This is the final section of this base medical student lecture originally given at NGHA Riyadh. It has been updated to current technologies and current types of blood components.

Includes registration, questionnaire, physical exam and arm check, collection, marker testing, component separation, donor immunohematology testing
This is the final section of this base medical student lecture originally given at NGHA Riyadh. It has been updated to current technologies and current types of blood components.
This presentation was originally given to third-year medical students at NGHA-Riyadh as their first lecture, Introduction to Transfusion Medicine. It has been updated for new component types and will be presented in multiple parts
2011
Established automated component production using Atreus technology, plasma and platelet pathogen inactivation (Mirasol)—made HMC component production Good Manufacturing System GMP compliant
2011
Qatar is the first to adopt non-PCR-based NAT technology (Grifols/Novartis Tigress) and becomes world reference site for this
2011
Based on the above, Qatar can now completely process all whole blood into blood components (red cells, platelets, and plasma) in as little as 5 hours from collection!
2011-2020:
I established policies and procedures for the hospital blood banks/transfusion services, blood donor center, therapeutic apheresis, and laboratory information systems to bring HMC in compliance with the Council of Europe, international AABB, and other standards. I customized our own standards for our local needs based on them.
2012-2013
Implemented custom build of the multilingual blood bank computer system (Medinfo) for both patient and donor services, including development of interfaces to all production equipment including Atreus and Mirasol (world’s first) and a direct link to Ministry of the Interior to obtain patient demographics in English and Arabic—Qatar became the world’s first site to combine fully-interfaced, automated component production with pathogen inactivation: Qatar becomes world reference site for this.
2013-2014
Built, validated, and implemented laboratory build of hospital information system, Cerner Millennium
2015
Replaced and updated Atreus with Reveos automated component production to allow faster throughput and capacity with a full bidirectional interface (world’s first), introduced platelet
additive solution PAS with pathogen inactivation (Mirasol)—Medinfo interfaces updated to Reveos for all equipment: this doubles the capacity to process whole blood into components using the same physical space
2015-2019
Updated dedicated blood bank software Medinfo Hematos IIG by several versions using Division Head, LIS, and internally trained Super Users—at great cost savings to HMC by not using outside consultants (e.g. Dell Consulting)
2019
Established column absorption technology using Terumo Optia therapeutic apheresis machine for treatment of ABO-incompatible renal transplants: I validated using the Ortho Vision MAX to perform ABO antibody titers for this system and correlated it with the reference method at Karolinska Institutet in Stockholm (manual gel) to bring rapid throughput and labor savings—Qatar being the first-site in the world to do this. We saved money by using the same apheresis machine to use this column absorption technology (no need for second machine to use the columns)
2020
Expedited setup (two weeks total) of COVID-19 convalescent plasma production, initially manual and then fully integrated into the Medinfo computer system as a customized module with separate quarantine collection, production, and transfusion service functions
Other:
I was awarded two HMC Star of Excellence Awards:
2013—Liver Transplantation Transfusion Support
2019—ABO-Incompatible Renal Transplantation Support
This presentation was originally given to third-year medical students at NGHA-Riyadh as their first lecture, Introduction to Transfusion Medicine. It has been updated for new component types and will be presented in multiple parts.





This presentation was originally given to third-year medical students at NGHA-Riyadh as their first lecture, Introduction to Transfusion Medicine. It has been updated for new component types and will be presented in multiple parts.
This presentation was originally given to third-year medical students at NGHA-Riyadh as their first lecture, Introduction to Transfusion Medicine. It has been updated for new component types and will be presented in multiple parts.
The AABB just updated its Ebola Toolkit and made proposed changes to the Uniform Donor Questionnaire UDQ to reflect this. Up to five (5) questions should be included in your questionnaire. What question(s) to use depends on:
| Yes | No | |
| Ebola Question 1: Have you ever had Ebola virus disease or infection? | q | q |
| Ebola Question 2: In the past 8 weeks, have you lived in, or traveled to, a country with widespread transmission of Ebola virus disease or infection? (Review list of affected areas, as classified by CDC) * | q | q |
| Ebola Question 3: In the past 8 weeks, have you had sexual contact with a person who has EVER had Ebola virus disease or infection? | q | q |
| Ebola Question 4: In the past 8 weeks, have you had direct exposure to body fluids (blood, urine, stool, saliva, semen, vaginal fluids or vomit) from a person who may have Ebola virus disease or infection, including a person under investigation? | q | q |
| Ebola Question 5: In the past 8 weeks, have you been notified by a public health authority that you may have been exposed to a person with Ebola virus disease or infection? | q | q |
If the response to question #1 is YES, then the donor is indefinitely deferred.
For questions 2-5, there is an 8-week deferral.
In areas with no widespread transmission, self-deferral of donors with a history of Ebola infection should be adequate, only question #1 is required. If there is widespread transmission, questions #2-5 should be added. Four (4) weeks after widespread transmission stops, revert back to using question #1 only.
These can be easily added to the donor questionnaire in Medinfo blood donor module.
References:
These are the answers to the previous post.
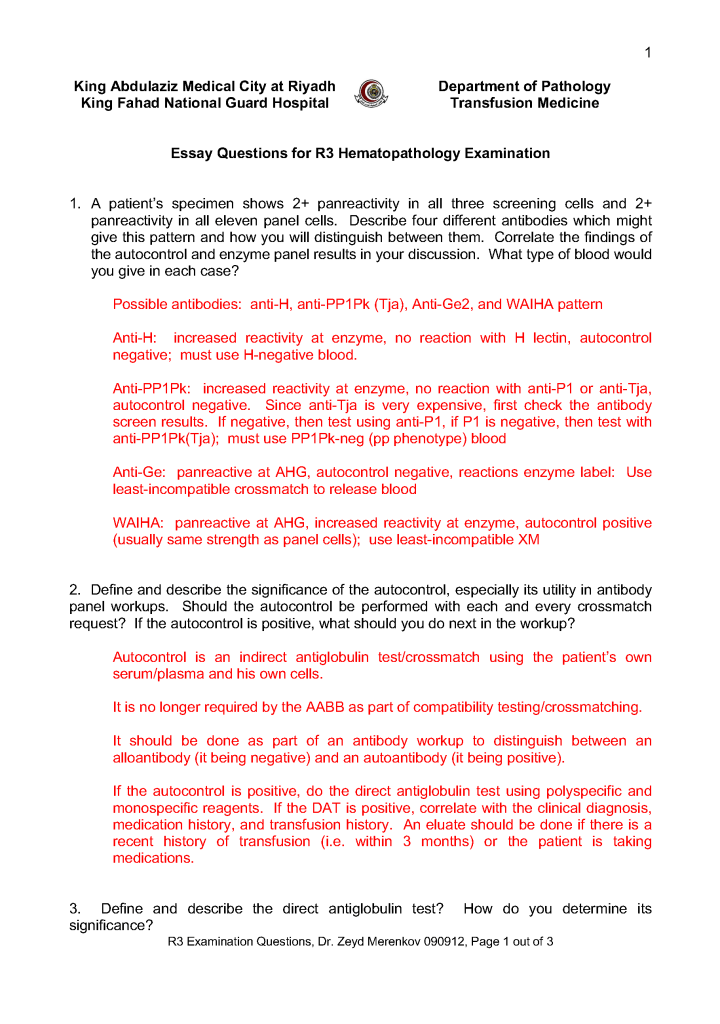
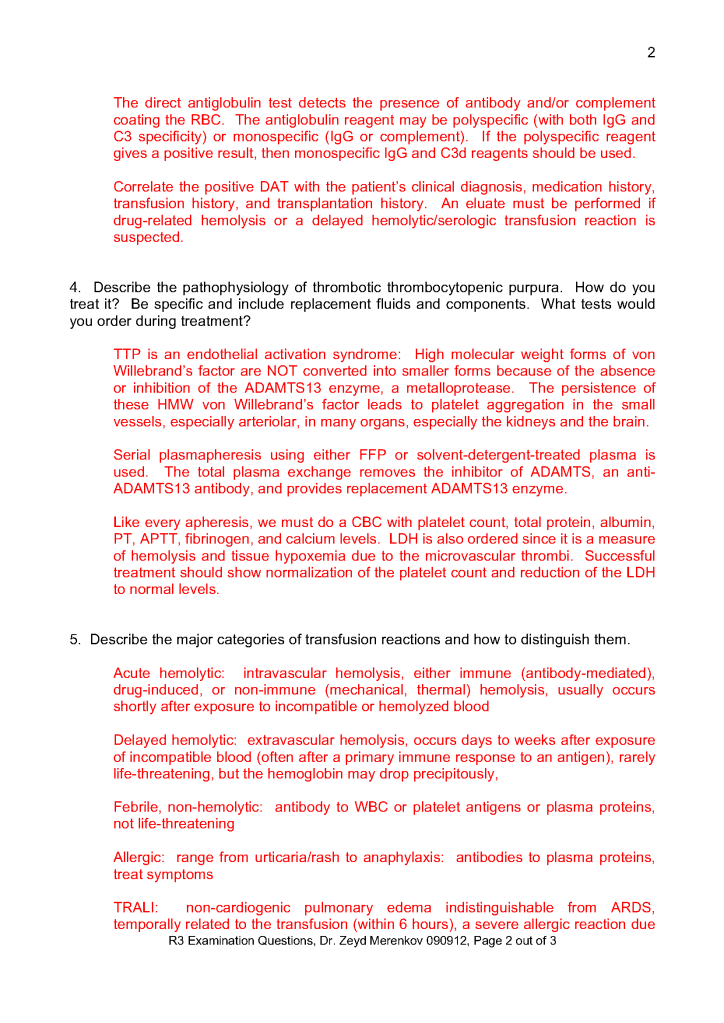
This is the third-year hematology fellow examination I prepared for NGHA Riyadh:
This is a post of an old teaching presentation for pathology residents, hematology fellows, and transfusion medicine fellows from my time at NGHA-Riyadh.