Includes compatibility testing (AHG, electronic, immediate-spin), antigen typing, antibody screening and identification, direct antiglobulin testing, elution, transfusion reaction and drug reaction workups, component typing tests upon receipt in hospital blood bank, release and return of components
This has been revised to recommend the use of a continuously recording portable vital signs device such as Umana’s UT1M (GPI, Italia) which includes PAO2 and heart rhythm measurements.
Principle:
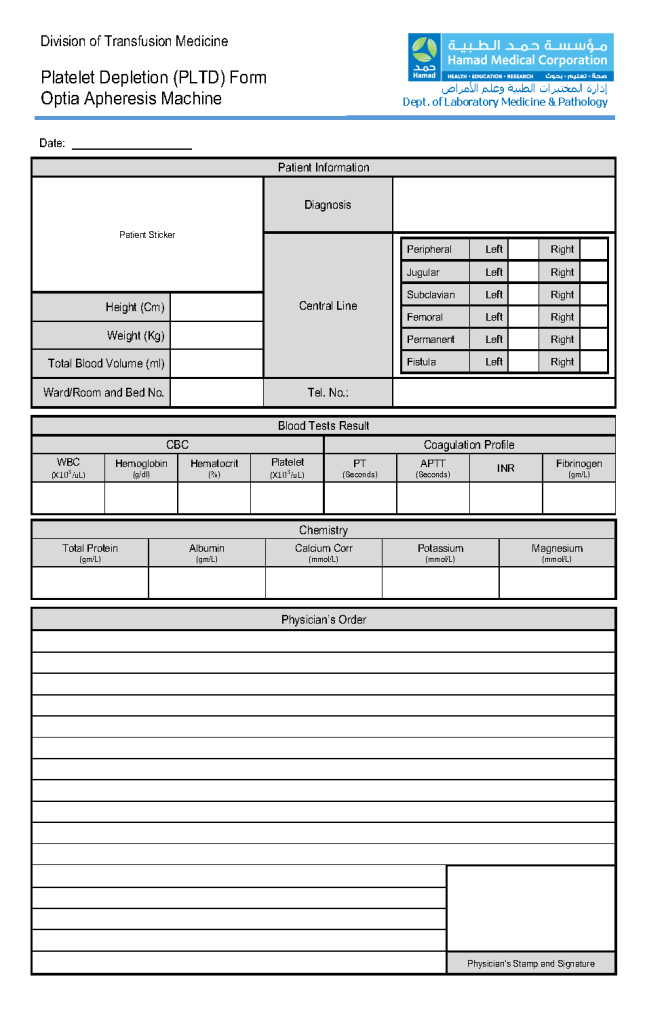
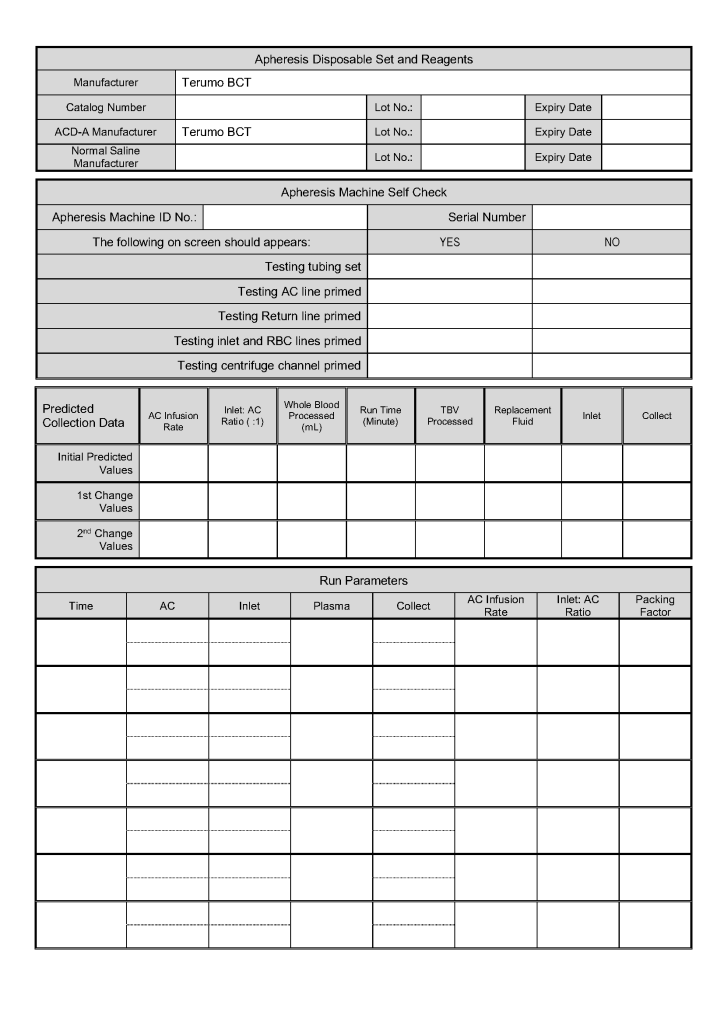
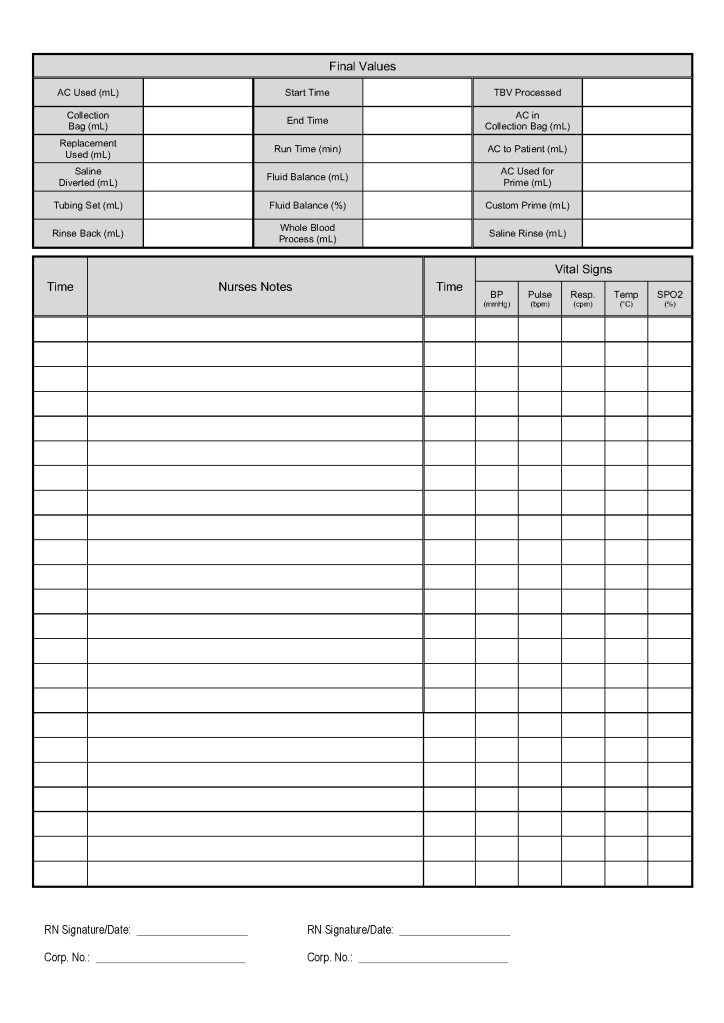
All therapeutic apheresis procedures are potentially life-threatening and must only occur by an order from a transfusion medicine physician with experience/competence in such procedures.
Definitions:
Policy:
References:
Revised 3/1/21
When I first moved overseas from the United States, I brought the perspective of my American training and experience. I saw everything in my new blood bank through those eyes.
Yet, most of my staff were not American or even North American. Few were even native in English, and most of those were not American. They had different qualifications, many of which would not have been accepted by the American schemes. Still, they functioned well.
I also worked with the US military technologist staff during Gulf War One. Some did not even have a Bachelor’s degree; yet, they performed the work well.
I used many technologies that were not yet (or never) US FDA approved such as gel or glass bead typings and pooled buffy coat platelet production. There were rare reagents I could buy off the shelf (e.g. anti-Tja/PP1Pk).
Later, I adopted pathogen-reduction technology (Mirasol), automated component production (Atreus then Reveos), and platelet additive solution. I achieve a level of good manufacturing practice that would have been difficult to achieve by the FDA-approved methods.
My perspective had changed. In the Middle East, I studied many frameworks and came to the conclusion that the best approach was to customize them to our local needs. My particular experience was to start with one framework, i.e. Council of Europe CE, and then localize it.
To do this, I could not use an American turnkey blood bank software for either the donor or patient operations. I needed a flexible system that could be customized to my needs. Again, I chose a CE-marked system, Medinfo Hematos IIG that had already been adapted to many frameworks.
It is much easier to work solely within one system such as FDA. However, if I had done that, I would have lost so much flexibility and not had a system optimized for local conditions. I would not have used Mirasol, Reveos, Diamed, and many other reagents.
One big disappointment at such international meetings is the perspective by one country’s regulatory agency that they feel its regulations and framework will work well overseas. I would wager that those people were not well acquainted with international conditions.
Another frustration was attending another international meeting in which the presenters apologized for the source of information since it came from a foreign country (France) and not their own (United States).
No country has a monopoly on what is best for everyone. To share our experiences and compare is so valuable. No one assume his way is the best. In my career, I have had the richest experiences studying other perspectives and my organizations have benefited greatly from the exchange. We can all learn from each other. We are citizens of the world.
Principle:
Kidneys have strong expression of ABO type and must be matched the same way as RBC components. In the case of ABO-incompatible renal transplants, we must not give significant amounts of plasma incompatible to the ABO type of the donor kidney. Plasma must also be compatible with the patient’s ABO type for RBC transfusions. The amount of residual plasma in PRBCs is limited since we use an additive solution SAGM. Likewise, platelet components are suspended in platelet additive solution with only minimal residual plasma. Cryoprecipitate has only minimal plasma and is given without regard to the patient’s ABO type.
All of the following rules can be built into the blood bank computer system Medinfo without hard coding.
Policy:
References:
Setting up ABO-incompatible renal transplants is a major undertaking and requires close coordination between Transfusion Medicine and the clinical team. This post addresses my experience in setting up this program in 2019 at HMC in Qatar.
Like any process involving titration, it is best to automate it to minimize inter-technologist variability. Unfortunately, doing both IgG and IgM titers takes up to 1 hour per machine and totally monopolizes the machine during that interval. I did not have sufficient staff to even consider doing the titrations manually. Performing automated titers disrupted my workflow so I encouraged the clinicians to send the specimens for off-peak processing.
Titration:
Columns:
Apheresis Equipment:
Staffing:
Specimen Collection:
Table of Permissible ABO Types:
Software:
Selection of blood component for ABO-incompatible renal transplantation is discussed in a separate post that will follow.
25/12/20
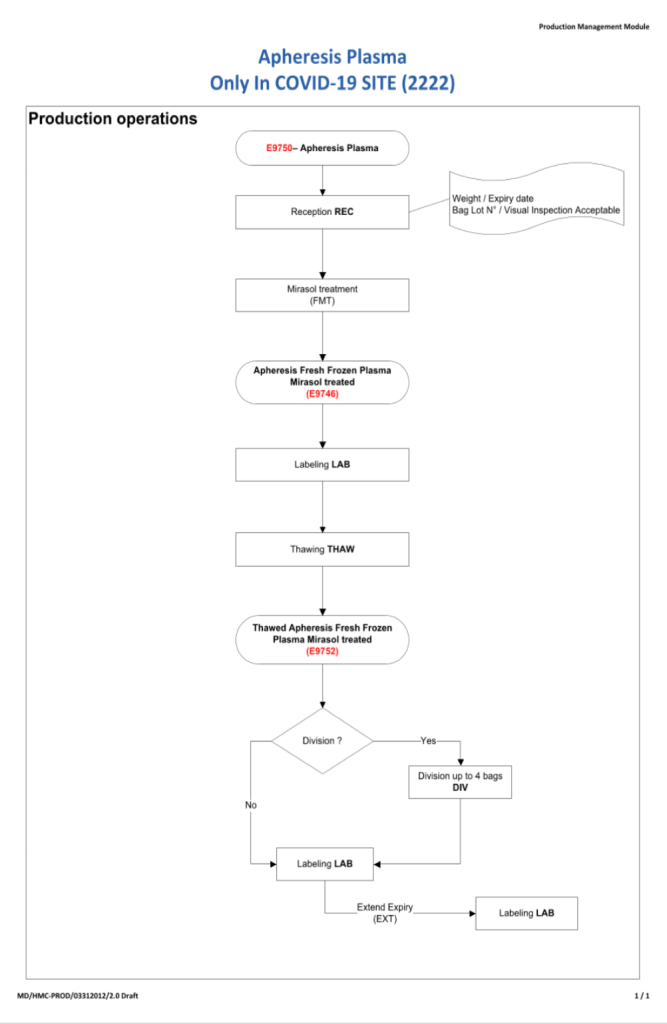
I will be posting a detailed series about the manual and software-enhanced COVID-19 processes that I set up in Qatar at HMC Doha in March-April 2020.
In this series I will provide you with screen shots of my Medinfo Hematos IIG software design for each step in the process: collection, processing, testing, inter-depot transfer, and hospital transfusion service/blood bank release.
This GMP-compliant software-enhanced system is based on the manual system I set up in early March 2020 at HMC.
I want to thank Medinfo Hematos IIG for their rapid response to building this parallel system based on my standard processes in so short a time (two weeks) and my special thanks to the software engineering team at Vital Health Technologies, the agent for Medinfo in Qatar.
To start the series, I am providing the basic workflow for the system. As is normal in Medinfo software design, a full mapping of the processes are made. This workflow shows the new CCP ISBT codes and the quarantine collection and processing steps. The donor testing (marker and immunohematology) processes are similar to those for regular donor units.
This is basically the same process both manually and in the software. I always say:
A good software process is based on a good manual process!!
Please note the following workflow for our initial discussion.
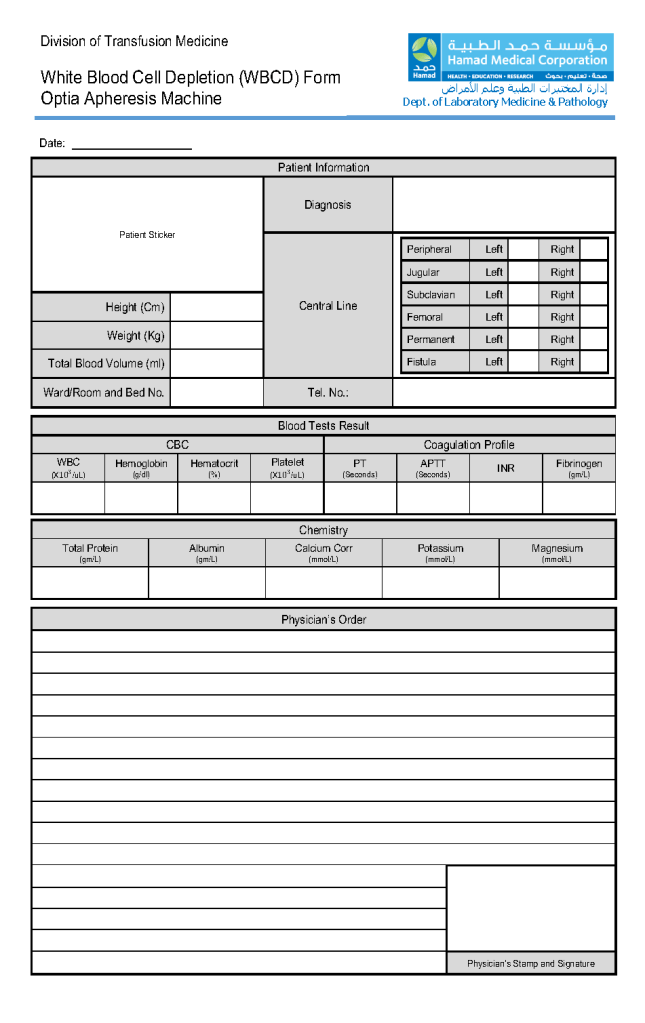
This form is the result of a collaborative effort between my therapeutic apheresis team and me. I want to thank Dr. Saloua Al Hmissi, Consultant, Transfusion Medicine, and Ms. Mini Paul, Head Apheresis Nurse for all their efforts.
This form can be readily converted into a computer data entry form–depending on your software’s capabilities.
Principle:
Since group AB plasma is in short supply, use of group A plasma with low anti-B titers may be substituted based on inventory levels.
Policy:
References:
This post outlines a framework for establishing the use of low-titer group A plasma as a universal donor. Manual titering large number of donor specimens in my organization is not practical. Using an automated system will also increase the precision of the results.
Process:
Special notes:
References:
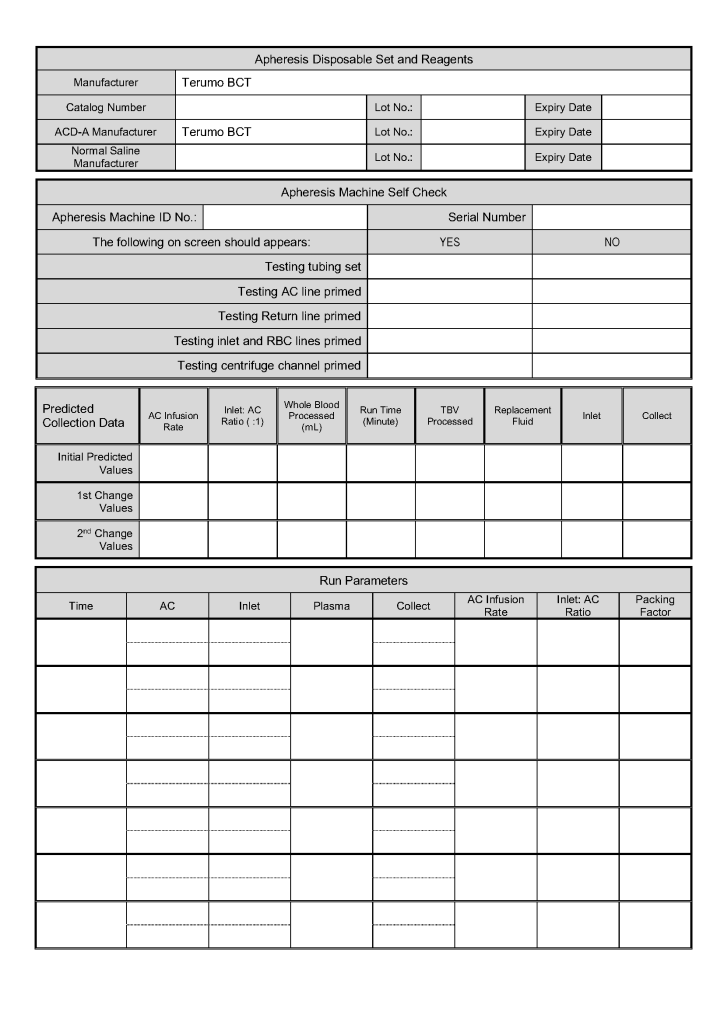
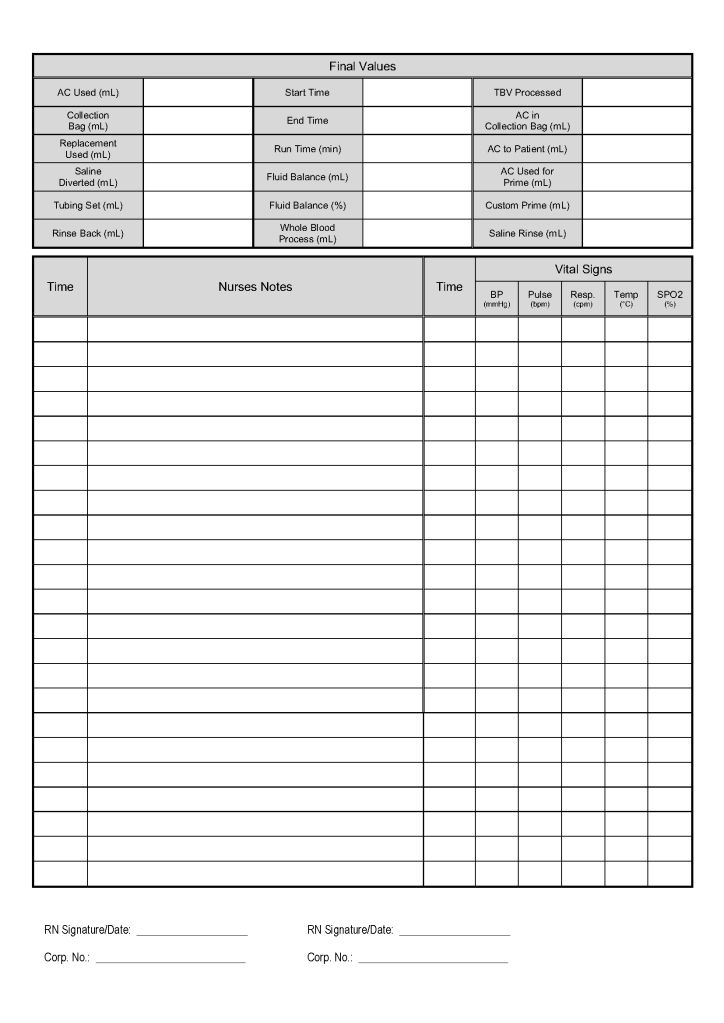
This is the apheresis form used for reductive thrombapheresis developed by my apheresis team and me. In particular, I want to thank Dr. Saloua Al Hmissi, Consultant Transfusion Medicine, and Ms. Mini Paul, Head Apheresis Nurse, all their hard work.
The attached form can be developed into a computer entry form if one has a suitable hospital information system. It is organized so that the apheresis nurse can quickly enter the data on one screen. Never forget that our goal is treat the patient–not spend all of our time on data entry!!
20/12/20
