I prepared the following plan for a CCP program for HMC Qatar in March, 2020. The workflow is divided into four (4) modules:
- Registration/Interview/Physical Examination/Apheresis Collection
- Donor Marker Testing and Immunohematology Testing
- Production/Aliquoting/Pathogen-Inactivation/Storage
- Product Thawing/Product Release
Module 1:
- Collection/registration/screening must be in a separate area from regular blood and apheresis donations.
- Donors must provide consent.
- ISBT specimen labels must be used on each tube collected.
- We need a minimum of two apheresis nurses, one for the registration/screening/post-donation observation and one for the actual apheresis procedure.
- If there will be multiple serial donors, then we need a waiting area (each donor at least 2 meters apart).
- Donor screening must be in sound-proof area so that other waiting donors cannot hear the interview/questionnaire process.
- Amount that can be collected depends on body weight: 500 ml for <80 kg and 600 ml for >= 80 kg, collection may occur twice per week
- Collection time includes 15 minutes for registration/interview/physical examination, 60-75 minutes and 15 minutes for cleanup/disinfection before the next case, approximately 2 hours per donation.
- A post-donation observation area (minimum 15 minutes after collection) with apheresis nurse nearby in case of reactions is needed if there will be multiple donors.
- Specimens will
Module 2:
- Donor testing and donor immunohematology will be done with other donor specimens in our regular location
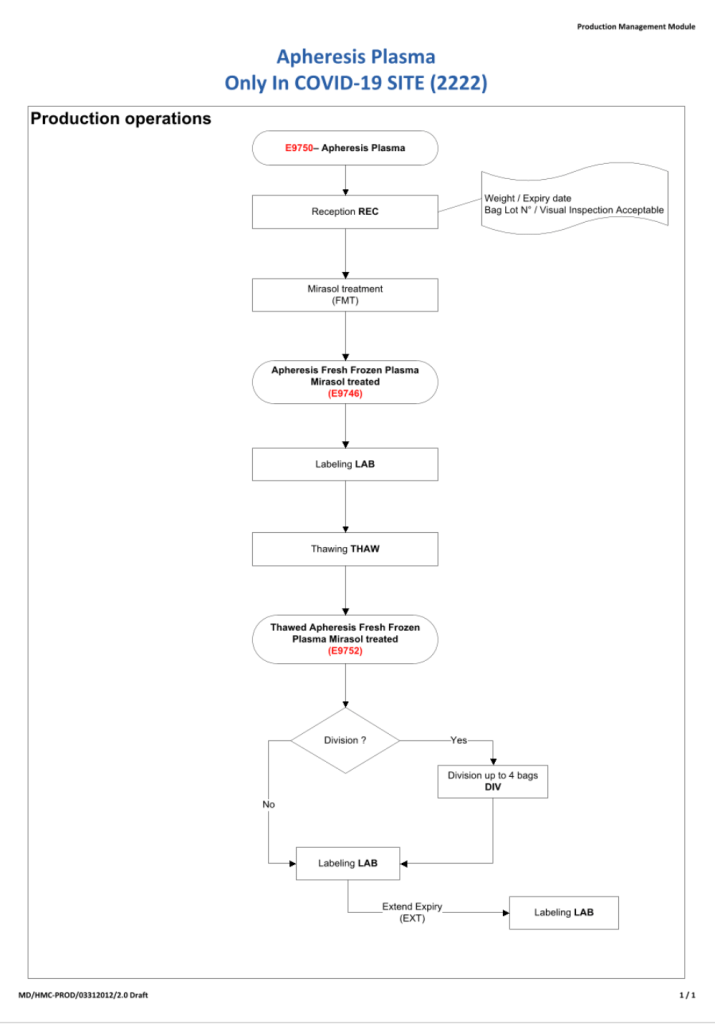
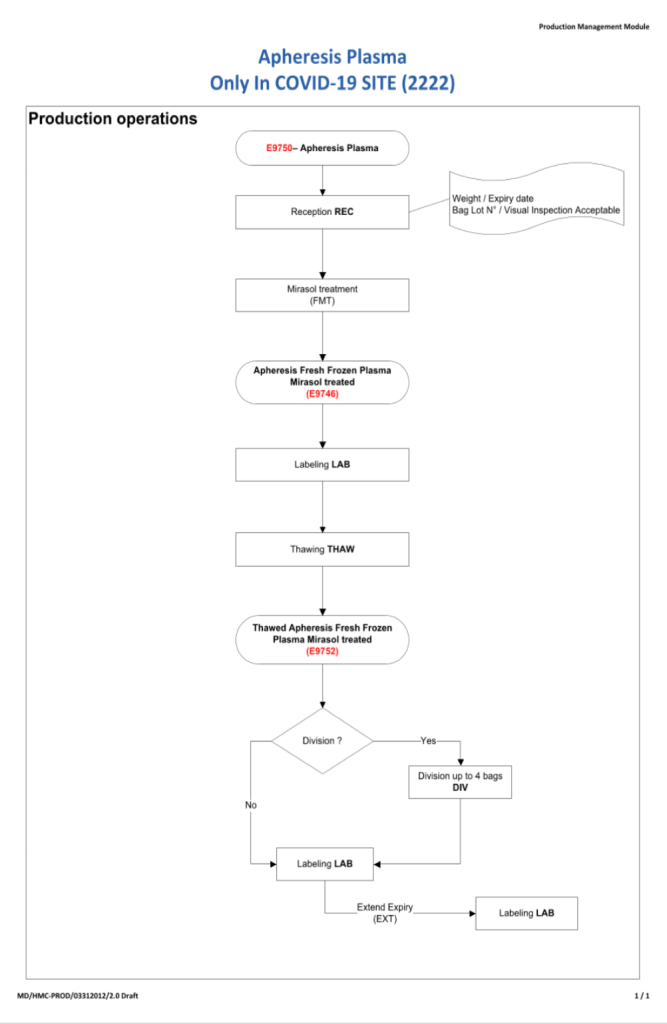
Module 3:
- Apheresis collection must be processed and stored separately from regular blood/apheresis donations.
- Processing will occur only after the results are shown to meet all criteria.
- Pre-collection testing (test-only donation) would permit processing without waiting for results.
- Storage at minus 80C may be for a minimum of six (6) years but this may be extended if needed.
- All acceptable components will have a final ISBT label—no products without the ISBT label will be transfused. The ISBT label indicates that the unit meets all donor criteria for convalescent plasma.
Module 4:
- Product modification (thawing) and release (sign out from blood bank) must be in a separate area(s) from the regular hospital blood bank.
- Release of convalescent plasma follows the same process as regular component release
- Transfusion of convalescent plasma at the patient’s bedside follows same process as regular component transfusion
- Nursing and other staff performing the transfusion must pass competency assessment.
- Plasma will be transfused as ABO-identical or compatible unless low ABO-titer group A is used.
- Plasma must be free of clinically significant antibodies
Workflow Considerations:
- Donors must be restricted to the waiting, collection, or post-donation observation areas.
- Donors must NOT pass through production, testing, or component release areas (just as they are currently restricted in the Blood Donor Center and HMC hospital blood banks/transfusion services).
Logistics:
- Throughput is a maximum of 4 donors (2000 to 2400 ml plasma) per eight-hour shift with one apheresis nurse and one donor apheresis (Trima) machine.
- The processes are scalable with additional staff and machines (e.g. with 3 machines and nurses, then 12 donors and 6000 to 7200 ml of plasma collected).
- Thawing of 1-2 units of plasma takes up to one hour. Contact the quarantine blood bank at least one hour before the desired pick-up time.
- The four modules above can be in separate areas not adjacent to one another. Modules 1, 3, and 4 must be quarantine areas where access is limited. Module 2 can be performed with regular donor specimens using standard precautions.
- We can provide training for transfusion of blood components and competency assessment to any location transfusing this product.
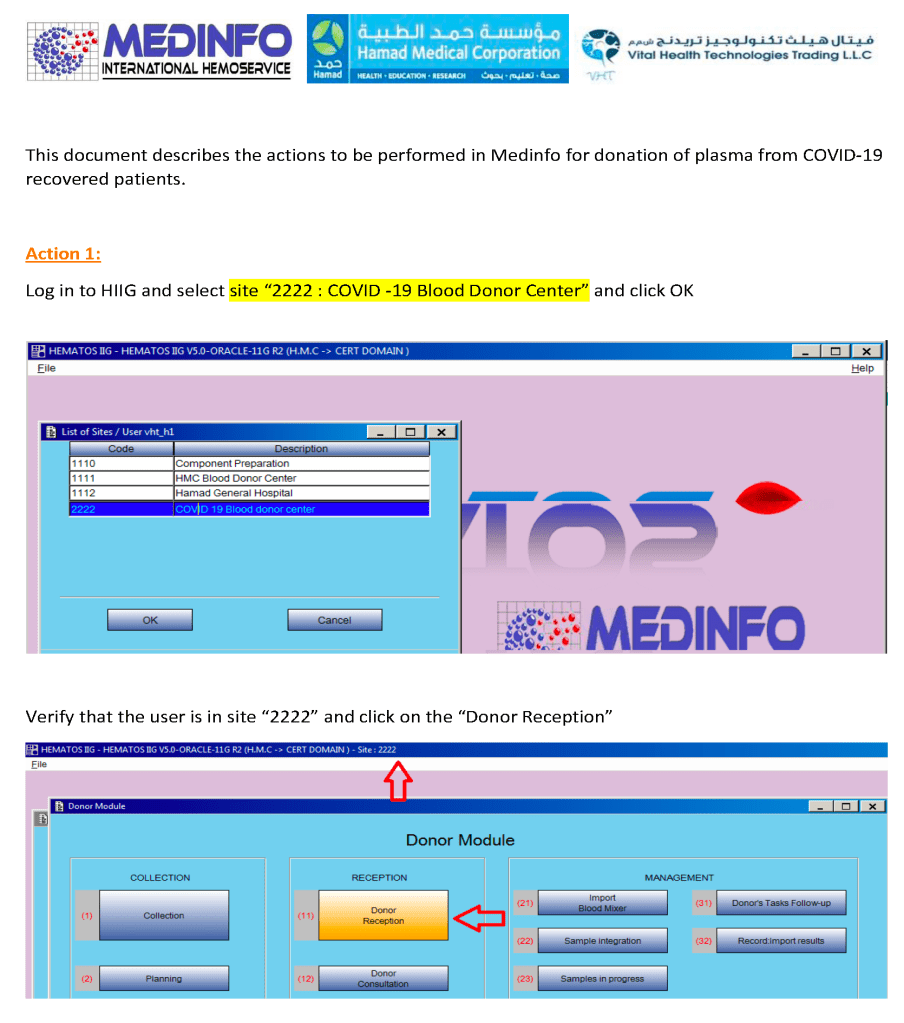
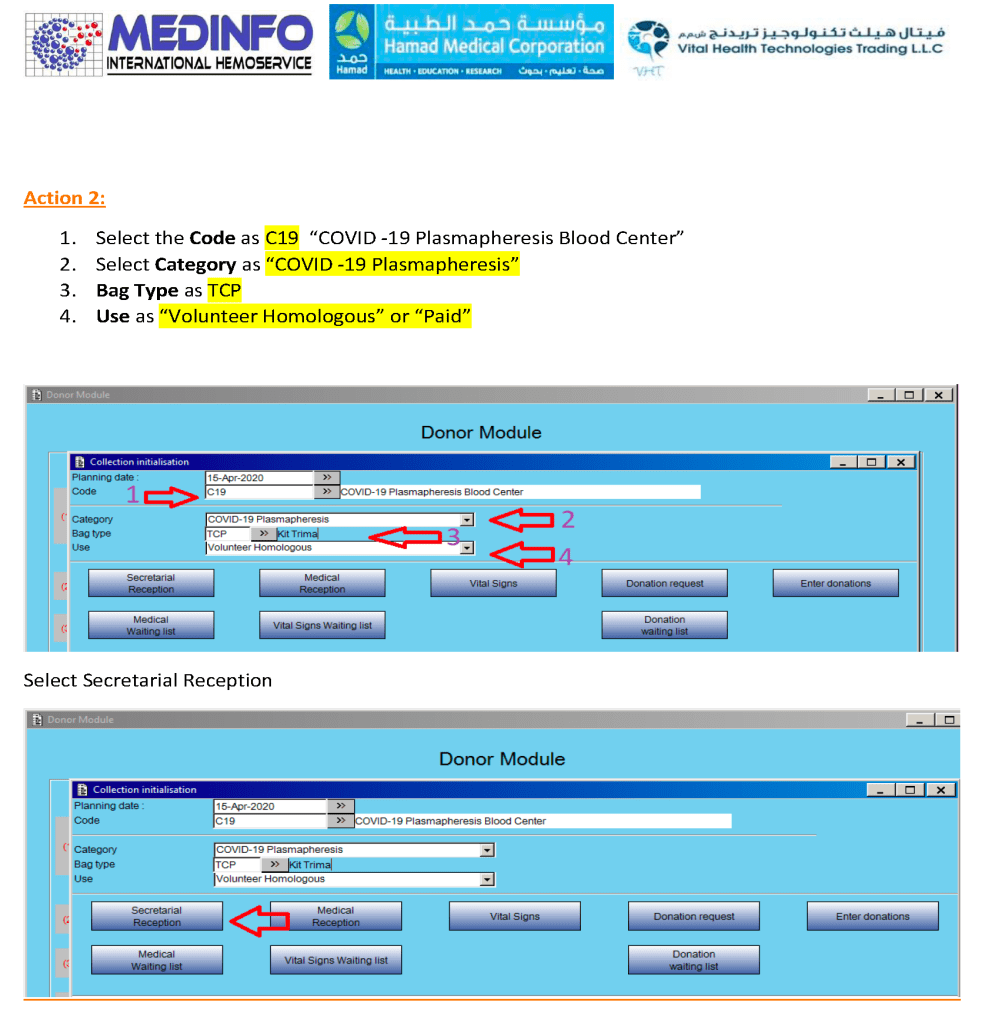
Information Technology:
- All modules will be connected to the Medinfo Hematos IIG dedicated blood bank computer system.
- All records of collection/production/testing/storage/modification/release will be stored therein.
- All ordering of convalescent plasma components will be through Medinfo.
- External test results (e.g. future antibody titering) can be added to the component information.
- Links to the Hospital Information System (Cerner) may be considered after the Medinfo processes are fully functional.