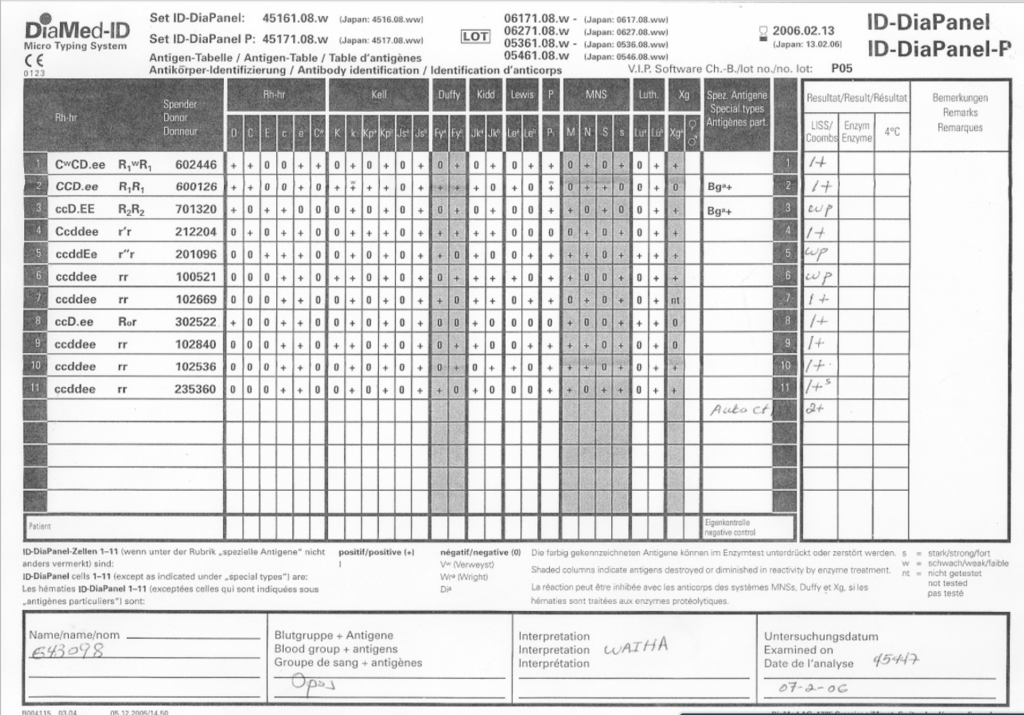
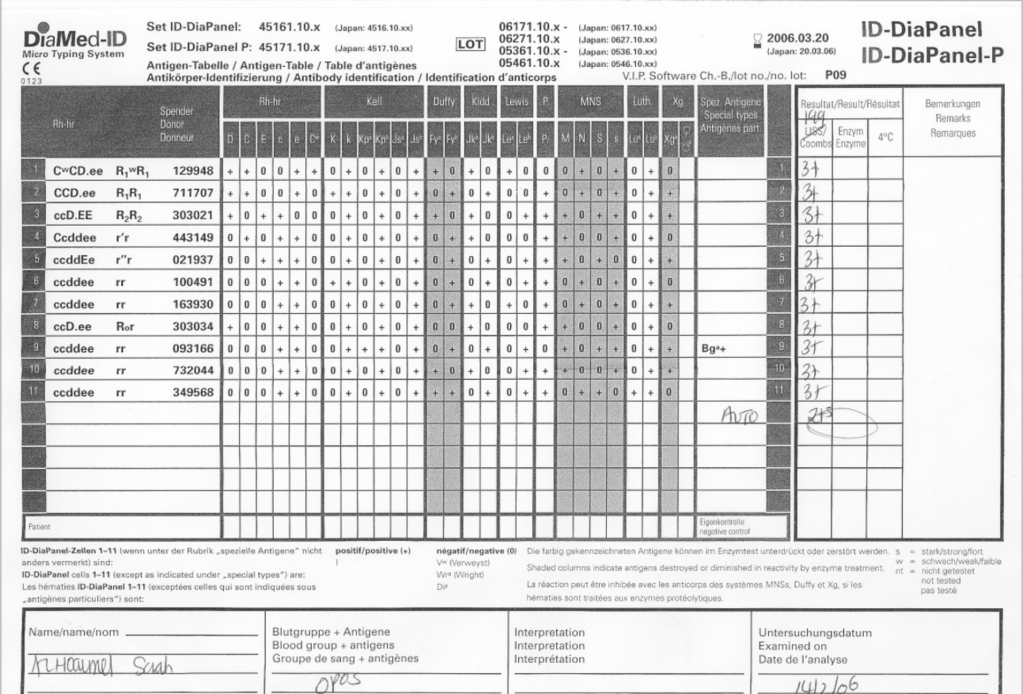
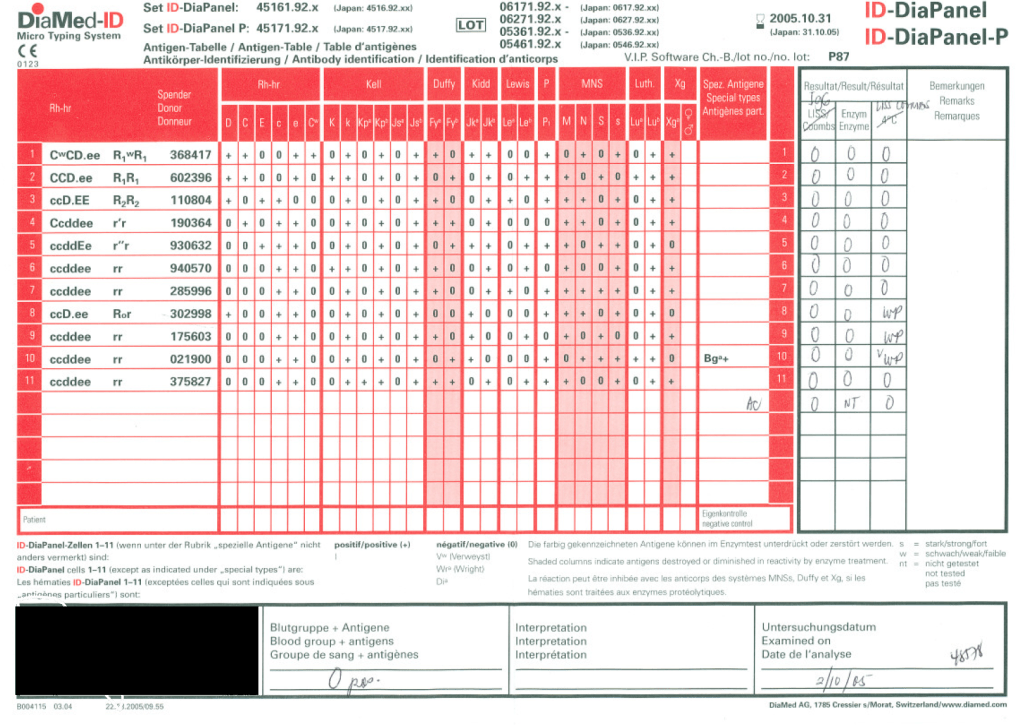
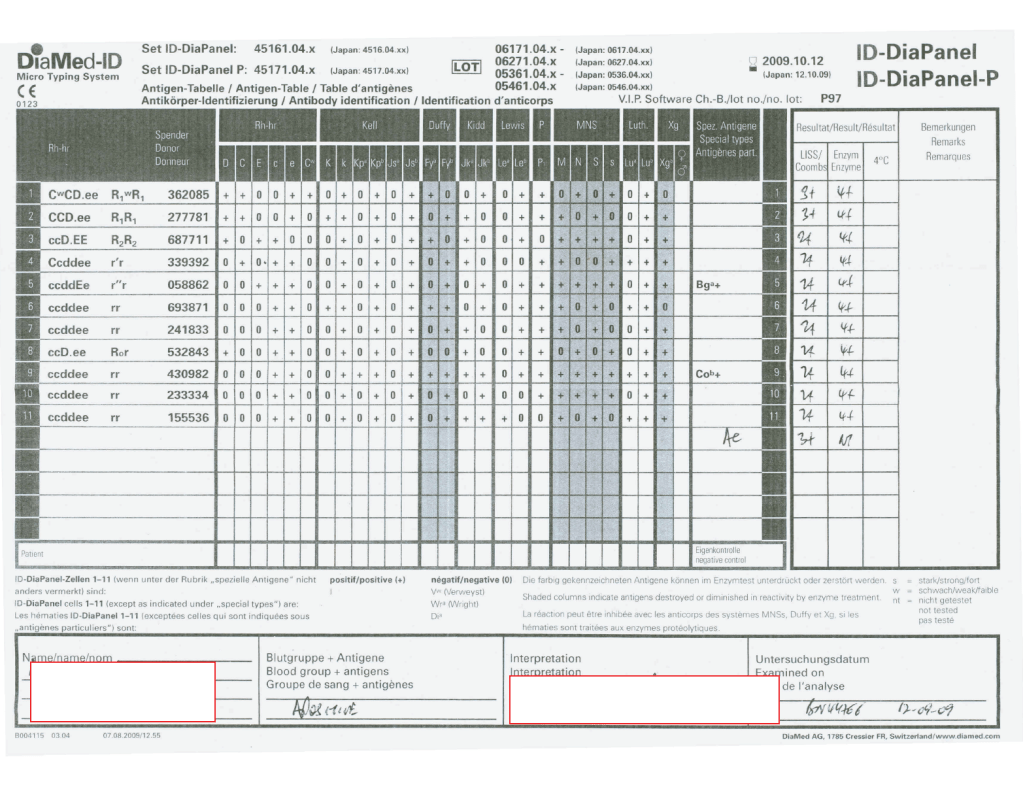
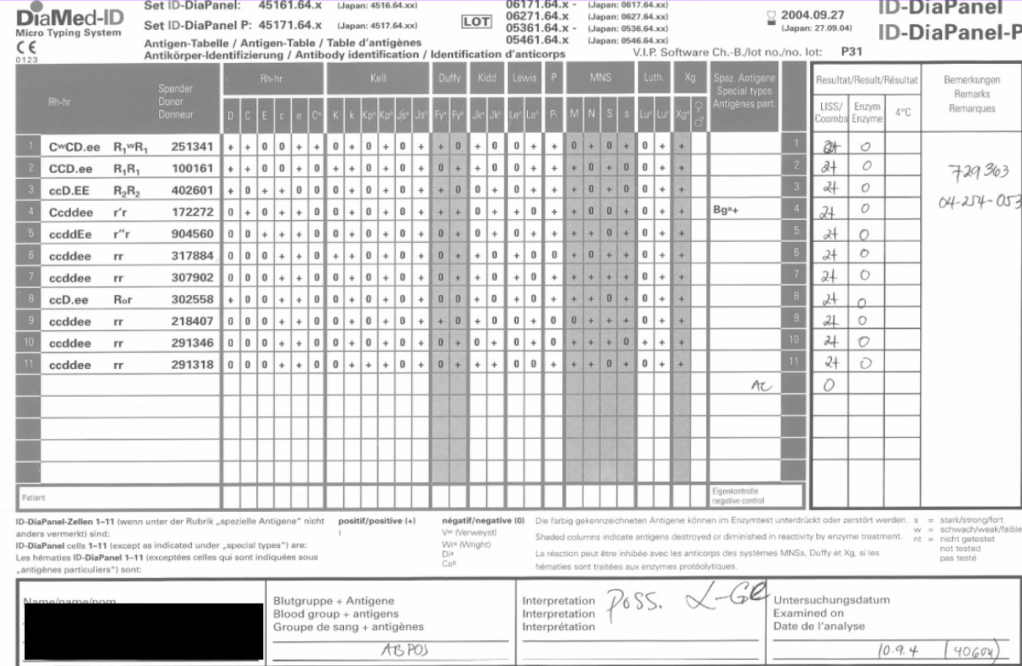
As a Transfusion Medicine physician, I reviewed all antibody workups. Here are three different panels, all appearing to be panreactive, at AHG phase. Note the differences:
- Autocontrol is positive, enzyme is panreactive and enhanced
- Autocontrol is negative, enzyme phase shows no reactions
- Autocontrol is negative, enzyme phase is panreactive enhanced
In the middle of the night, if I am called to select blood, I always keep these patterns first and foremost in my mind.
Case 1:
If the autocontrol is positive at about the same strength as the panreactivity. I can state that this is probably a warm autoimmune pattern WAIHA (although I cannot rule out underlying clinically significant alloantibodies obscured by this pattern and need to do autologous auto-absorption ZZAP). Both warm autoimmune antibodies and certain drug reactions may cause this pattern. Use least-incompatible crossmatch matching any significant specificities you found by ZZAP and observe the patient closely throughout transfusion.
Case 2:
If the autocontrol is negative and all reactions are enzyme-labile—and if you live in the Middle East/Gulf region, then you have a presumptive anti-Ge2. You can safely ignore this antibody and release least-incompatible crossmatch RBCs, regardless of the strength of the reactions.
Case 3:
If the autocontrol is negative and the reactions are unchanged or enhanced by enzyme, BE AFRAID, VERY AFRAID!! This is an antibody to a high-incidence antigen. These can be very dangerous. In the Middle East/Gulf region, consider anti-H, anti-k (cellano), anti-Kpb, anti-PP1Pk, and rare antibodies to the MNSs such as anti-U or other MN system deletions. There are many other possibilities, e.g. anti-Fy3.
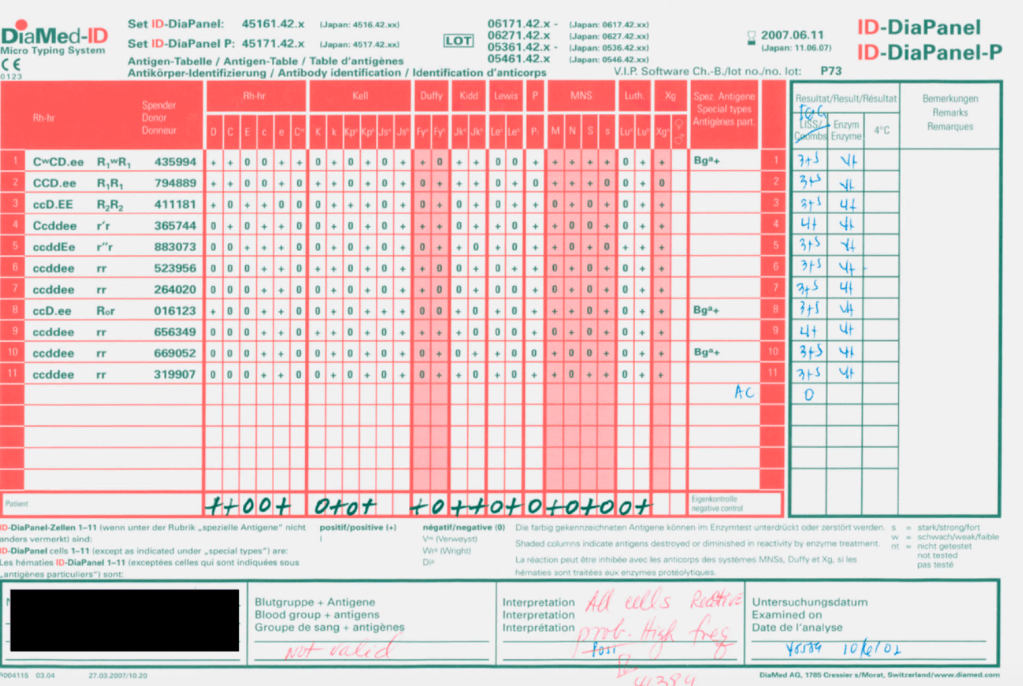
You need to perform extended antigen typing across the major Rh antigen, Kell, Duffy, Kidd, MNSs, P systems (at least P1):
- Run H lectin to rule out Bombay Oh or Parabombay.
- Some Rh system deletions and Rh null show pan-Rh reactivity—check D, C, c, E, e typings.
- Anti-k (cellano) will be suggested by k-negative phenotype.
- Unusual, weak or absent reactions with M and N reagents suggest something like En(a)-negative or similar.
- Absent P1 with no other findings, you must rule out anti-Tja (anti-PP1Pk).
I have seen all of these specificities during my time in the Middle East. All of these antibodies can be clinically significant and often life-threatening.
Conclusion: NEVER NEGLECT TO REVIEW THE AUTOCONTROL!!!