Principle:
ISBT labels are ONLY GENERATED THROUGH MEDINFO HEMATOS IIG SOFTWARE. We do not buy preprinted labels or have a separate label-generating program. ISBT labels are only attached to blood components after production of new or modification of existing blood components and are only printed if the Good Manufacturing Process GMP criteria are met and confirmed by the software.
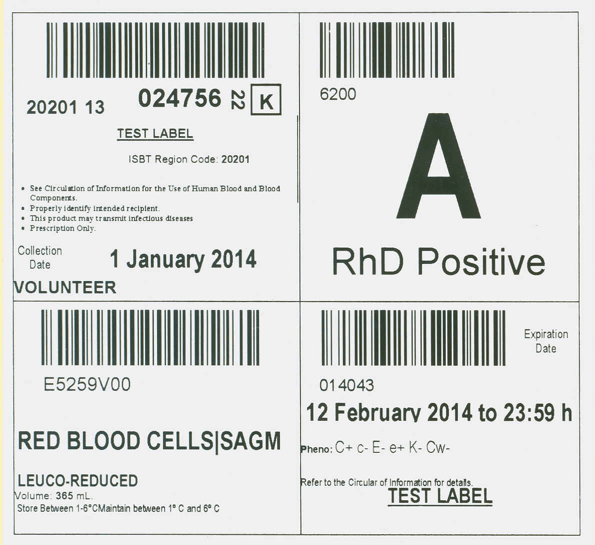
The ISBT component label measures 10 x 10 cm and is divided into FOUR quadrants:
- Upper left: Donor Unit number: 20201 (site location) then two digits for the year (e.g. 13) followed by the donor encounter number followed by a check digit. Reference is made to the Circular of Information, patient identification, risk of disease transmission, and prescription-only status.
- Upper right: ABO/D type
- Lower left: E code corresponding to the component type specification, the designation of origin (volunteer vs directed vs autologous vs paid donation) plus the division number. E codes are taken from the ISBT master database. We use CE-approved codes (NOT US FDA).
- Lower right: Expiration date and time using 24 hour system plus any other phenotype data and other testing.
ISBT Specimen Labels:
ISBT specimen labels are used for all samples at the time of donor collection and include a separate check digit to confirm that the barcode is properly read. ISBT specimens can be used in all parts of Medinfo Hematos IIG software; however, non-Medinfo systems not complying with the safety features of the Council of Europe (worst case scenario is Cerner Millennium and all other American software) may not be able to read them.
Since we do not preprint ISBT labels, there are no phase-out of labels, they are only printed immediately upon need. As component production changes frequently, the actual ISBT designation from the ISBT database for the new component is used by Medinfo.
Policy:
- All blood components and solvent-detergent treated plasma SDP must be labelled with ISBT labels.
- All donor specimen labels must meet the ISBT standard, including the check-digit.
- No blood components may be dispensed to patients unless there is an ISBT label corresponding to the final component, including ALL modifications (aliquoting, irradiation, washed, pathogen-inactivated, etc.)
- No one should write anything on an ISBT label: If there has been a change in the component, perform the modification through Medinfo HIIG and reprint the label.
- Do NOT attach any other labels to an ISBT label.
- Ensure that the final ISBT label at the time of dispensing is on-top of all other ISBT labels.
- The ISBT sequences will be reset each year at 2359 hours on 31 December by the Medinfo software engineer.
- The choice of E codes is made by the Division Head, Transfusion Medicine/LIS using the ISBT master database.
References:
- Guide to the Preparation, Use, and Quality Assurance of Blood Components, European Committee (Partial Agreement on Blood Transfusion, CD-P-PS, Current Edition
- Standards for Blood Banks and Transfusion Services, Current Edition, AABB, Bethesda, MD, USA
- TRM.43600 and 43625 CAP Checklist, 2016