I was recently talking with one of the hospital software system administrators from my previous site. He had originally worked on building the Medinfo system, but was then reassigned to the laboratory modules of the hospital information system.
His alarming comment to me was that the Medinfo build was completed so there was no need to worry about it now—it was finished. I guess he was looking from the perspective of the general laboratory software. There is no need to make major changes to the build, just update interfaces and troubleshoot.
I was surprised. He had no idea of how many times we have to update the structure for new rules and regulations, and changes in blood bank practice—let alone emerging pathogens such as ZIKA, dengue, Chikungunya, and most recently, COVID-19.
My daily morning routine was to survey several blood bank websites with changes to blood donor criteria including US FDA CBER, read the transfusion journals (Transfusion, Vox Sanguis, etc.), AABB, and ASFA. If there were any changes pertinent to our organization, I had to make interim policies and procedures, and finally prepare specifications for changes in the Medinfo software.
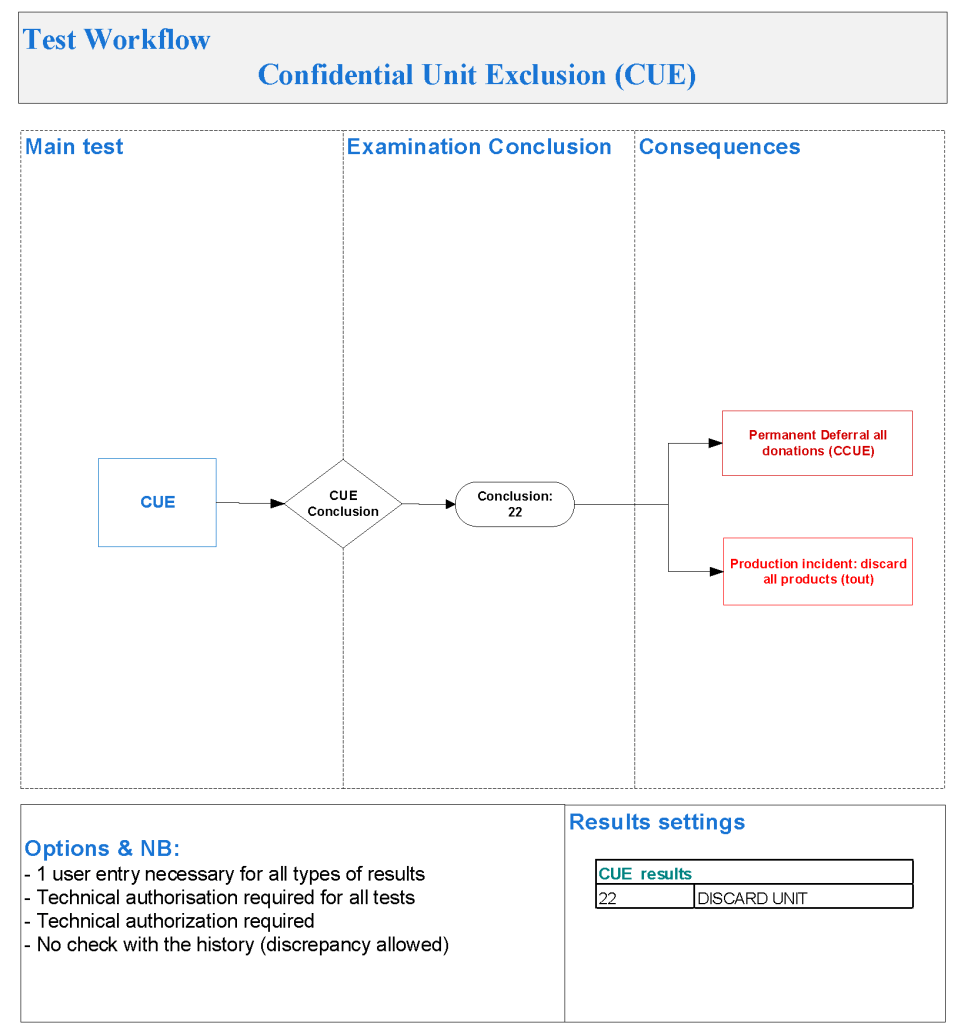
The Medinfo engineers would prepare flow charts of the proposed changes and implement them in a test environment for the Super-Users to test. I had to prepare validation protocols for the testing, and then review the validation results and finally approve the adoption of the changes.
I cannot remember even a month going by without some revision in the donor protocols. When COVID-19 came, I had to prepare a parallel, but separate, processing and allocation/release system.
This was a never-ending story that kept the Super Users and the local Medinfo engineers busy. I always reminded the hospital information system staff that playing with blood bank software was like playing with fire: there is a good chance you will get burned if you do not set it up properly.
31/10/20