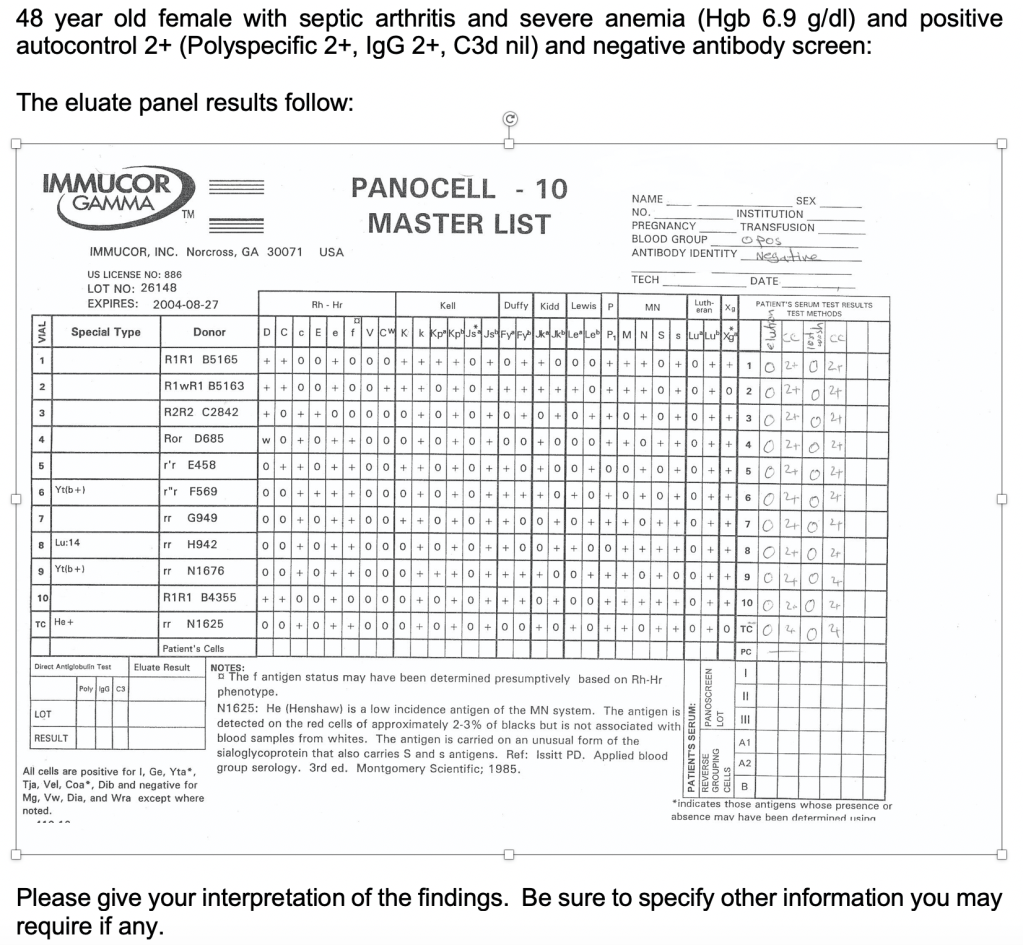
Will they know to get the medication history? What are the mechanisms by which a drug may cause a positive DAT?
21/9/20
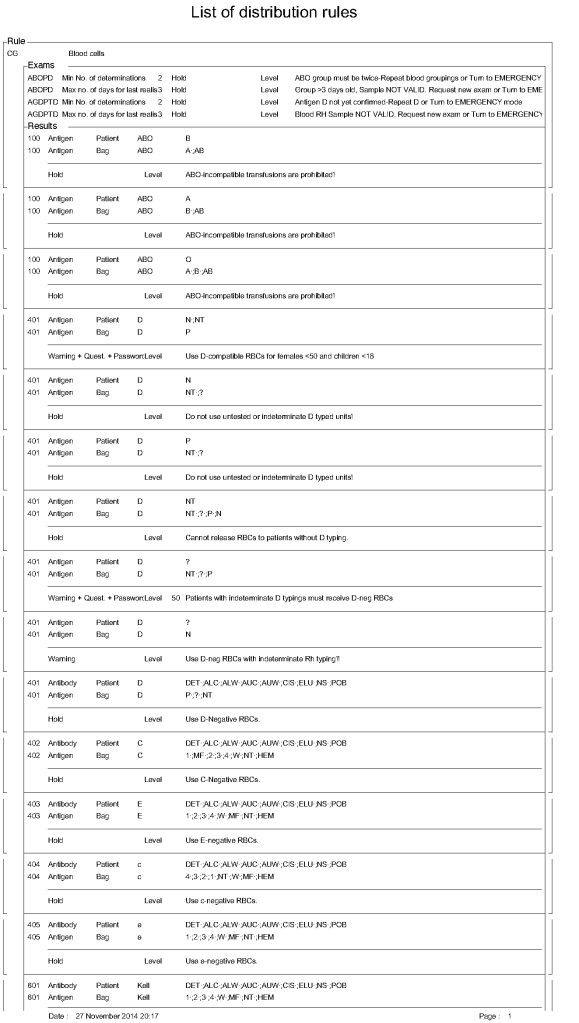
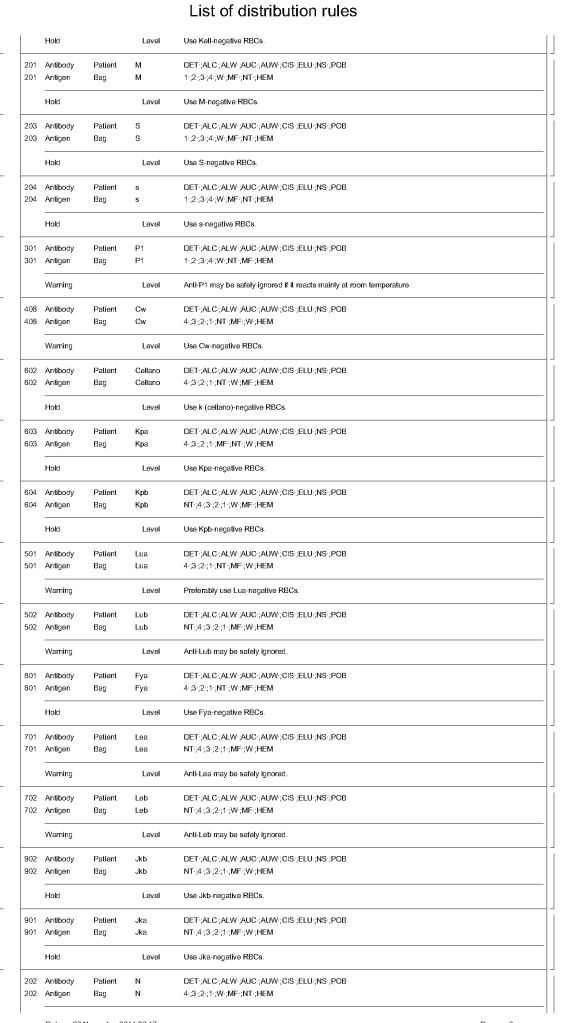
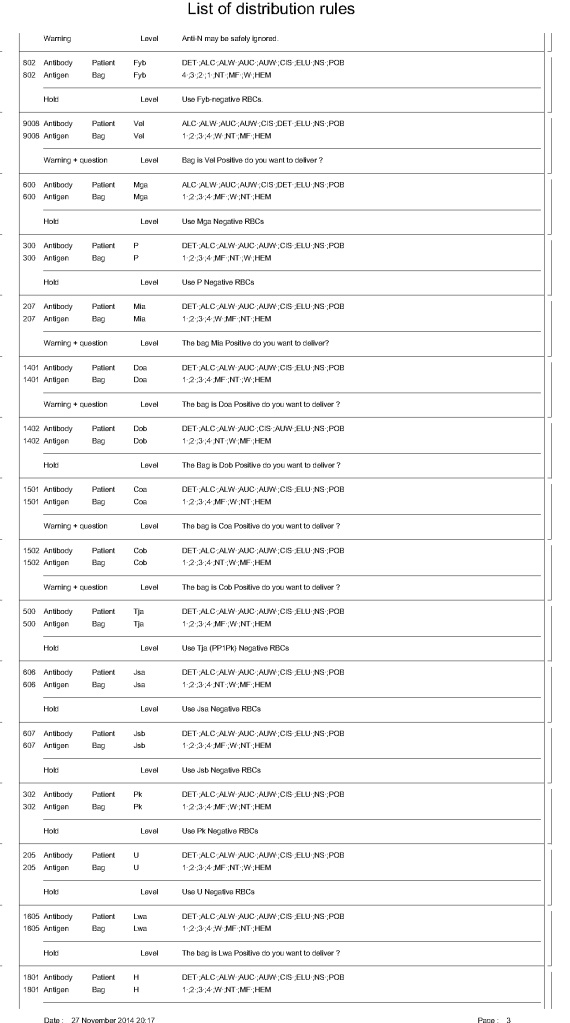
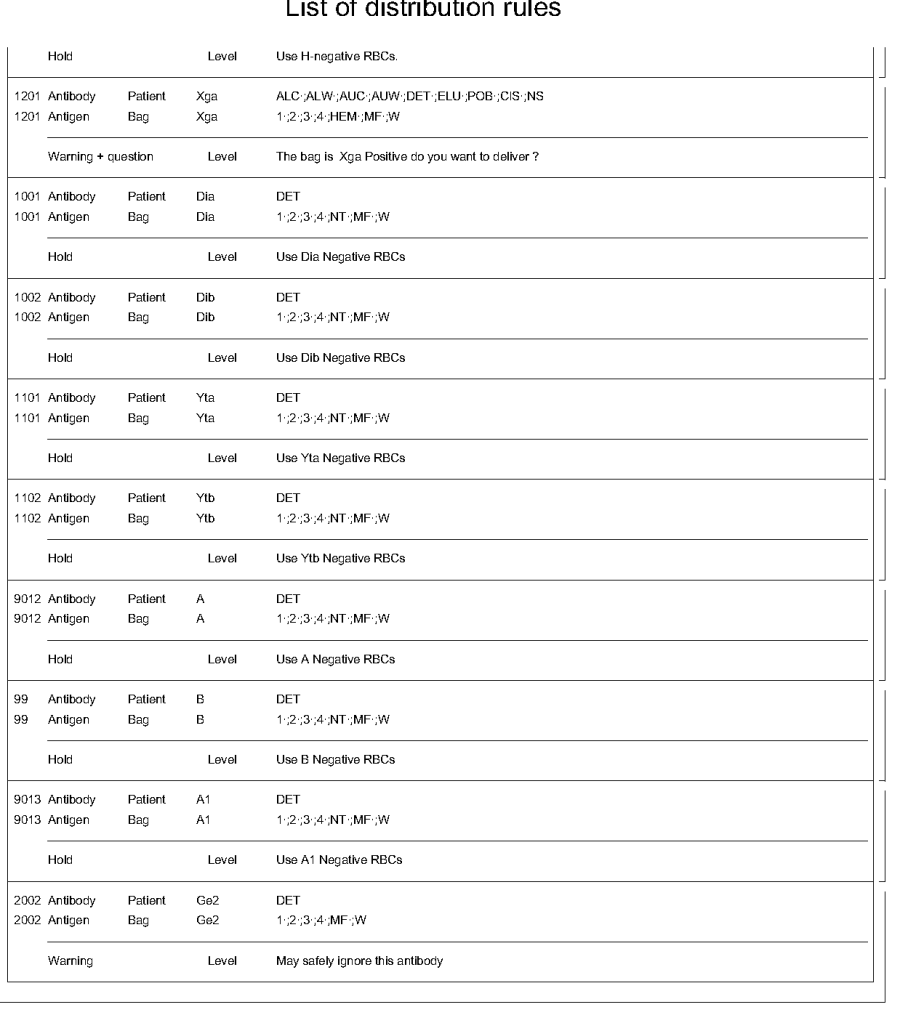
In Medinfo HIIG, one sets parameters to determine which antigens must be matched to allow a RBC product to be released. These criteria may include:
Number of and timing of ABO/D typings
Permissible ABO/D substitutions
Emergency release
Required antigen matches
Optional antigen matches
Exact wording of conditional and blocked combinations
For ABO/D typing, a minimum of two typings must be on record for routine release and the last typing done within 72 hours. If not, emergency release must be selected. ABO-incompatible selections must be blocked. For D-negative patients, only D-typed units may be selected. D-incompatible transfusions will trigger a message to use D-compatible for females <50 years.
Required antigen typings include using antigen-negative for patients having antibodies against the specified antigen, e.g. D-negative RBCs for patients with active anti-D, c-negative for patients with anti-c, K-negative for anti-K, etc.
Certain antibodies will trigger a message to flag the use of unmatched units but not block the release.
The attached document shows sample settings for RBC release. Note that these rules are user-definable.
31/10/20
