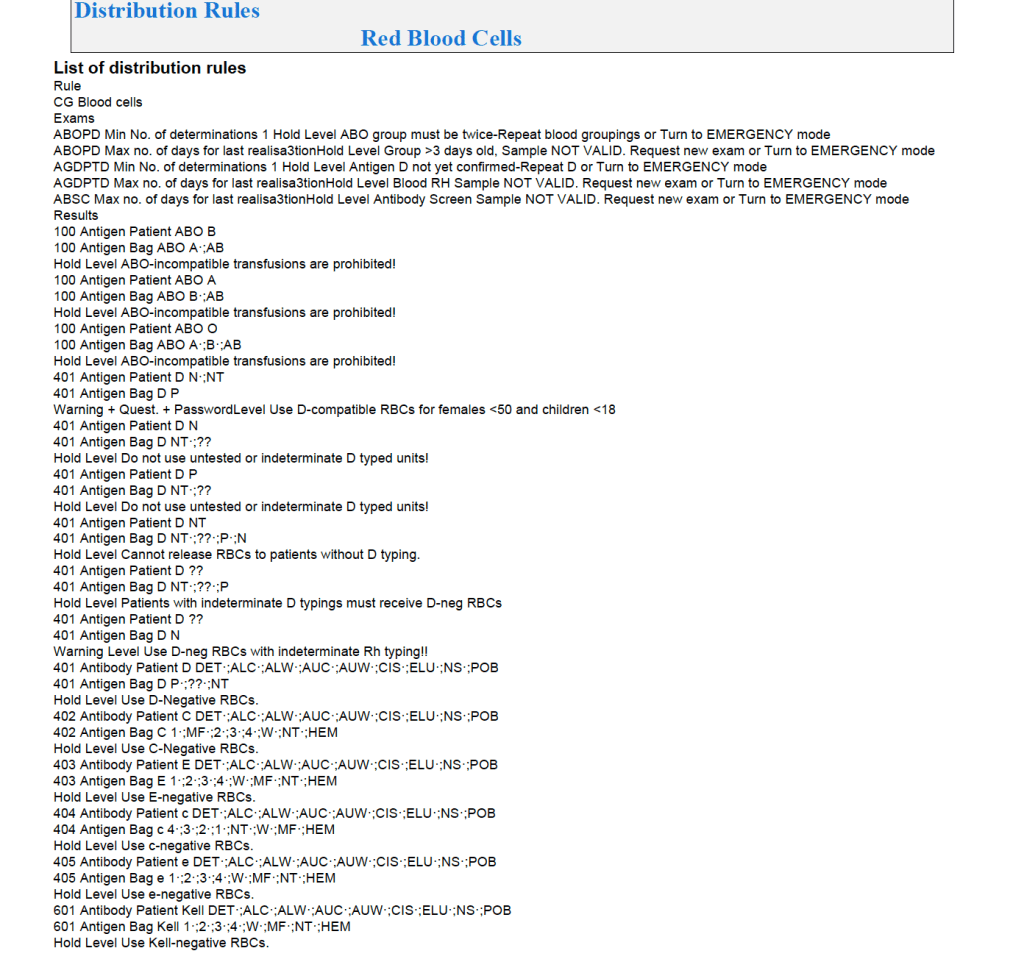
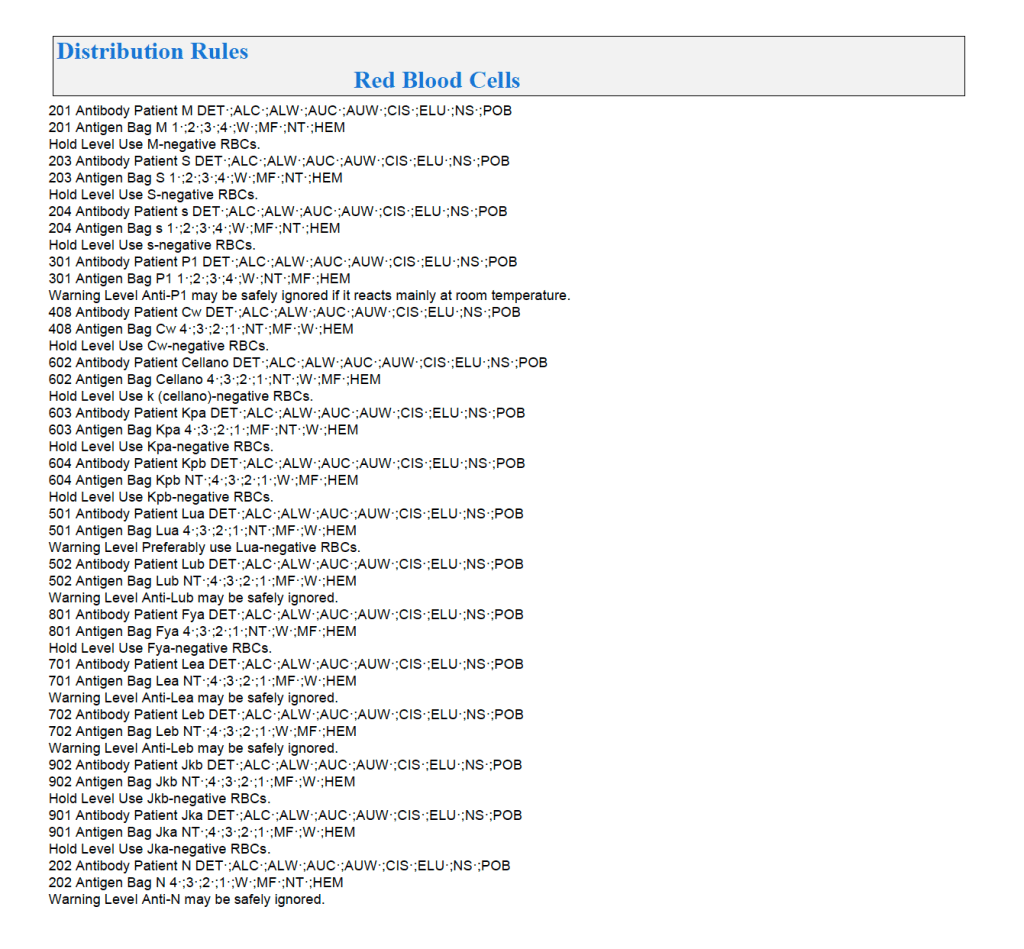
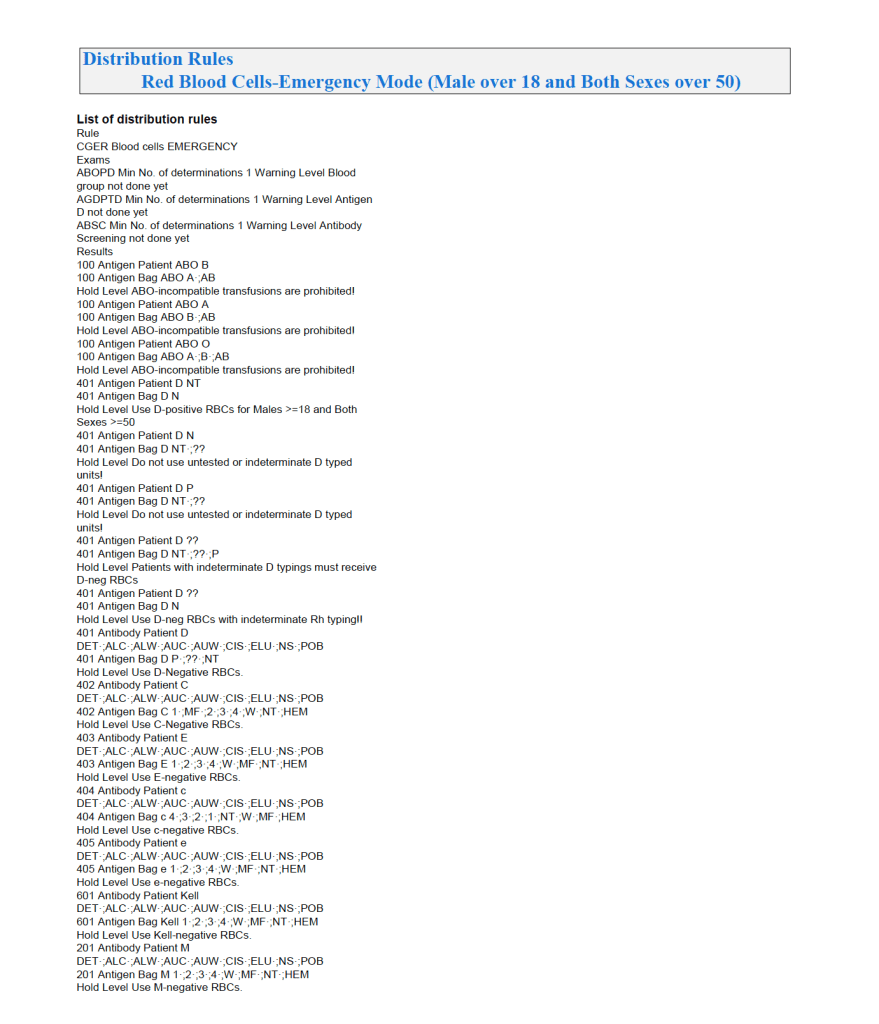
In the previous post, the Medinfo document for Inter-Depot transfer had many pages of rules for matching RBC antigens. Multiple actions were available:
- Forced Match, no release of untested or antigen-mismatch (e.g. anti-Kell requires specifically tested K-negative RBCs).
- Match Optional (e.g. anti-Lea/Leb does not require Lewis-matched blood): system would flag a comment showing the antibody specificity, user would respond Y/N, and select units
- Least-Incompatible (e.g. WAIHA): requires sufficient privilege (senior technical or transfusion physician) to authorize release
- Permitted Incompatible (e.g. give C-positive to patient with anti-C in times of shortage or complex multiple antibodies without fully matched blood available): requires sufficient privilege to release
- Fully Allowed (e.g. group O RBCs to group A, AB, B patients)—no flagging, allocation of units permitted
- Prohibited Under Any Circumstance—NO Override Permitted (e.g. group O for Bombay Oh, c-positive for anti-c, K-positive for anti-K)
To avoid mistakes, the blood bank computer system enforced the rules. There was no mercy. Only specific individuals could override this( in many cases, but certain allocations (e.g. group O RBCs to a Bombay Oh patient) were not permitted under any circumstances.
Prophylactic Antigen Matching:
Please also refer to my prophylactic antigen matching post made last week for the rules I selected for Qatar.
Prophylactic antigen matching is common in Europe. I have been doing this during the many years I have worked in the Middle East. Most patients were not local nationals but transient. They would return to their home countries where blood bank testing (antibody screening/identification/antigen matching) or intrauterine exchanges might not be always available.
For pregnant patients, we would prophylactically match K-negative and c-negative—regardless if there were antibodies detected—R1R1 units for R1R1 patients. At the end of my time in Qatar, we had several pregnant women with various Rh deletions, so we added routine extended Rh(D) and Kell typing to all.
For sickle cell patients, especially African type, I would prophylactically match Rh antigens (D, C, c, E, e) and Kell because of the polymorphisms in the CE gene, some of which may lead to pan-Rh antibodies.
I would consider selective prophylactic antigen matching in chronically transfused populations, again regardless if clinically significant antibodies were detected.
If a patient makes any antibody, regardless if is clinically significant or not, I would consider that patient as a candidate for prophylactic antigen matching (but NOT necessarily for a clinically insignificant antibody).
In Qatar, blood bank services (testing and components) were not charged to the patient. In many other parts of the world, blood bank is a cost center. No prophylactic antigen matching may be routinely performed. If it is done, it must be charged to the patient or the hospital must assume the cost. I have gone to conferences in such locales where not even R1R1 patients were not matched and subsequently developed anti-c, which complicated management. It would have been cheaper to do the antigen matching than to pay for the consequences of the alloimmunization.