This is part 3 of a medical student lecture I gave at National Guard Health Affairs.
Includes registration, questionnaire, physical exam and arm check, collection, marker testing, component separation, donor immunohematology testing
This is part 3 of a medical student lecture I gave at National Guard Health Affairs.
This is the second part of a lecture I gave to medical students at National Guard Health Affairs in Riyadh.
This is an updated version of a medical student lecture I gave at National Guard Health Affairs in Riyadh.
To be continued
5.2.1 PROCESS: DONOR QUESTIONNAIRE
Process:
References:
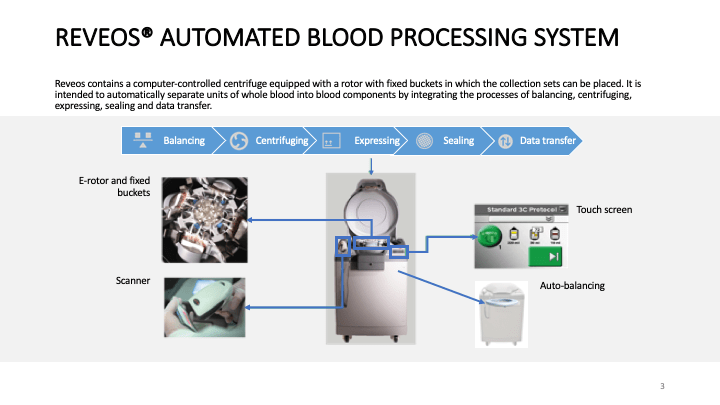
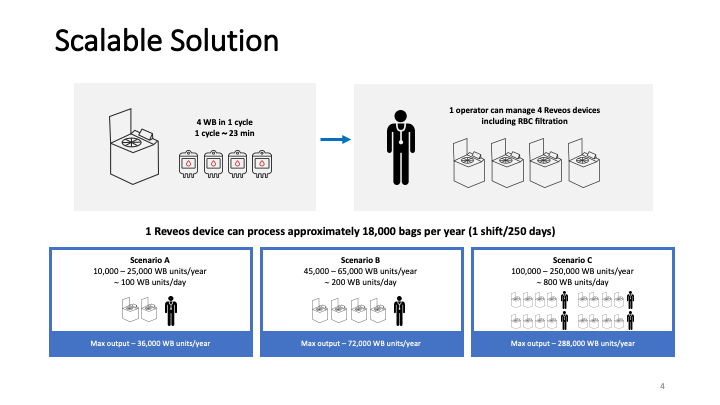
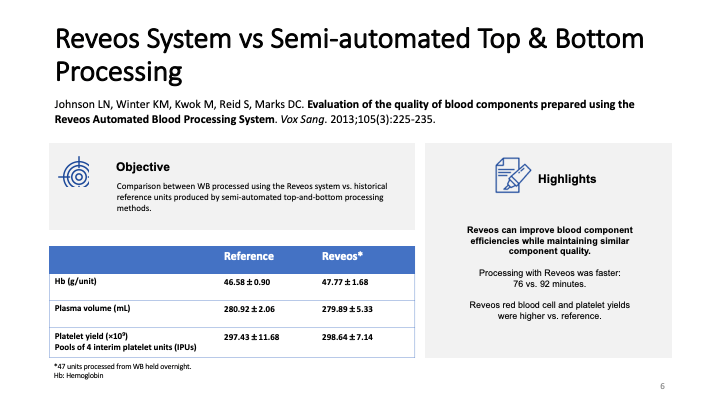
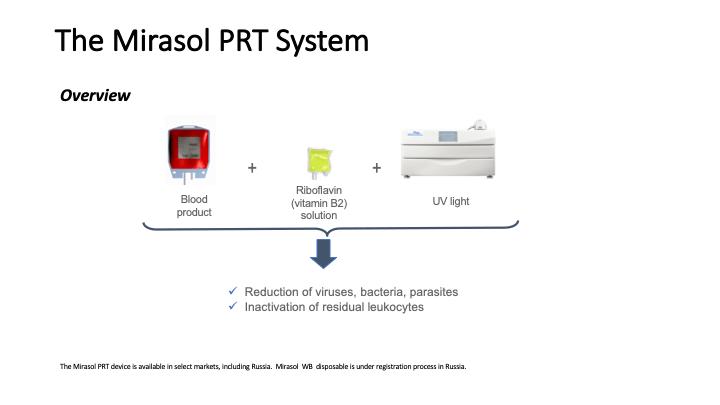
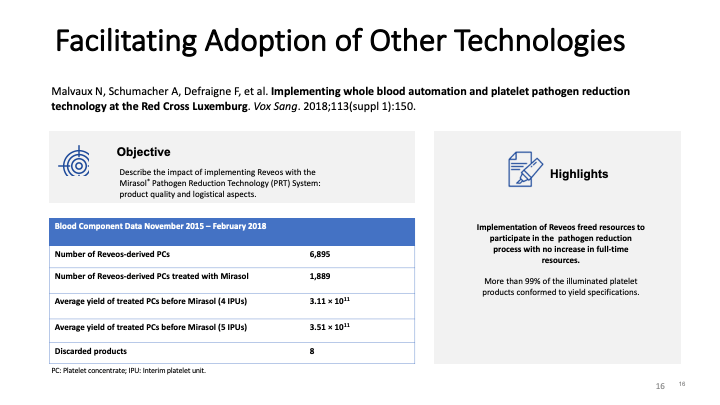
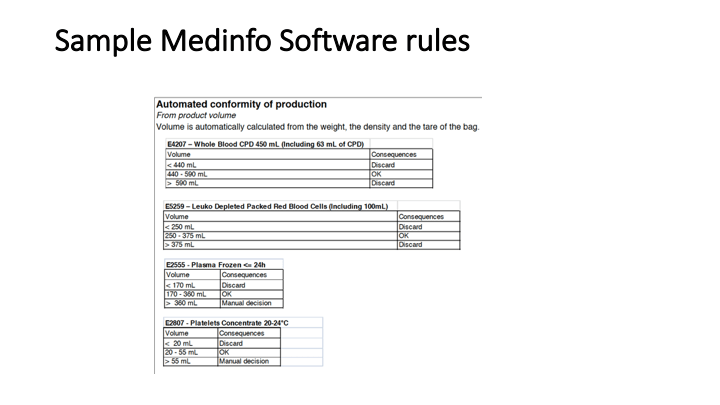
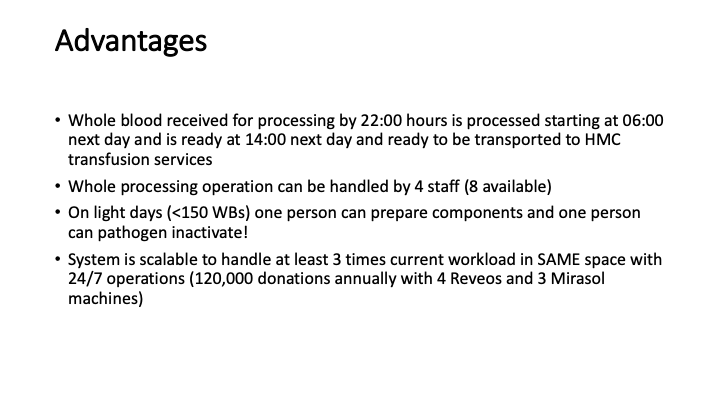
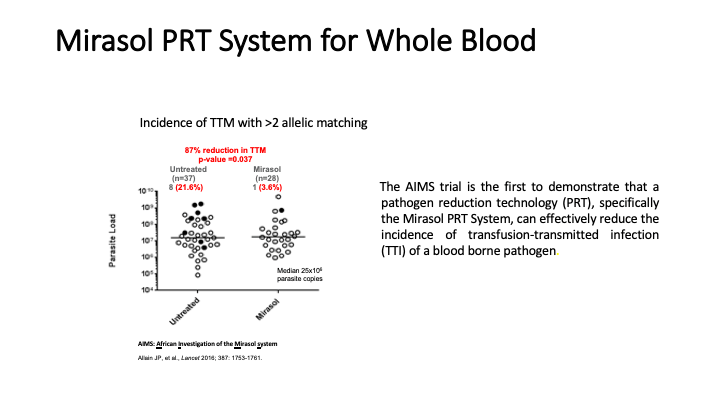
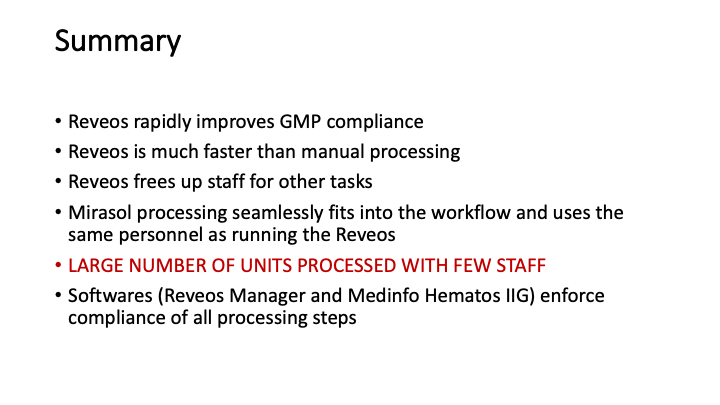
This is the virtual talk I gave at the Russian Transfusion Congress in Moscow on 13 May. It gives a brief description of automated component processing and riboflavin-based pathogen inactivation and then discusses the use of these technologies together to free up labor and enhance the quality of products, i.e. improved GMP, especially if a dedicated blood bank computer system is used to enforce production rules.

Policy Donor Medical Questionnaire
5.2 POLICY: DONOR MEDICAL QUESTIONNAIRE
Policy:
References:
5.1.1 PROCESS: Donor Registration
Process:
References:
Number: 5.1
Policy:
References:
5.0.1 PROCESS: Donor Recruitment and Campaigns
Process:
References:
5.0 Donor Recruitment and Campaigns Policy
Policy:
References:
