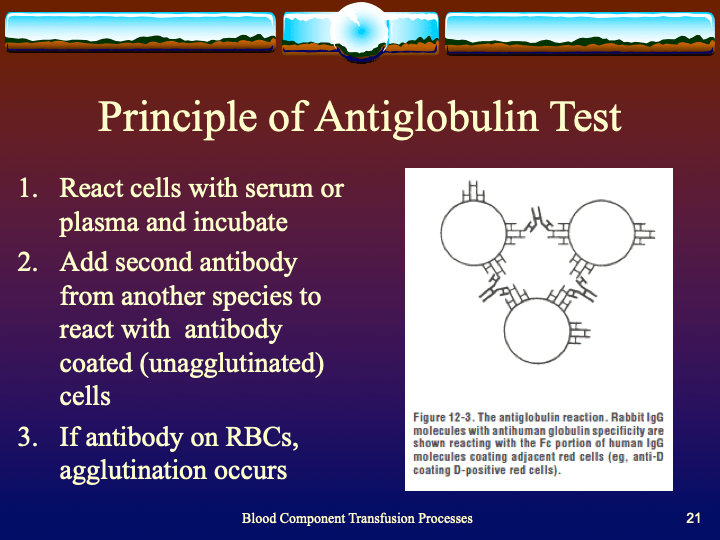
Antiglobulin reagents are used to detect molecules bound to the RBC surface. What they detect depends on their specificity. Such detection can be performed in the routine immunohematology laboratory or elsewhere such as flow cytometry. This discussion is for the blood bank laboratories, both routine and reference immunohematology.
This is how I classify and use the various reagents in my daily practice:
- Routine use—DAT testing and compatibility testing
- Antibody identification
- Drug-related hemolysis and transfusion reaction workups
- Special assays: DAT-negative AIHA, prediction of clinical significance of reaction by IgG subclass determination
There are many types of antiglobulin reagents:
- Polyspecific: IgG and complement usually C3d but sometimes C3b specificity included
- Whole Molecule IgG including mu heavy chains and kappa and lambda light chains
- Monospecific gamma heavy chain, mu heavy chain, alpha heavy chain, C3c, C3d, C3b
- IgG subclass: IgG1 IgG3
Whole molecule IgG detects class-specific mu heavy chains AND light chains kappa and lambda. Since kappa and lambda are found on all immunoglobulin classes, whole molecule reagents can detect IgM so there may be weak staining with cold antibodies that are not clinically significant.
C3d is the final breakdown product of C3b and does not cause hemolysis. Its presence merely means that at some time—unspecified—complement was fixed. C3c is an intermediate product in the breakdown pathway. If detected, C3c positivity means ACTIVE complement fixation was occurring at the time of specimen collection.
General Use:
Routine DAT testing:
- Polyspecific: if positive, then use
- Monospecific IgG and monospecific C3 reagents
Antibody workups:
Routine: antibody screens and AHG crossmatch (if indicated)
- Polyspecific
- Gamma heavy-chain monospecific
Monospecific gamma heavy chain is preferred to minimize non-clinically significant, cold antibody interference.
Complicated—where detection of complement reactivity is especially important:
Polyspecific for drug-related hemolysis and transfusion reactions
Difficult antibody workups, e.g. to rule out anti-Jka and/or anti-Jkb
Specialty Reference Procedures:
- DAT-negative AIHA: mu heavy chain, alpha heavy chain for IgM and IgA mediated hemolysis (rare), C3c to detect active complement fixation
- Predicting clinical significance: IgG1 IgG3
Complement fixation may be important in various drug-related hemolysis and some transfusion reactions so I always use a polyspecific reagent in these situations. Most antibodies can be detected by gamma heavy-chain specific reagents; however, there are rare examples of anti-Jka and anti-Jkb which are only detected by complement. Whenever I have a nonspecific reaction in an Jka-negative or Jkb-negative patient, I repeat the AHG panel using polyspecific reagents. I do not use polyspecific routinely because of the nonspecific and non-clinically significant cold antibodies.
One way to assess for the clinical significance of an antibody is to determine its IgG subclass. In general, IgG3 antibodies may fix complement and cause severe hemolysis. Both IgG1 and IgG3 antibodies cross the placenta and may cause hemolytic disease of the fetus/newborn.
In summary, when reviewing immunohematologic reactions using AHG, I always remember to check which type of AHG reagent was used. I always keep multiple types of AHG reagents in the laboratory for the reasons explained above.