Principle:
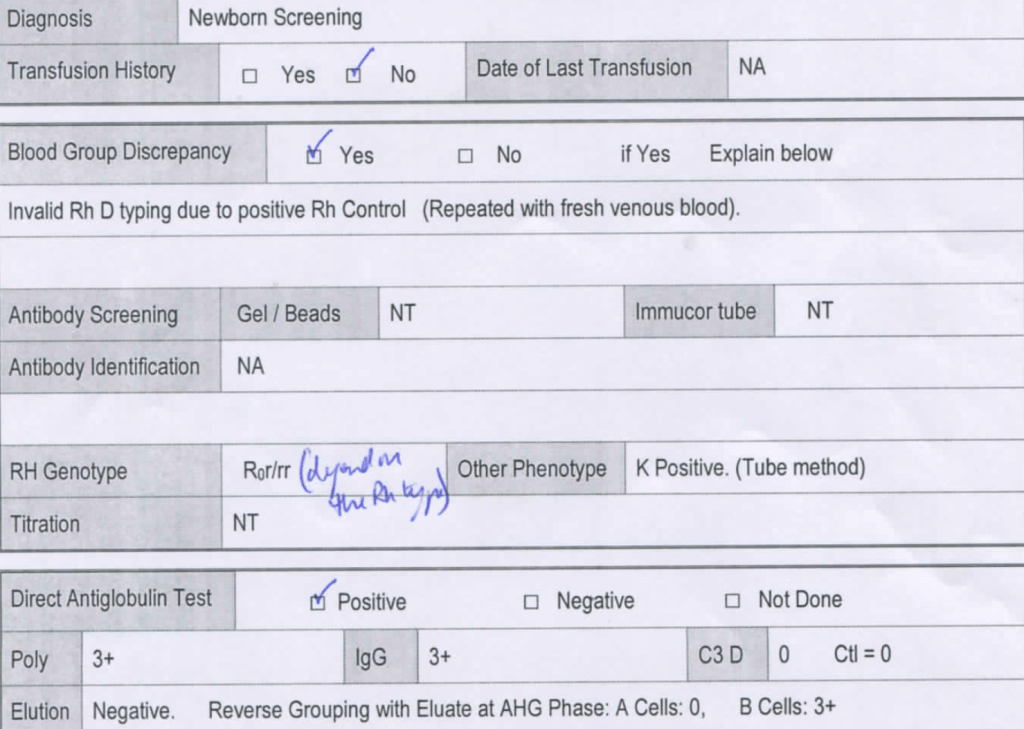
Daratumumab is a monoclonal antibody that binds to CD38 antigen, which is expressed weakly on the surface of all RBCs. It may thus cause a positive direct antiglobulin test DAT and so interfere with compatibility testing if an antiglobulin phase is required.
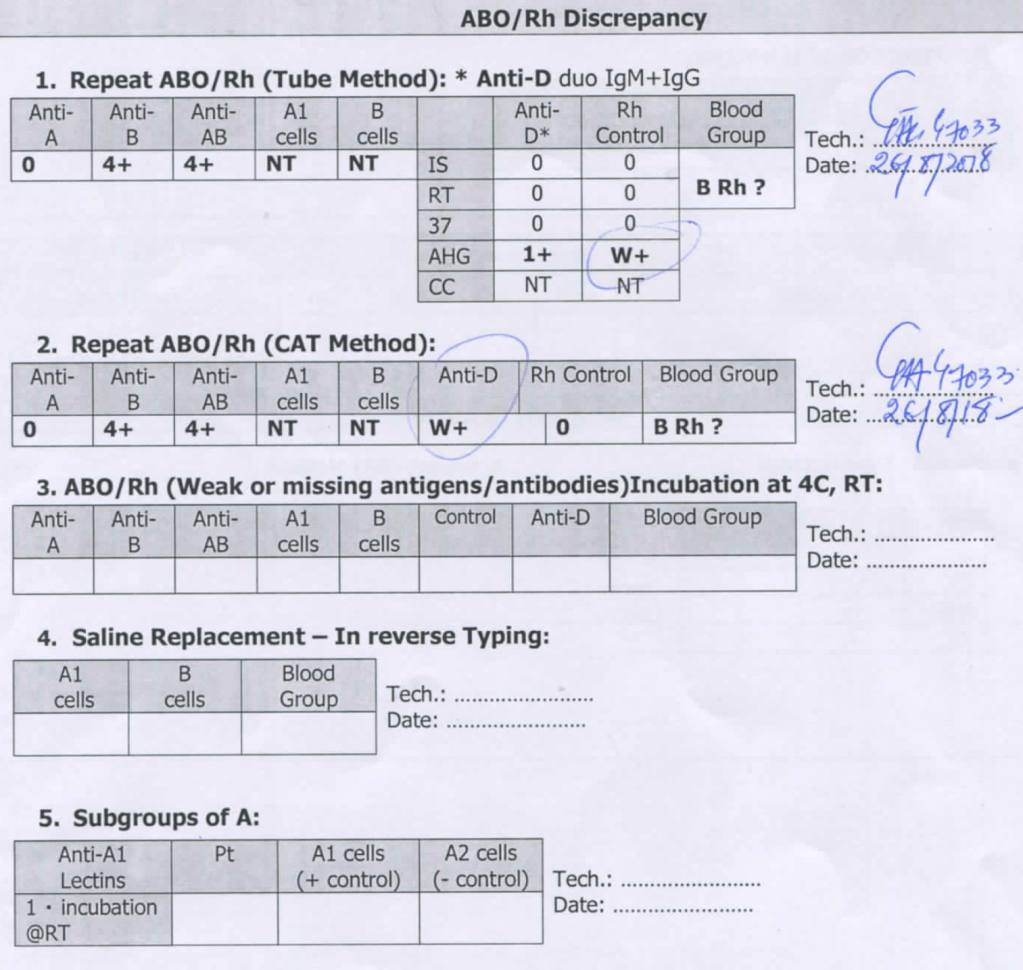
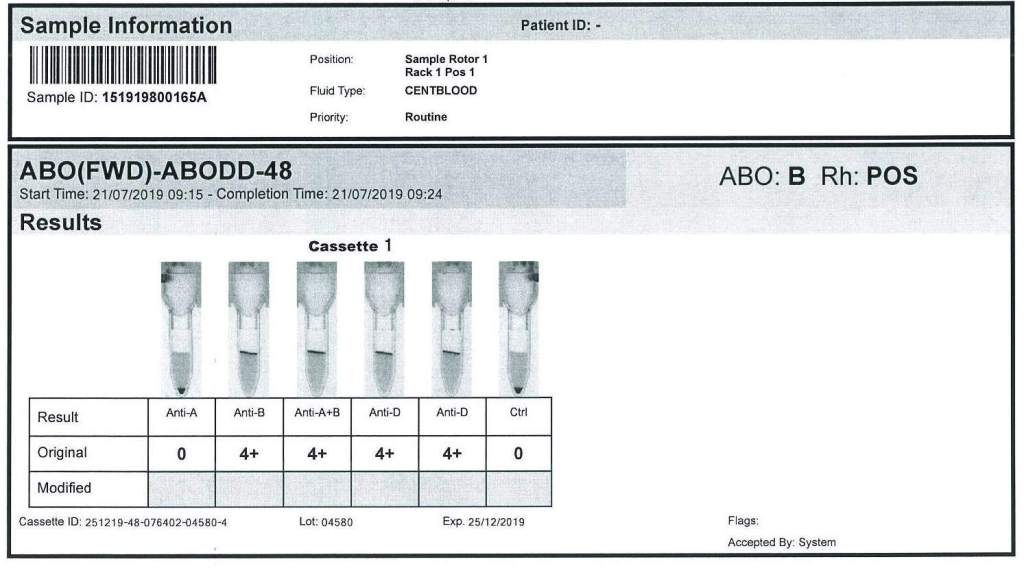
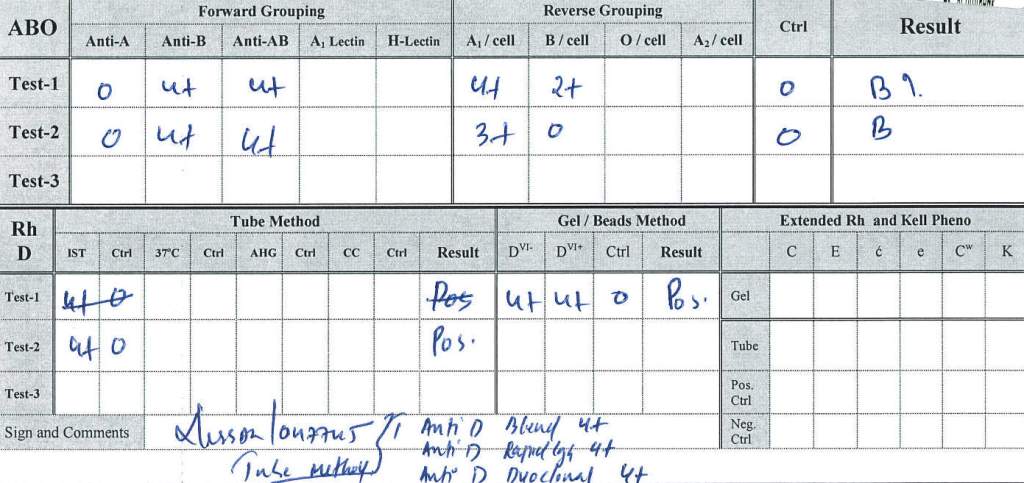
This effect may persist up to 6 months after discontinuing the drug. The monoclonal antibody does not interfere with routine ABO/D typing.
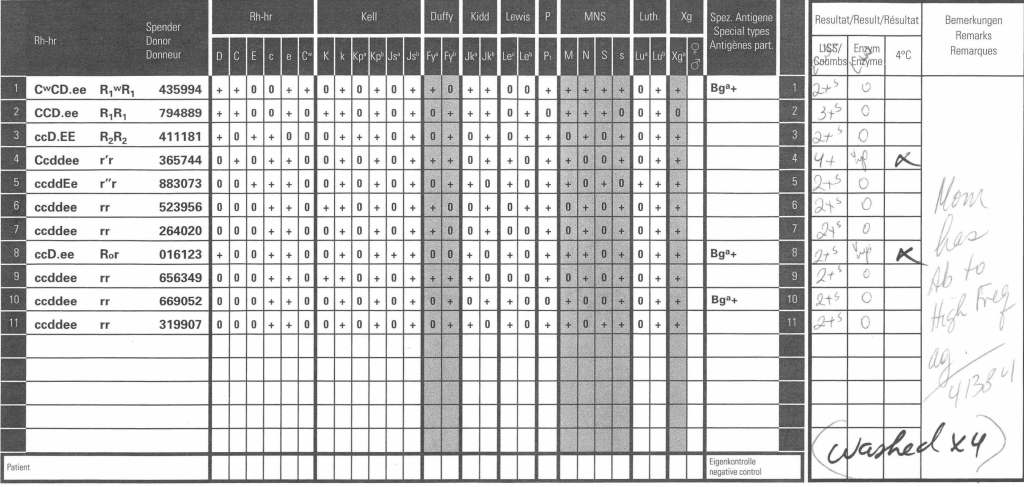
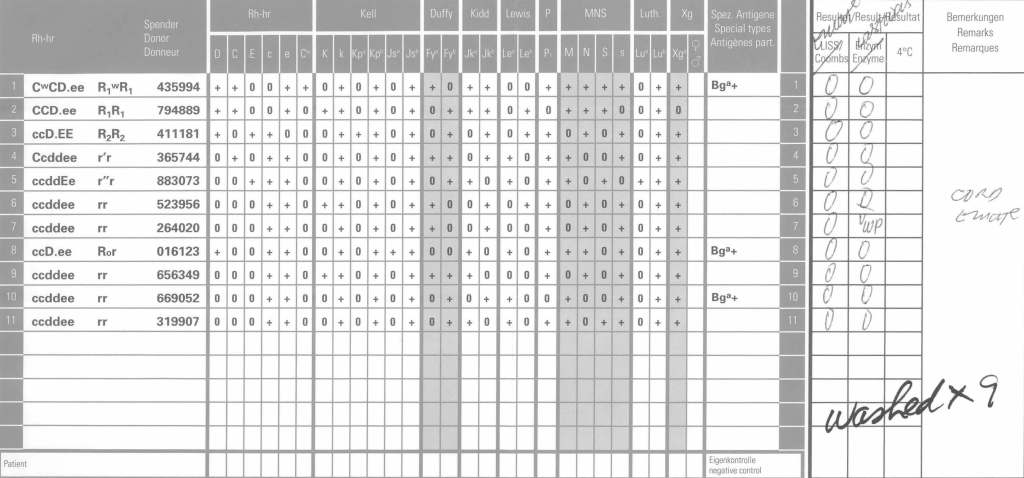
Special techniques (neutralization of CD38 antibodies by CD38 anti-idiotypic antibodies, or soluble CD38 antigen) may remove the panreactivity but are not generally available. DTT, a sulfhydryl reagent may denature the native CD38 antigen on RBCs but it should be used under a biologic hood.
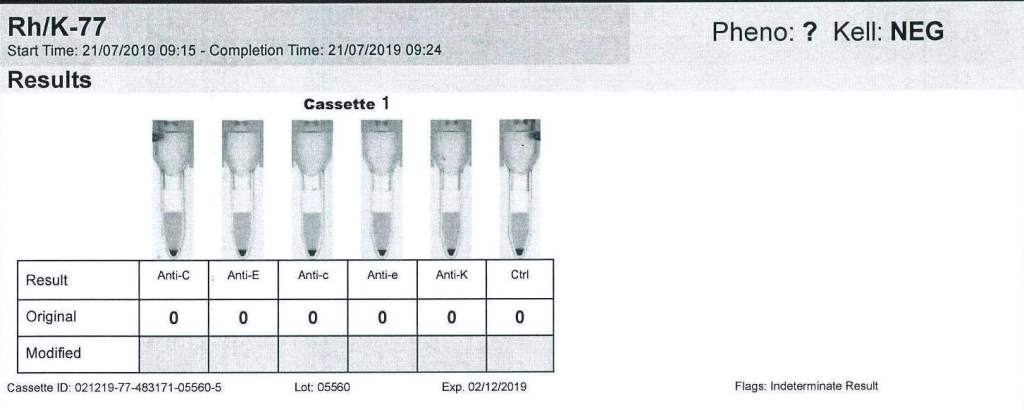
Kell antigens will be denatured so Kell antibodies cannot be detected after treatment so Kell-negative RBCs should be used. In the Gulf Area, this is about 72% of RBCs. In the Medinfo software a rule to require K-negative RBCs has been built.
Policy:
- The clinical services must inform Transfusion Medicine of patients who will be receiving daratumumab therapy BEFORE treatment is started.
- Transfusion Medicine staff will enter a general comment (i.e. not associated with a particular result) in the patients Medinfo HIIG record: PATIENT ON DARATUMUMAB.
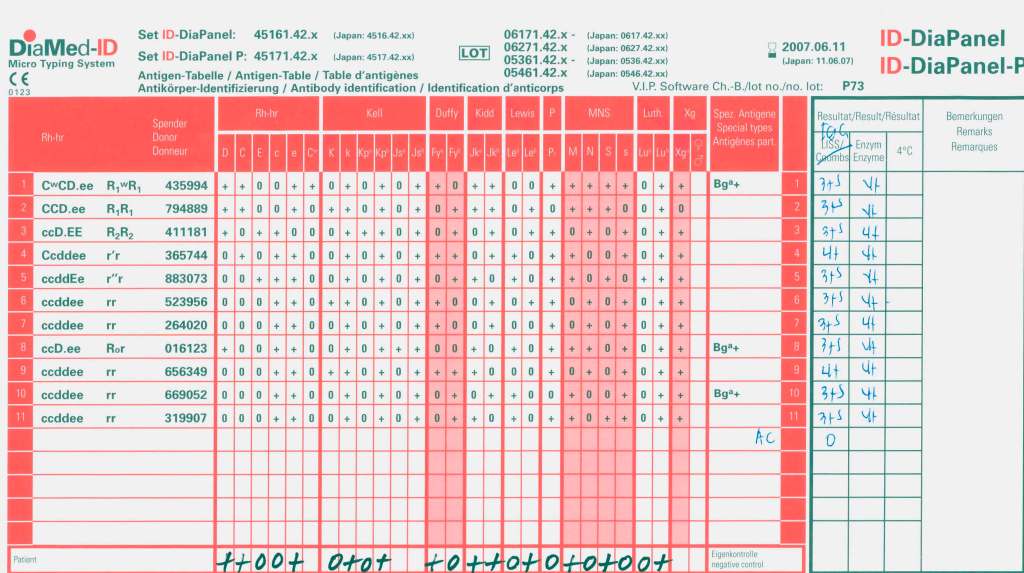
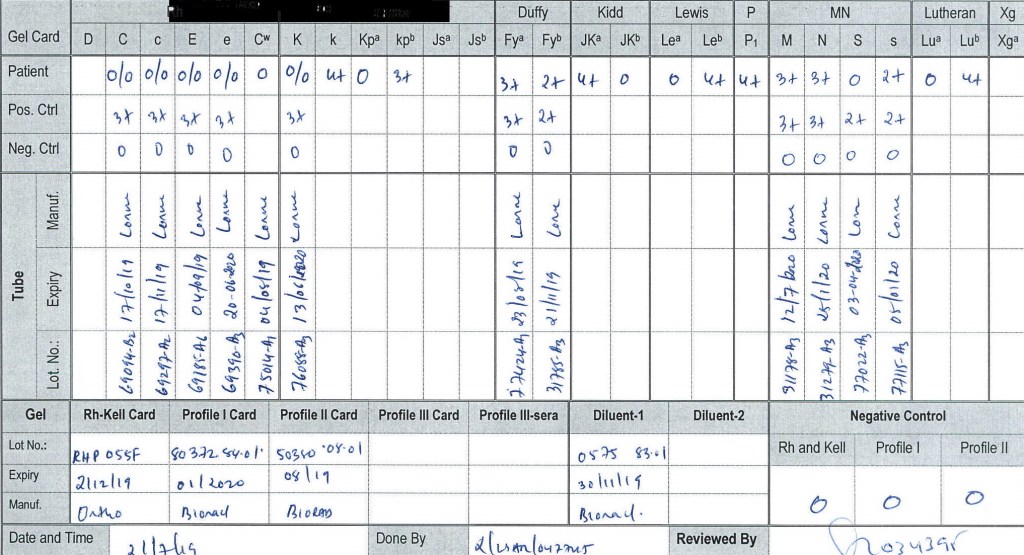
- If not already done, Transfusion Medicine staff will perform an extended antigen typing: at least C, c, E, e, K, k, Kpa, Jka, Jkb, Fya, Fyb ,M, N, S, s, Lea, Leb, P1—even if no antibodies are currently identified.
- Transfusion Medicine staff will send each such patient’s record to a Transfusion Medicine Physician to determine the blood type including extended antigens to match for future transfusions.
- When compatibility testing is requested, perform it as per our SOPs.
- If available, prepare DTT-treated cells for testing but realize that this will denature Kell antigens. Use K-nell RBCs.
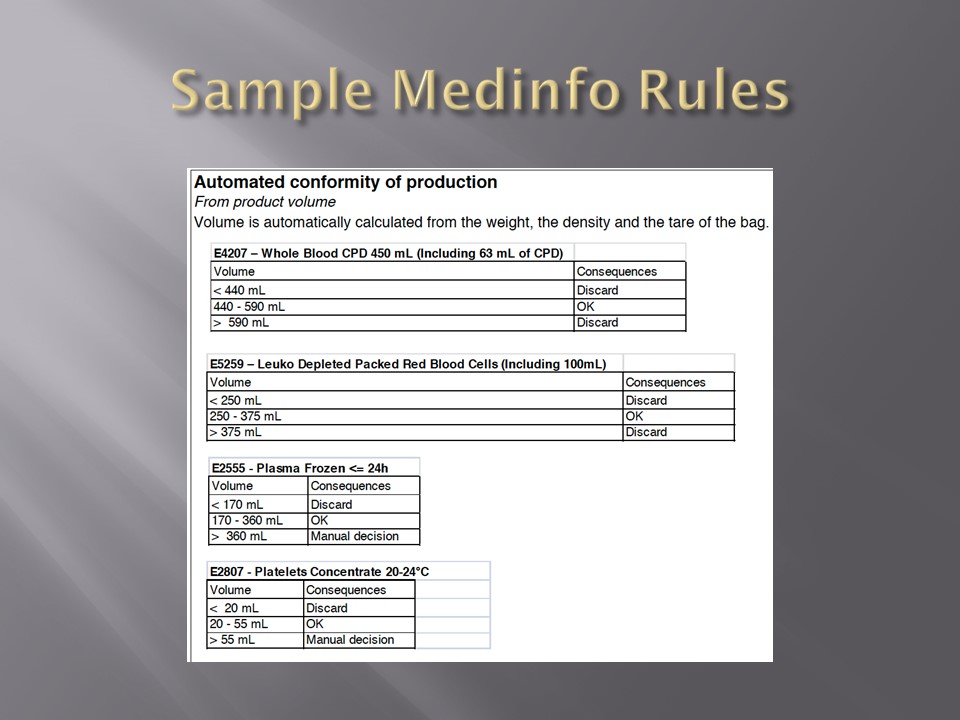
- Medinfo has a rule to automatically require K-negative RBCs if this medication is used.
- Release least “incompatible” RBCs must be approved by the Transfusion Medicine Physician.
- When the DAT becomes negative (i.e. up to SIX months after cessation of Daratumumab therapy), routine compatibility testing and RBC selection will apply.
References:
Trick or Treatment, Anti-CD38 Reactivity and How to Treat It, AABB Satellite Symposium transcript, U. Cincinnati and RedMedEd, October, 2015 (attachment)