In my long career, there have been cycles in transfusion practice. Today’s dogma becomes yesterday’s heresy and then later again the dogma. Just consider the selection of blood components before the introduction of cyclosporine for intended renal transplant recipients.
In training, I was told NEVER, NEVER use the intended donor’s blood for the renal recipient. This would immunize him against the donor tissue antigens and cause the transplant to fail.
Several years later after cyclosporine, we were doing a booming business of directed RBC transfusions from the donor to his/her recipient.
Just a few years ago, I used blood component therapy for all, especially trauma patients. Give the victim what he lacks: for oxygen-carrying capacity, RBCs; for volume crystalloid; for low protein albumin; for coagulopathy FFP, factor concentrates, cryoprecipitate; for thrombocytopenia, platelets.
Most recent studies now mention the danger of giving too much crystalloid, etc. It talks about using fresh whole blood to provide all of the above in less volume. Results from trauma and military studies are encouraging and may be better than individual component therapy.
There are special considerations for whole blood:
21-day outdate for the RBCs
Platelet functionality limited after 7 days
Use of group O, low-ABO-titer
Pathogen-inactivation of whole blood is CE-approved by riboflavin (Mirasol). Terumo BCT is developing an exciting technology to first use Mirasol and then make components using the Reveos automated component system—RBCs, plasma, and platelets. This is an ongoing project so for now the only CE-approved project is use as whole blood. Such Mirasol-treated whole blood has been shown to prevent malaria transmission in Ghana.
From my review of the literature, these are my specifications as of this date 18/8/20:
Use/ordering restricted to trauma and selected ICU/surgery suites
Only male donors
7 day outdate
Group O, Anti-A and anti-B IgM titers, both <= 1/256
Leukodepleted < 1E6 residual WBCs
What level of anti-A and anti-B titers is acceptable? The titer was set as low as 1:32 but at recent THOR meeting 1:256 has been used. In Qatar in a pilot study, I found that about 50% of our donors had titers < 1:256. The issue is that each time the donor presents himself/herself, we must repeat the titer—it is not stable.
Of course, performing even just a saline-titer is time consuming. The only practical way for us in Doha would have been to use an automated titration option on an immunohematology analyzer—in our case, the Ortho Vision MAX, which could perform 1 titration run in about 30 minutes, and the instrument cannot be used for any other testing during the process.
I personally would perform leukodepletion to conform to CE, but you need a special whole blood filter that removes WBCs butspares the platelets. Terumo BCT has such a filter that achieves <1E6 residual WBCs. Never use a standard RBC leukodepletion filter since it will remove BOTH platelets and WBCs—this would defeat the purpose of using whole blood.
At HMC Doha, female donors were only used for packed RBC production—all plasma and platelets were discarded. Some centers do HLA antibody screens and allow negative females to donate.
Finally, many groups do not leukodeplete at all. I am concerned about the risk of adverse reactions and TRALI so I would conform to CE and do it.
Whichever conditions you stipulate, it is easy to create the process in Medinfo. The most important thing is to know what you want to specify.
Transfusion Medicine includes laboratory and non-laboratory functions. The non-laboratory and purely clinical functions are unique and have no analogy within the general laboratory.
The transfusion service/hospital blood bank laboratory is the closest to a laboratory operation, but there is component modification and complex manual testing, especially for reference immunohematology testing. The staff must make detailed manual decisions, the errors for which could be life-threatening for the patient.
The blood donor center manufactures a pharmaceutical, i.e. blood components with collection, donor qualification, donor abnormal results review, infectious disease marker testing, component production, and donor immunohematology testing—all subject to Good Manufacturing Practices. Never forget: Blood is a drug!!
No other laboratory section is directly responsible for treatment of critically ill patients. Therapeutic apheresis is essential for organ and stem-cell transplants, nephrology, neurology, etc. No other laboratory section is directly responsible for treatment of critically ill patients. Transfusion Medicine physicians are functioning as intensivists. There is no hiding in the laboratory from clinical medicine.
There may also be an industrial manufacturing plant to extract various blood derivatives (e.g. factor concentrates, albumin, Rh immune globulin, etc.) This is pharmaceutical manufacturing on a large-scale basis. There is medical, technical, and special administrative expertise.
Many functions may operate 24/7. The transfusion medicine physician may be on-call for donor issues and review of complex immunohematology problems to acutely decide which blood component (and phenotype) should be given as well as review all adverse reactions to transfusion.
The unique blend of clinical skills is unlike anything else in the laboratory. Also, those outside the blood bank rarely have the skills or judgments for the best course of action for transfusion medicine or for its operations.
The clinical transfusion medicine physician must make acute, life-threatening decisions unlike anyone else in the laboratory. The blood bank technologist is at the cutting edge of the battle with his testing and interpretations. No other area of the laboratory is at such risk for injuring or even killing the patient. There is high stress and burn-out.
I have talked with many blood bankers and many seem to share the exasperation that the laboratory does not understand us. The latter looks at blood bank testing like that coming off a hematology or chemistry analyzer—although patients rarely would have severe morbidity or mortality like the blood bank from errors in those analyzers.
No laboratory pathologist has the pressure of the blood bank physician on-call. It really is 24/7 and requires a broad, clinical background to make the right decisions. It is very stressful and does not permit a good night’s sleep.
Thus, I make my case to separate us from the laboratory. We can form our own more effective administrative organization and optimize our own planning. Regretfully, I have never worked in such an administrative structure. I also am a realist that cost-containment nowadays makes it much less likely high administration would permit this change for a mere cost center. This will probably never happen during my career.
Finally, Transfusion Medicine is an essential service. Blood components are essential drugs. The operations and staff must be free of political influences. This is a service for the entire region or country like the fire department, civil defense, etc.
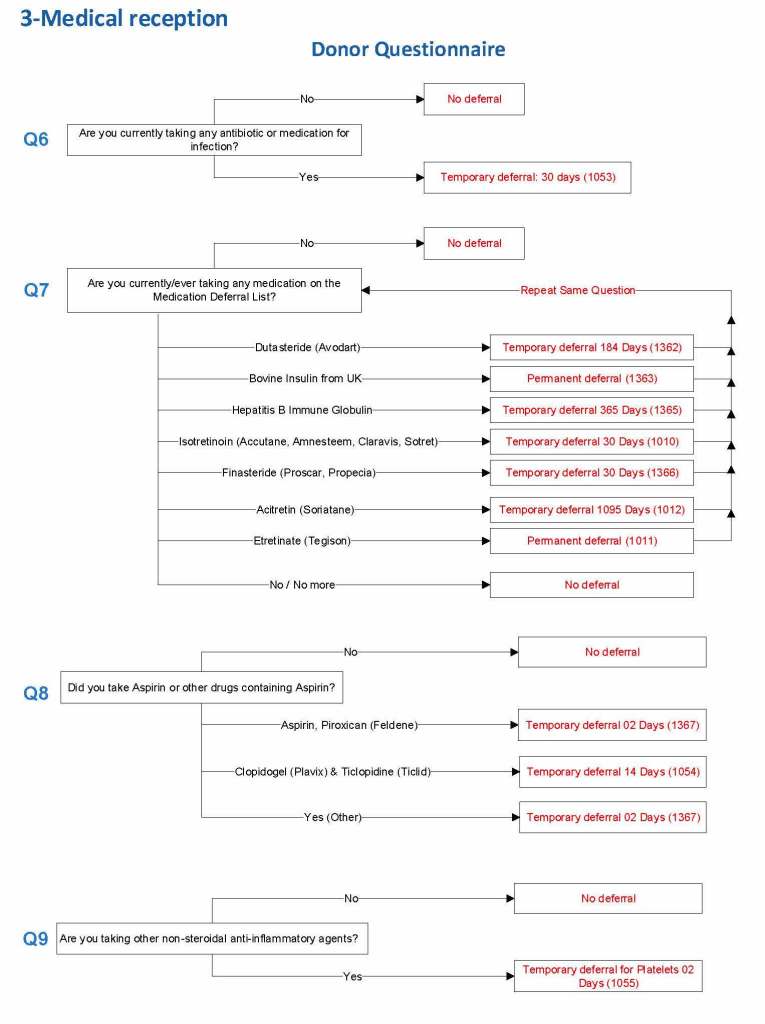
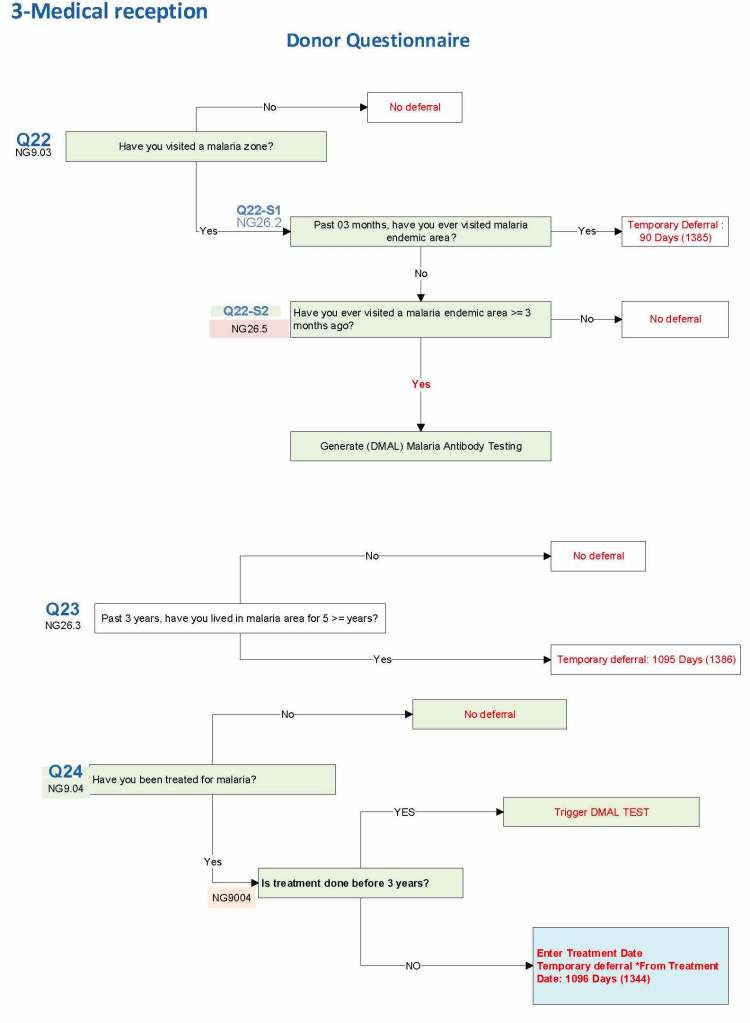
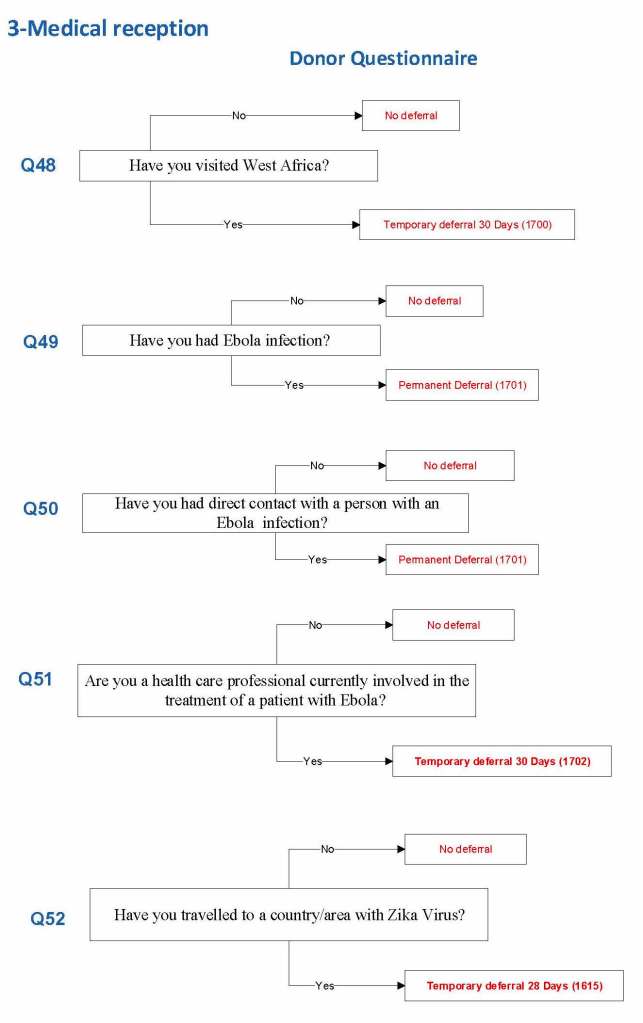
I started building this using the Uniform Donor Questionnaire UDQ from the AABB; however, I modified it to include coverage for Chikungunya, Zika, etc. and to include enhanced processes for malaria based on the Australian Red Cross.
For each screening question, I prepared the exact wording (usually the UDQ’s) and set the deferral to temporary (how many days) or permanent.
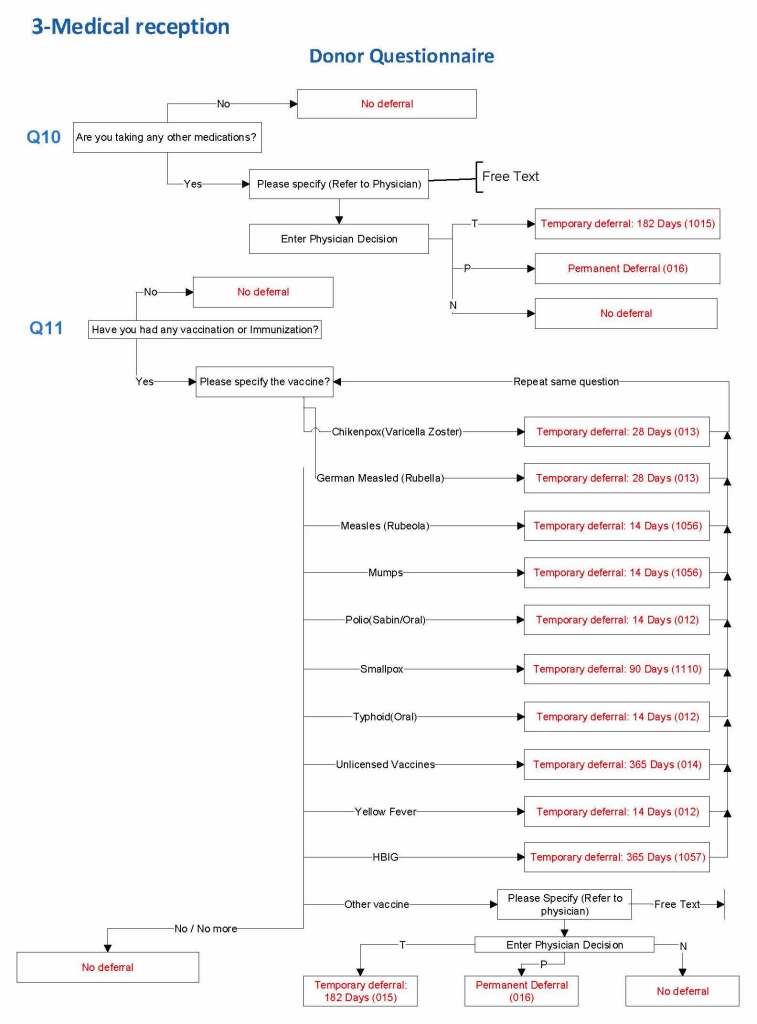
Some questions were more open-ended, and the interviewer manually entered a medication, surgical procedure, etc. The transfusion physician would review this and assign a temporary (specifying the interval) or permanent deferral.
The questionnaire was constantly being updated by changes. My role was to review different accreditation systems (AABB, CE, etc.) and the World Health Organization’s websites. I would then prepare an interim policy and pass the specifications for the changes to the Medinfo software engineer and when ready, finally to the Super Users for testing. If there was an urgent change, the whole process could be completed in less than one day including validation testing.
The following shows examples of the software processes:
Medications
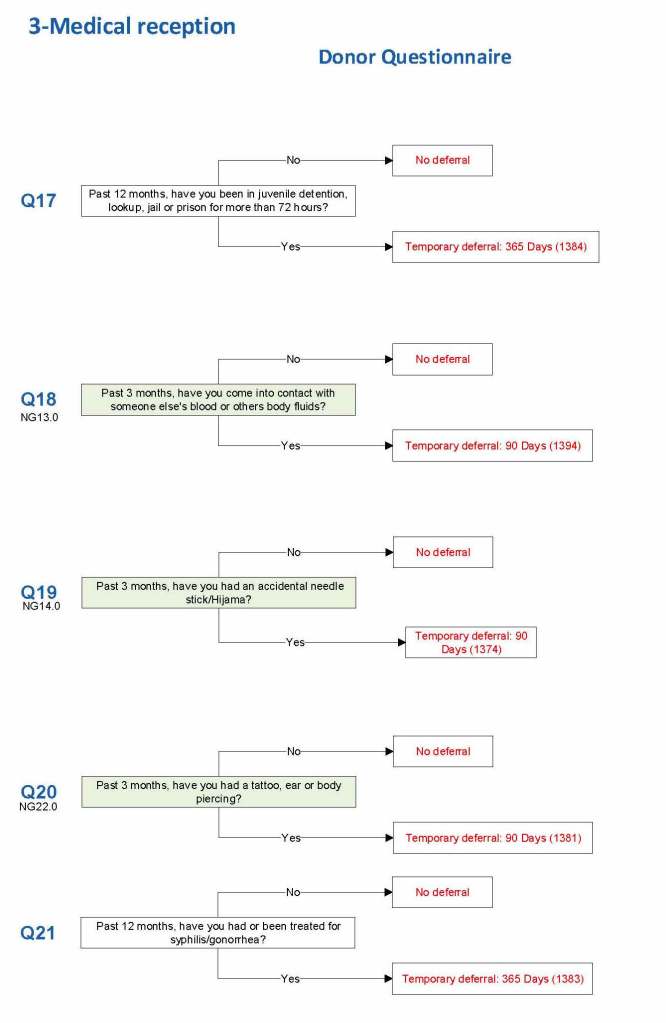
Body fluid exposures
Vaccinations
Malaria
Ebola/Zika
I emphasize that all of these settings are user-definable (at least in jurisdictions that permit all open, non-turnkey software).
Medication Questions:
Vaccinations:
Blood and Body Fluid Exposures:
Malaria Example: DMAL refers to the malaria antibody test.
Building the Software Processes for the Donor Collection 5:Donor Physical Examination and Adverse Reaction Reporting
Donor Physical Examination and Adverse Reactions
Donor physical examination, along with the donor questionnaire, are important both for donor and patient safety. In general:
Is it safe for the donor to donate?
Is it safe for the patient to receive the blood even if it is safe for the donor to donate.
Any donor who does not feel well must not donate. This may be the single most important step in ensuring a safe blood supply.
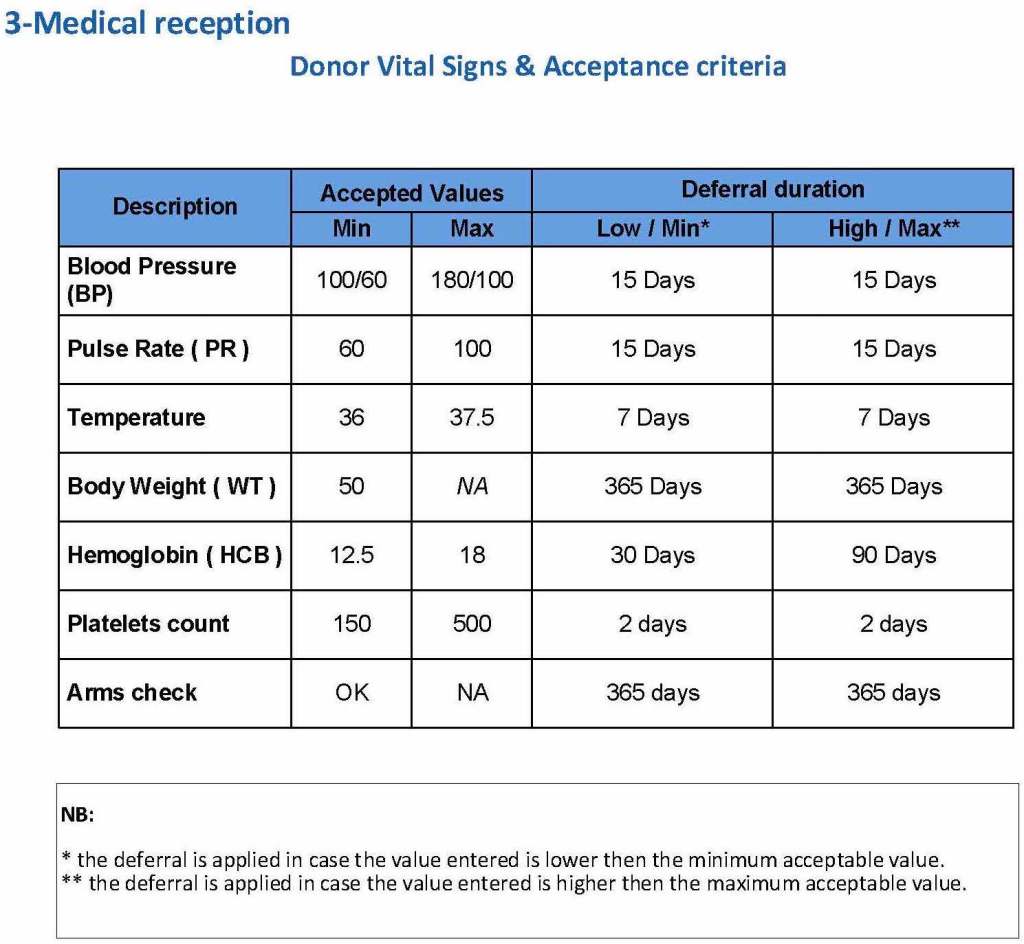
The donor physical examination includes the vital signs (blood pressure, pulse, temperature, heart rate, and temperature). I have attached a sample set of criteria for review. All are user-definable. Note how the arm examination is also included (looking for scarring, skin lesions, etc.)
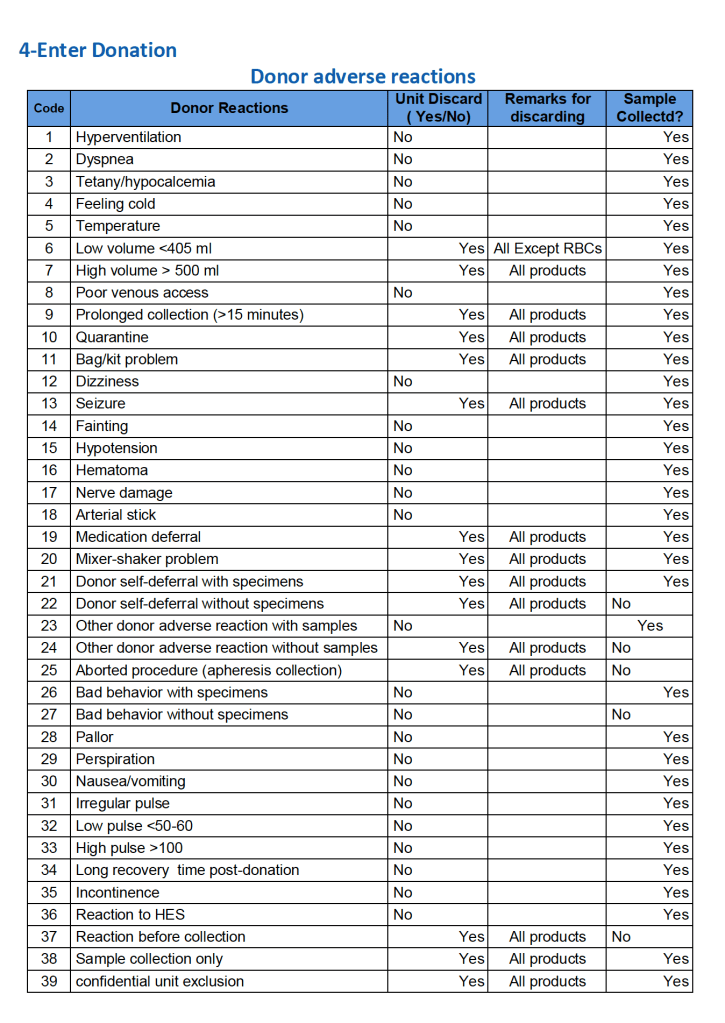
For all types of donations, there may be adverse reactions. These must be documented in the record along with the disposition of the donation. Will the donor need an extended deferral if the RBCs in the apheresis run are not returned? This can be built from the reaction documentation. Note the following sample table of reactions.
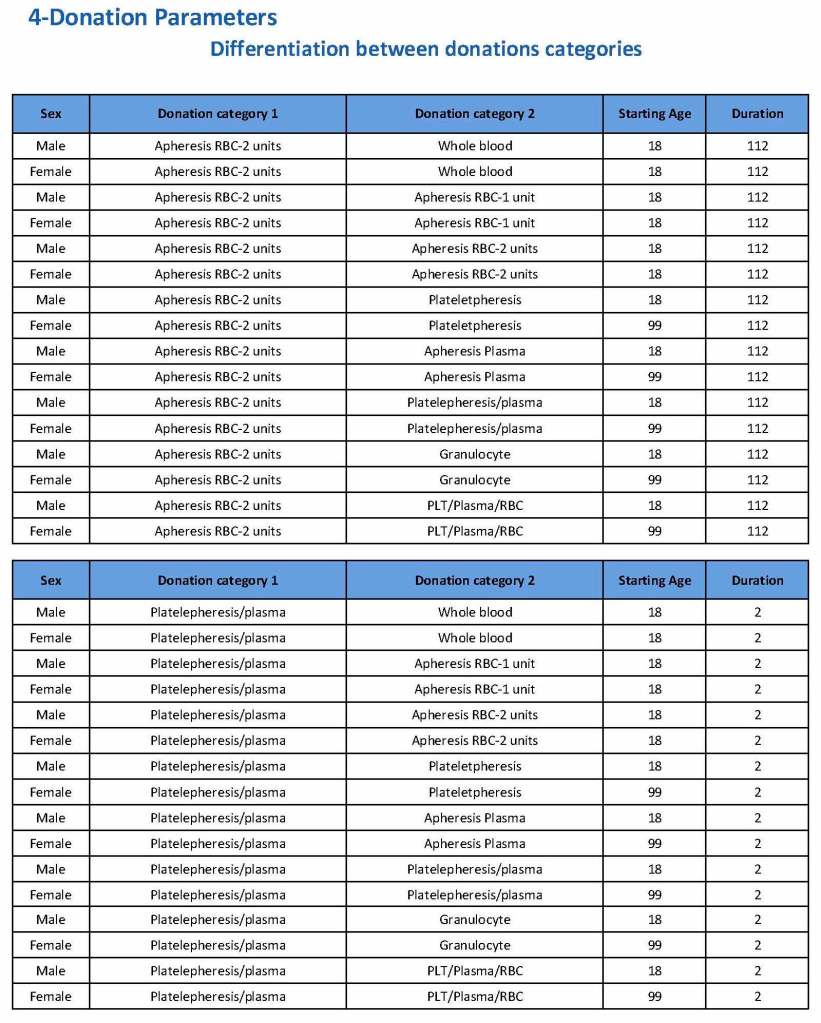
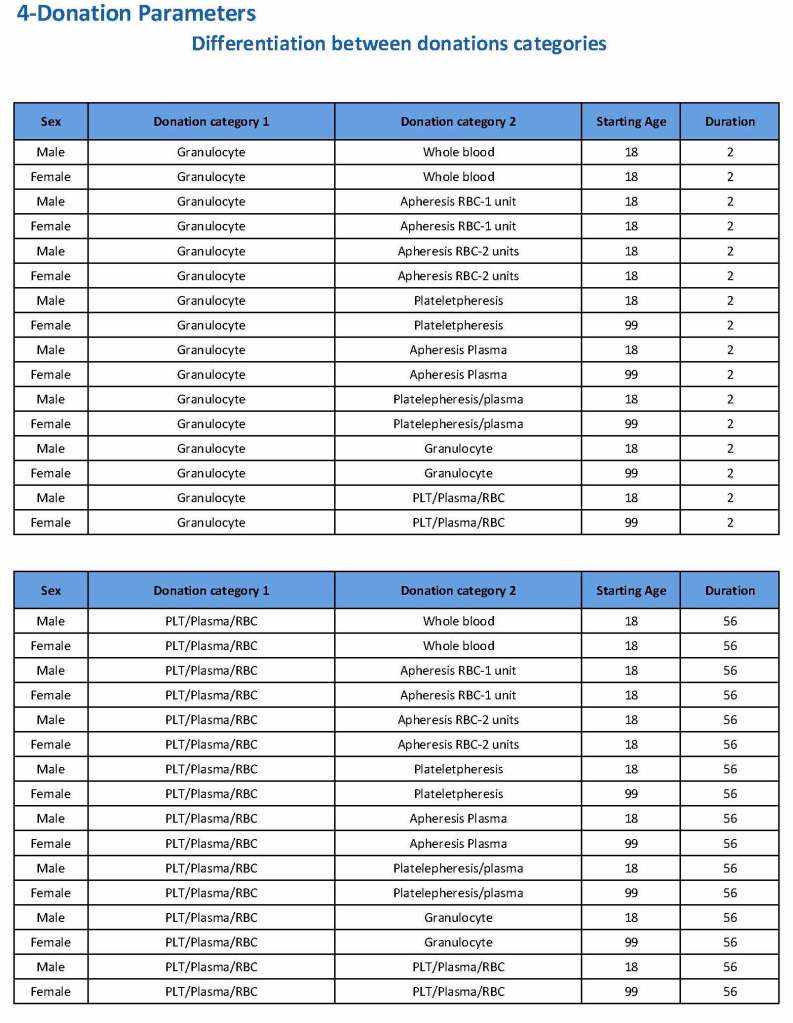
Donation can be whole blood or apheresis-based. The sex and age for each donation type is specified. At HMC, we did not accept females for platelet or plasma donations, so the starting age is listed as 99 years. Otherwise, in accordance with Qatari law, the starting age for donation is 18. All these parameters are user-definable, and a transfusion medicine physician can override the rules if necessary.
For each and every combination of donations, the deferral interval must be specified. Examples follow. The temporary deferral period is in days:
Previous donation whole blood, current donation whole blood: 56
Previous donor platelets, current donation whole blood: 2
Previous donation whole blood, current donation platelets: 56
Also note how for each possible combination there is an entry for male AND female. Females are restricted to whole blood donation and only RBCs will be made from the collection.
If there is a collection incident and the apheresis procedure is not completed, the interval will be set to 56 days. This will be covered in the post on donor adverse effect reporting.
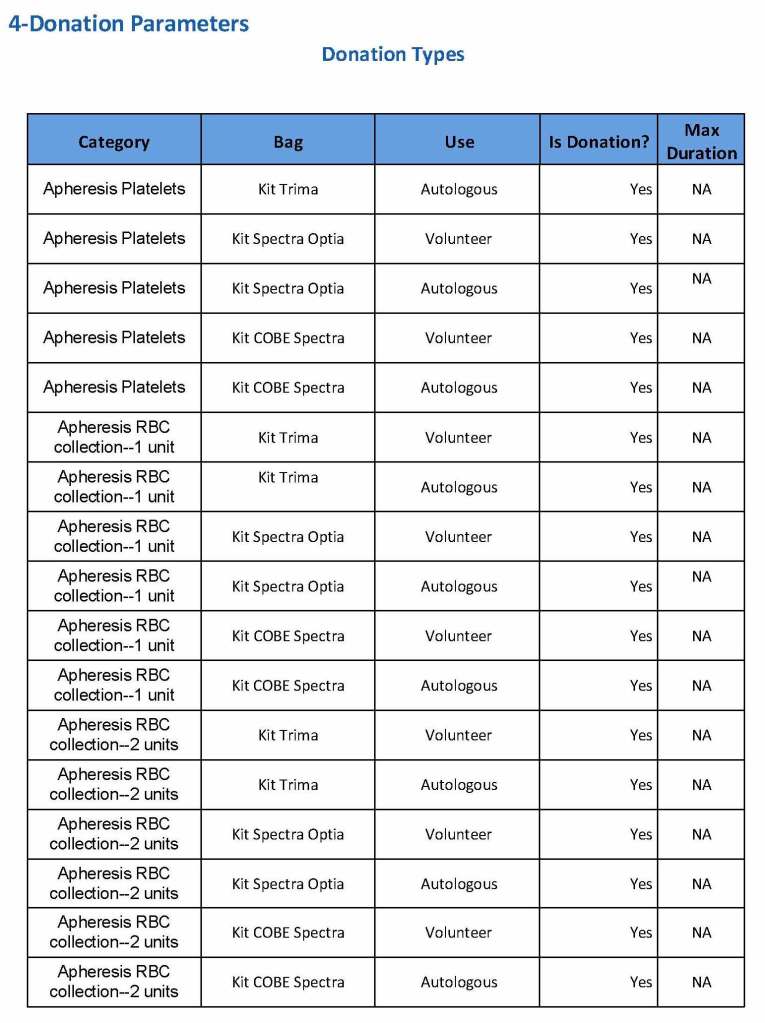
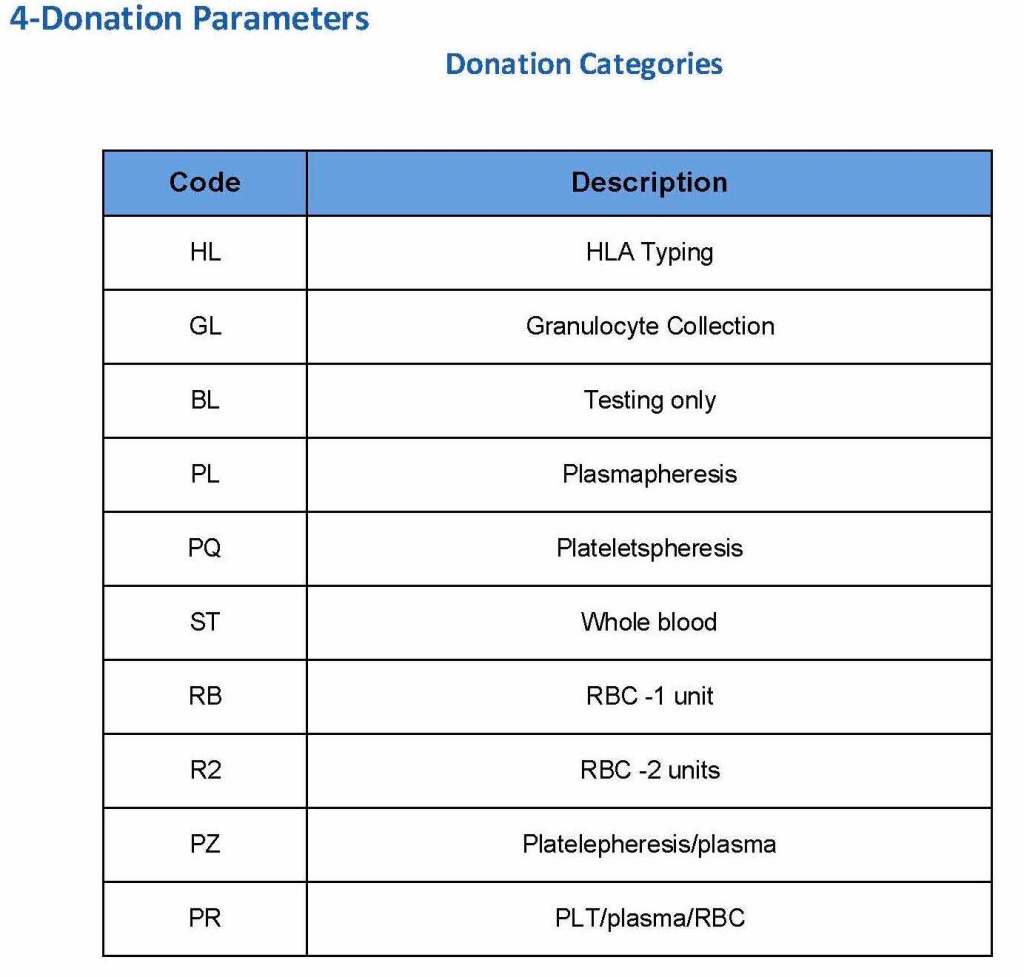
At the time of registration, the type of donation must be specified. In my last position, this could include whole blood for automated Reveos, whole blood for cryoprecipitate, plasmapheresis, COVID 19 convalescent plasmapheresis, plateletpheresis, concurrent platelet and plasmapheresis, concurrent platelet, plasma, and RBC apheresis, RBC apheresis-one unit, and RBC apheresis-2 units.
There is also a specimen-only donation without actual collection that includes database check, assignment of an ISBT specimen number, donor questionnaire, physical examination, and specimen collection only..
We specified which bag or kit could be used for each type of donation so when it was selected, only that bag type would be accepted by Medinfo
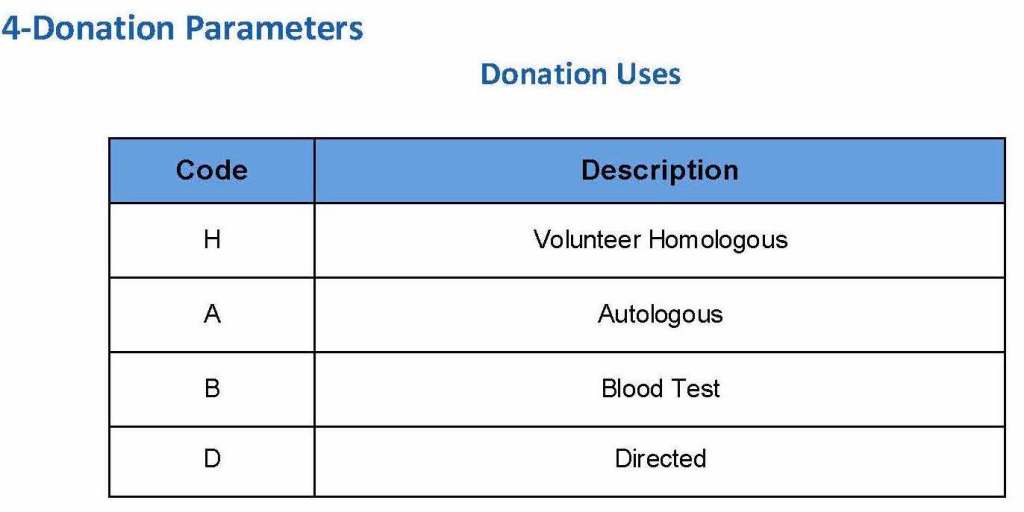
For each of these types we must specify what type of donation is permitted: volunteer, autologous, or directed.
Finally, we must indicate the maximum length of the procedure permitted. This applied to whole blood only and we set this at 15 minutes—this is user definable.
The following are a sample set of parameter settings for the above:
Note how we included contingencies for old bag sets and equipment (that we later discontinued) and for granulocyte collection (which we did not actually perform).
Building the Software Processes for the Donor Center 2:
Donor Collection and Screening—Registration and Pre-Donation Parameters
The potential donor enters the collection area. He takes a number and waits to be called. When called, he shows a picture identification card with a unique alphanumeric sequence. This is entered into the donor module software and the system checks the donor deferral database for temporary and/or permanent contraindications. If none are found, a consent form with an ISBT specimen number is generated.
In this post, we will consider:
Registration process in multiple languages
Donor deferral database
Donor consent with generated unique ISBT specimen number
Registration Parameters
Registration:
In the Middle Eastern region, multiple languages are used. Although Arabic may be the main language, not all the registration staff may speak it. English is commonly used as the main work language. The date may be entered as Common Era (Gregorian) and/or Hijri.
An issue is that for native Arabs, the only precise, unambiguous name spelling is in Arabic. English transliterations vary. Example, Muhammad in Arabic is very simple to write, in English it may be rendered as Mohamed, Mohammed, Muhammad, etc. The donor’s name should be recorded exactly as in his native alphabet. How do you register when the staff do not speak or type Arabic?
Fortunately, I have worked with software that is in UNICODE, meaning that the data does not have to be restricted to English or Latin script (I wonder why the hospital information system we had at one institution could be sold in the Middle East and not have this capability!). That means one could perform registration and donor questionnaire tasks in multiple languages, and preferable the native language of the donor. One could even prepare database reports in Arabic.
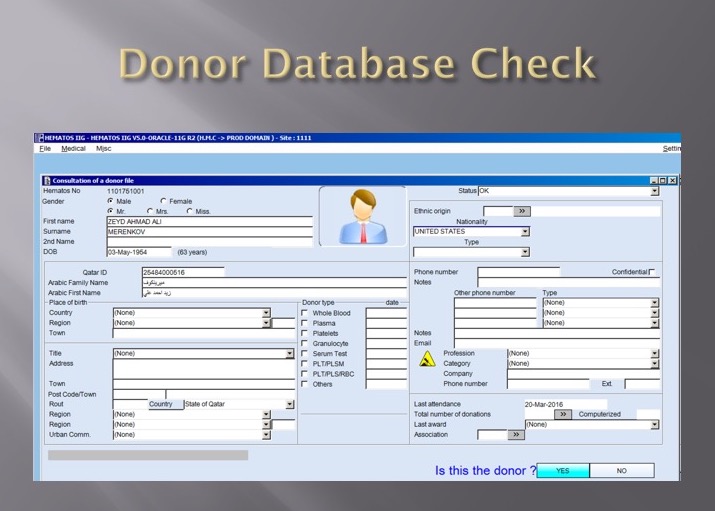
Medinfo had an elegant solution to the registration process in Qatar. It read the local identity card’s barcode issued by the Ministry of Interior and accessed (read-only) the demographic data on that donor and received back both the English and Arabic name fields:
This would generate the demographic fields in the registration:
The blood bank software would check the national donor deferral database and list any deferrals/contraindications to donation and the next eligibility date. It would also list what type of donations were permitted (e.g. for females, only RBCs could be collected and processed: if a whole blood unit was collected, then the platelets and plasma would NOT be permitted to be processed and were discarded.)
Medinfo used a unique key field, the Medinfo Hematos Donor ID for the database. This was not the same as the national ID card. All records were indexed against this number with strong security.
Donor Deferral Database:
Medinfo had already imported donor data from a previous computer system and added this to its own database. Thus, there was only one database to check. The database listed all previous donations: dates, type, status (complete, aborted). Any contraindications would be prominently shown in RED.
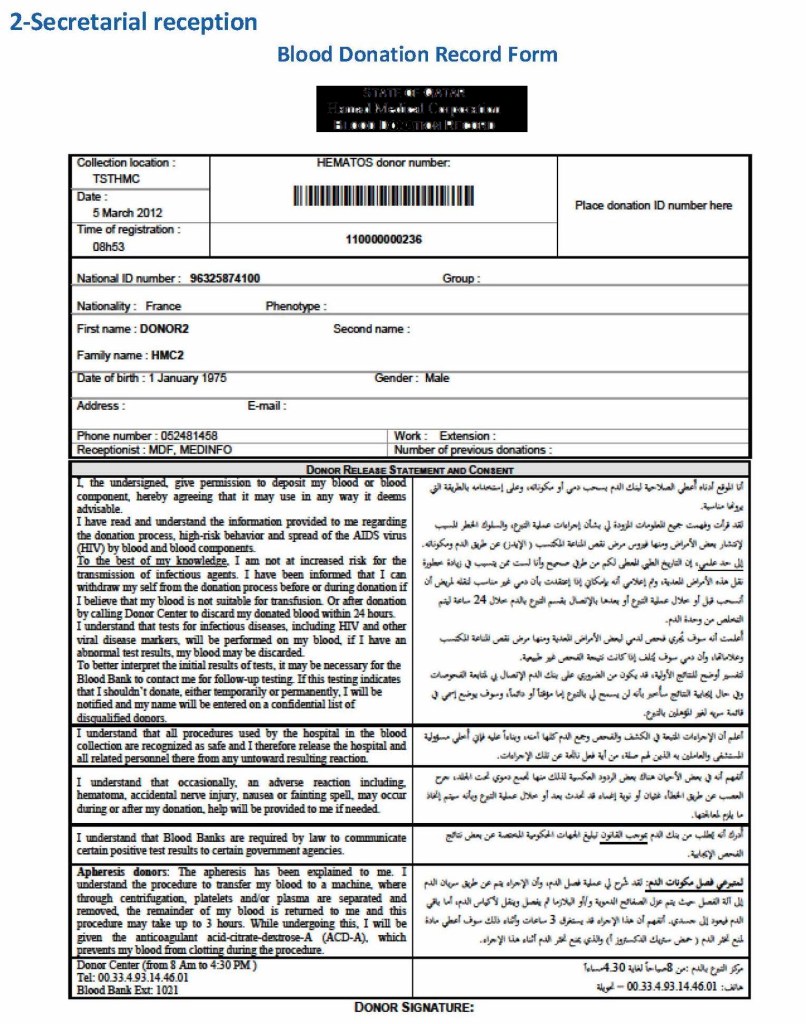
Donor Consent and Assignment of Donor Unit (ISBT Specimen) Number:
If there were no contraindications, Medinfo generated a donor consent in English and Arabic and the unique donor unit number for the current encounter:
Registration Parameters:
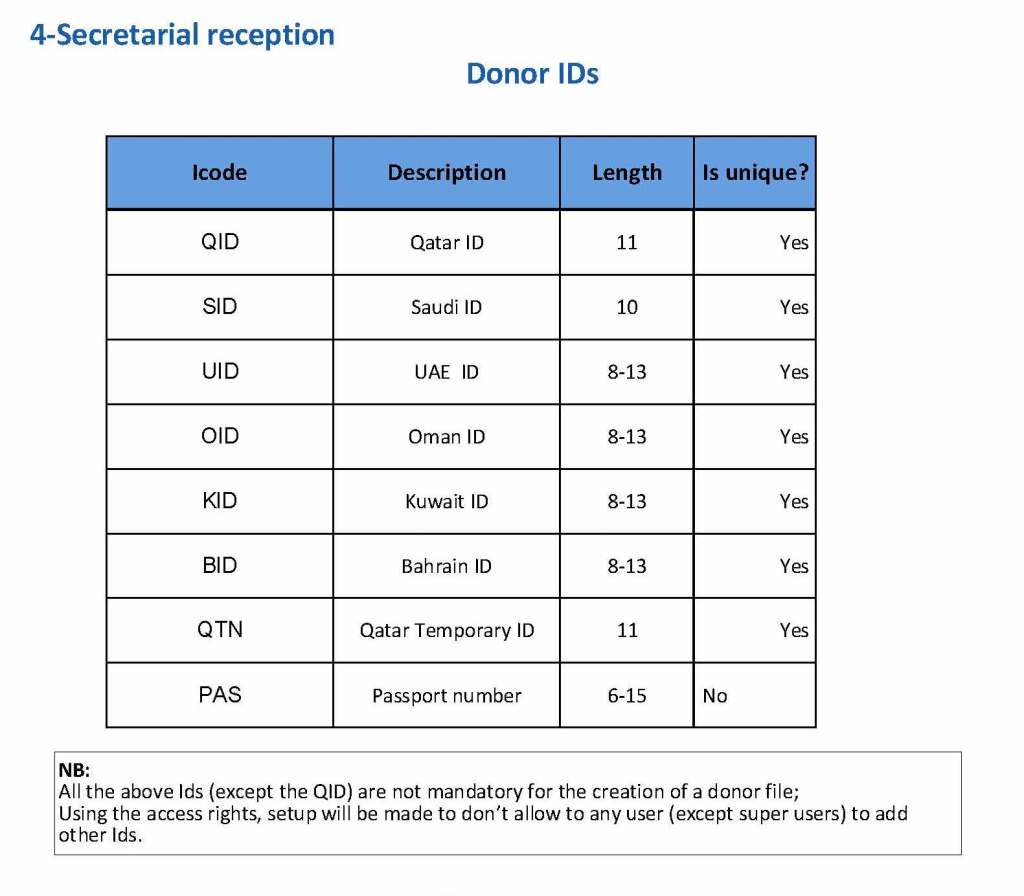
Medinfo enforced registration according to the format of the identity card. The donor ID format was built into Medinfo. If the entry deviated from this, it was rejected and registration could not continue:
The registration type would be selected (volunteer, autologous, directed, or paid). In Qatar, paid donations were not permitted:
Next, the donation type had to be selected:
At the time of registration, the type of collection bag (or kit if using Reveos) was automatically set in Medinfo. I will consider this further in the next post of this series to determine eligibility based on the previous donation interval and type.
At each donation site, the allowable types of donations and kits could be set. Based on the donation parameters above, staff could not select the wrong type of bag/kit (e.g. an apheresis kit for a mobile donation).