A 31 year old Indian female’s prenatal testing results follow:
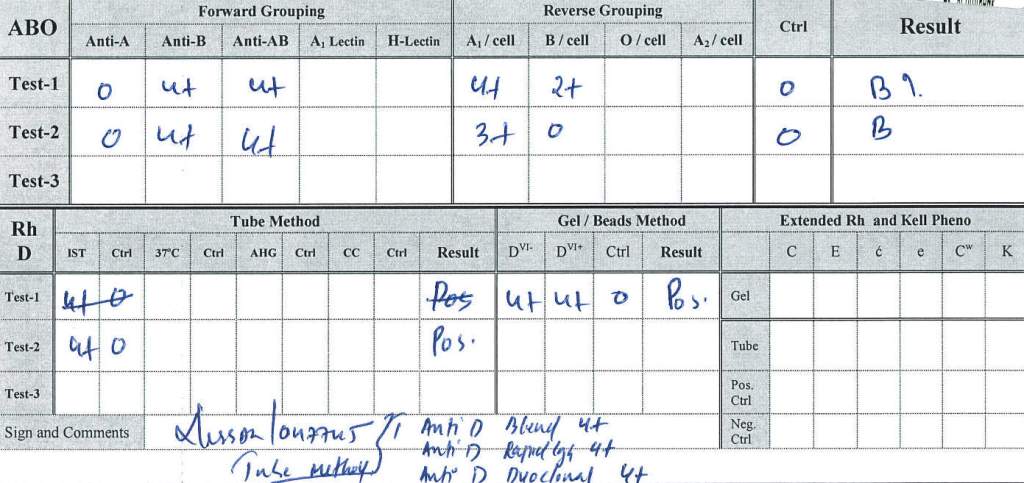
ABO Group B—unremarkable pattern
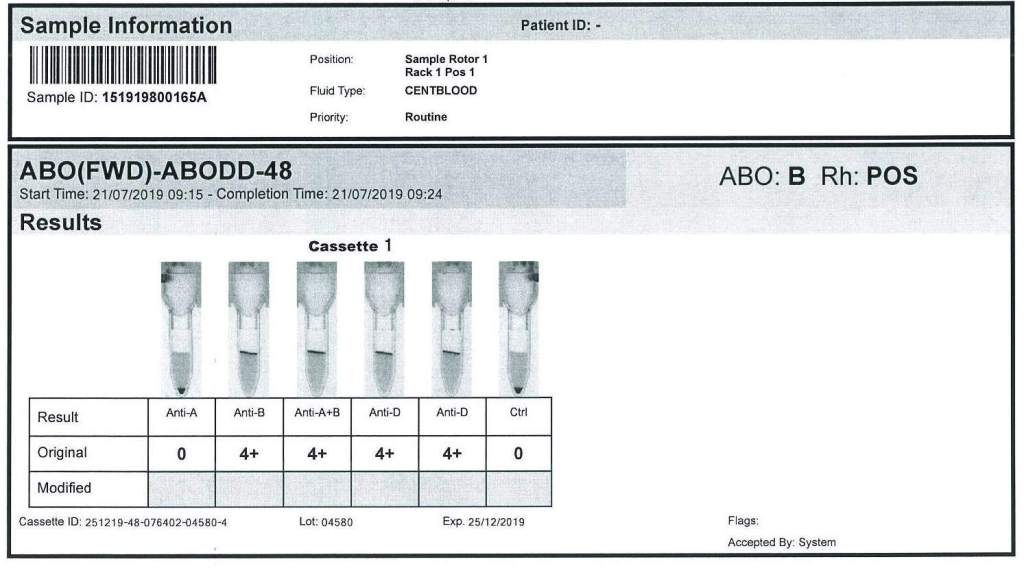
Rh(D) positive by both DVI+ and DVI- reagents by multiple manufacturers, both with gel and tube methods
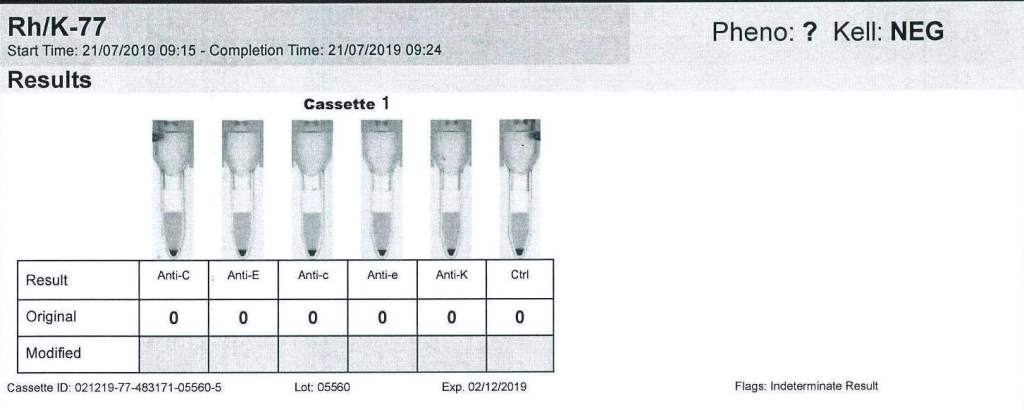
Extended Rh and Kell:
No reactions for C, c, E, e; Kell negative
(These results were confirmed by multiple manufacturer’s tube and gel reagents)
Extended Antigen Typings:
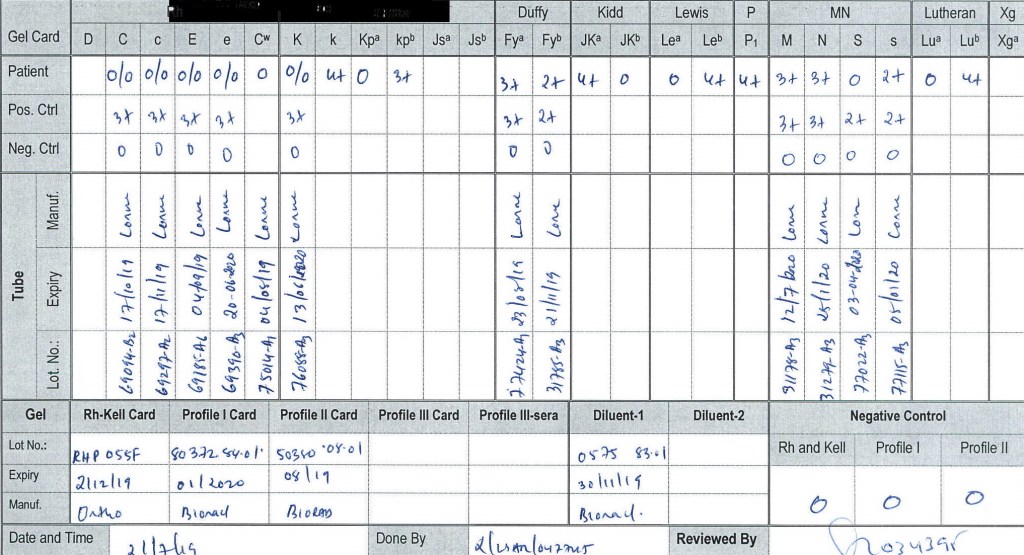
From the phenotypic data, we could already rule out anti-H, k, PP1Pk, U, and some unusual MN system variants found in the region.
DAT: Polyspecific and monospecific IgG, C3b/C3d were all negative.
Antibody Screen: 4+ panreactive
Antibody Panel: 4+ panreactive, autocontrol negative, also 4+ by enzyme
Clinical Course:
At the time of the prenatal specimen, we informed the clinicians that we did not know the significance of the panreactive antibody. We recommended screening any blood relatives and autologous blood collection. We also recommended genotyping of the mother.
Several months later the patient presented in labor with severe fetal hydrops. The previous workup was repeated and confirmed. Neither genotyping or autologous collection had been done. No relatives had the same phenotype, and none were compatible with the mother.
We now knew that the antibody was highly clinically significant and very dangerous. With the permission of the treating obstetrician, the mother’s blood was used for transfusion of the newborn (washed, irradiated). Both mother and baby were group B positive.
To date of my departure from HMC Doha, the antibody had not been characterized, but we continued to recommend genotyping and autologous collection from the mother.
