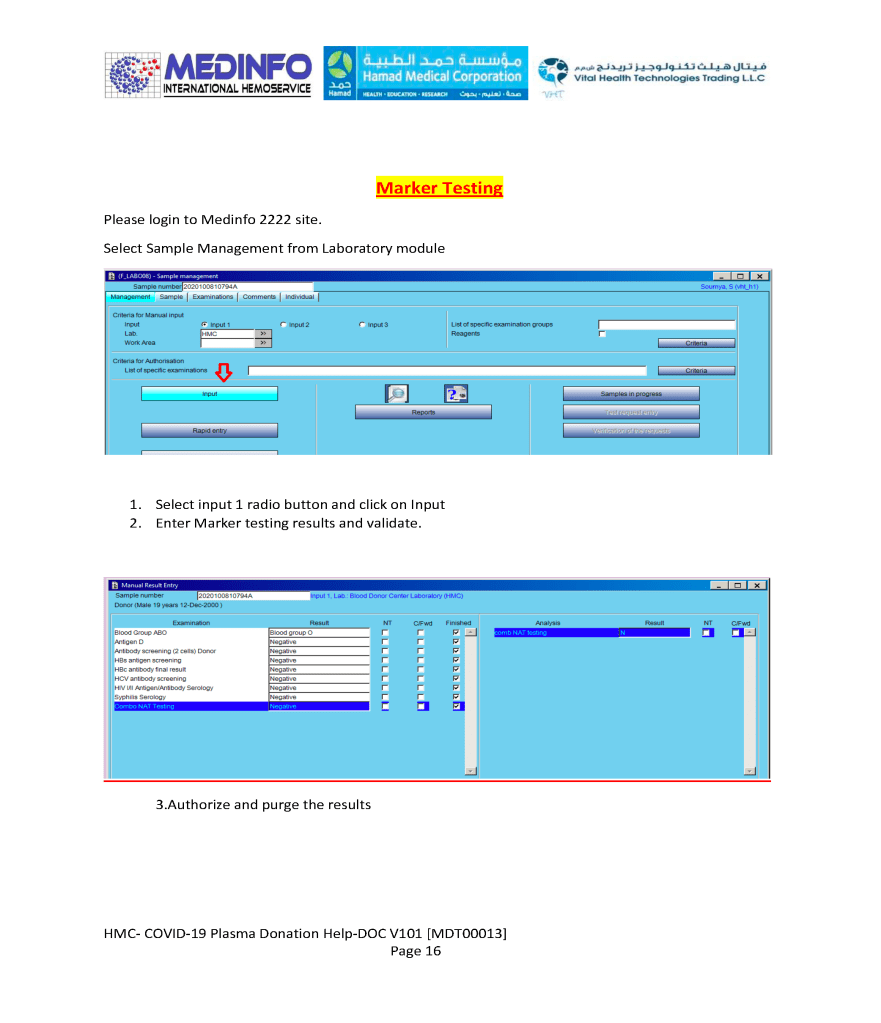
This is a part of a continuing series of posts on the actual Medinfo design of the CCP donation and release processes and covers CCP plasma thawing/labelling and donor marker testing. It highlights specific changes made for the parallel CCP system.
Thus, the machine interfaces for testing are the same as for regular testing and are not included in this document. Likewise, donor immunohematology testing is the same as for regular donors and is not addressed here
Once the blood component has left the hospital blood bank, it should be directed transported to the patient’s bedside for immediate transfusion.
At the bedside, the transfusionist (usually a nurse or doctor) must verify the information on the blood component labels (both the ISBT and specific reservation one for the patient). With a bedside device, this includes:
Scan the patient armband for hospital number
Scan ISBT label:
ABO/D type and any other antigen typings
Blood component type (RBCs, platelets, plasma, etc.)
Expiration date/time of the component
Verify Reservation Label (on back of unit)— centrally performed in blood bank computer system based on #1 and #2 above:
Intended recipient name and hospital number
Compatibility status (compatible, least-incompatible, etc.)
Expiration date/time of the compatibility testing/crossmatch
Record Documentation During Transfusion:
Physical inspection of the unit
Time stamp of transfusion start
Vital signs before starting transfusion
Periodic vital signs during transfusion
Time stamp of stopping transfusion
Any adverse effects during the transfusion
Any adverse effects after the transfusion (remote vital signs, oxygen saturation, EKG lead—if appropriate monitoring device attached to patient (e.g. Umana T1 device).
All of these parameters can be entered into a hand-held device that transmits them to the blood bank computer system (e.g. Medinfo Hemotrace.)
The Blood bank computer system (patient module) should verify that this is the proper unit for the intended recipient and that the transfusion is starting within the reservation limit of the unit and serves to verify the information on the reservation label attached on the back of the blood unit.
With a device such as the new Umana T1 device from the GPI group, the vital signs together with an EKG lead and oxygen saturation can be automatically uploaded into the handheld device that feeds into the blood bank computer system such as Medinfo Hematos IIG and/or directly transmitted to the blood bank software. This device can continuously record this information for several days and detect post-transfusion adverse effects such as TRALI/TACO and delayed hemolytic transfusion reactions.
Note:
Some other nursing hand-held devices are available for recording patient data but many cannot read the ISBT unit number or descriptor information. They also do not check with the blood bank computer system to check if the right unit of blood is being offered to the patient during the validity of the transfusion period (four hours after leaving the blood bank).
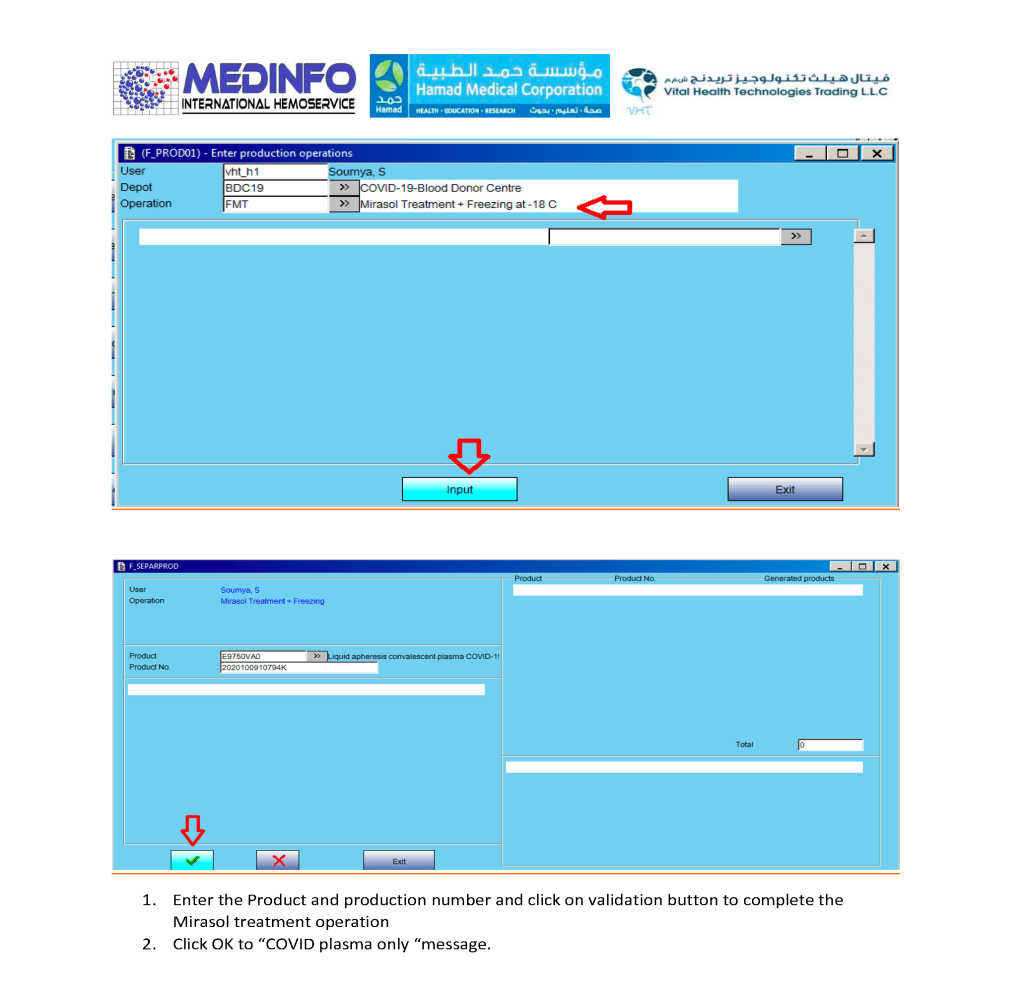
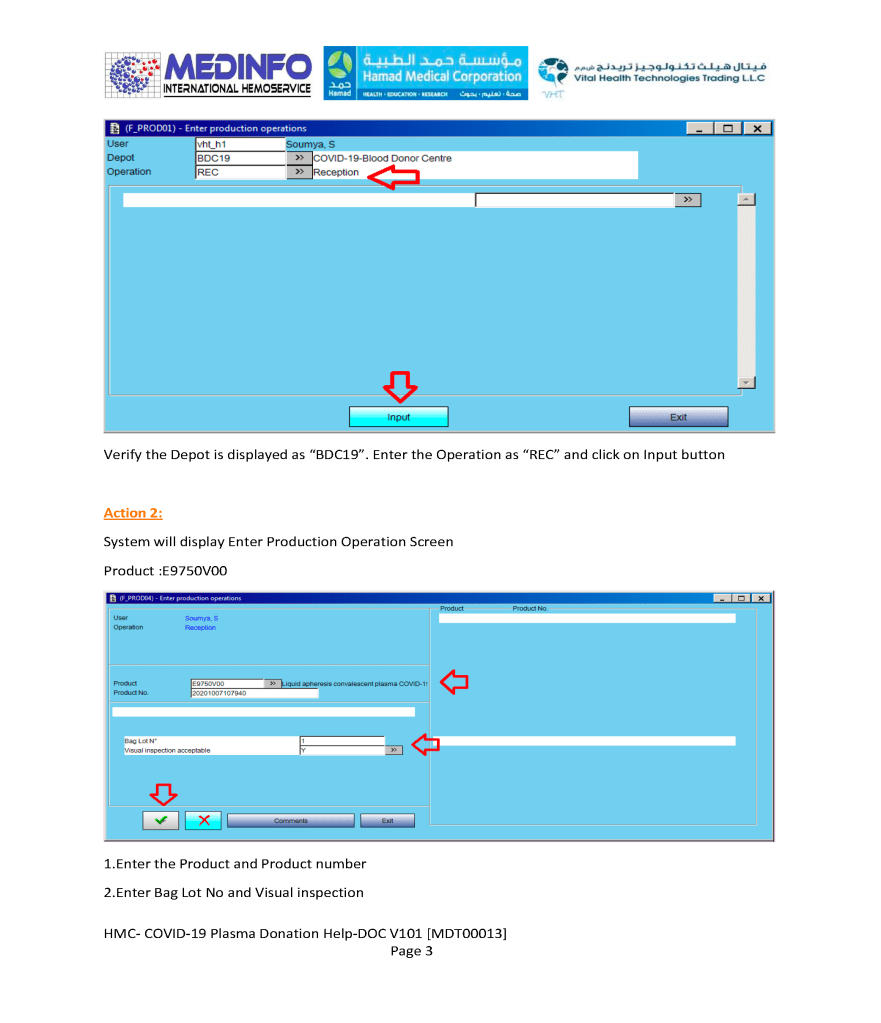
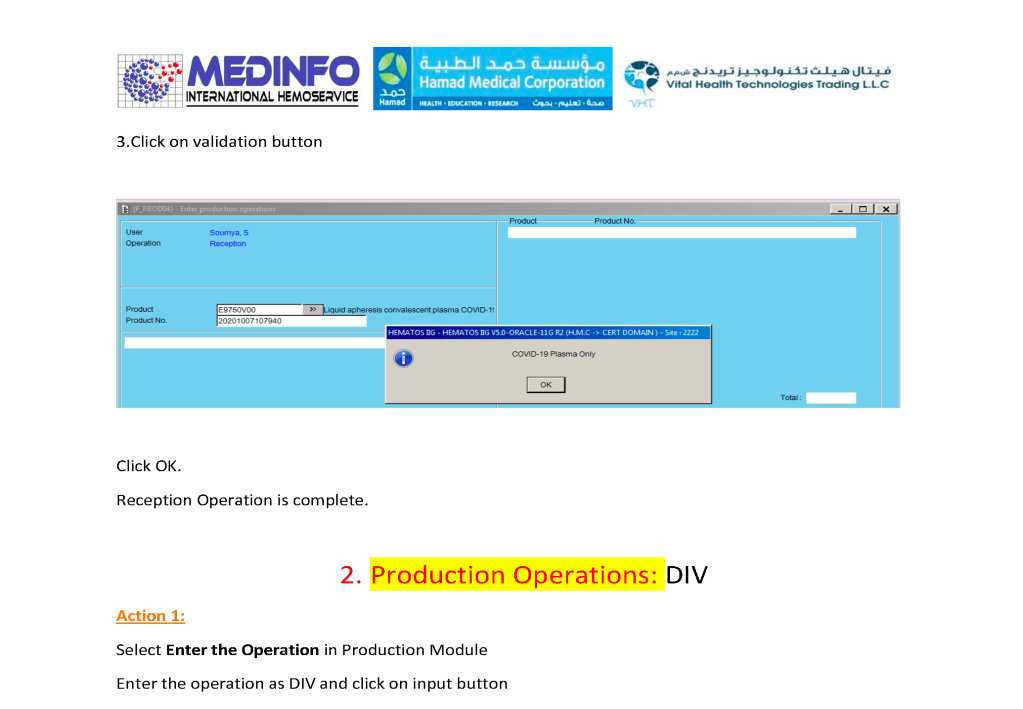
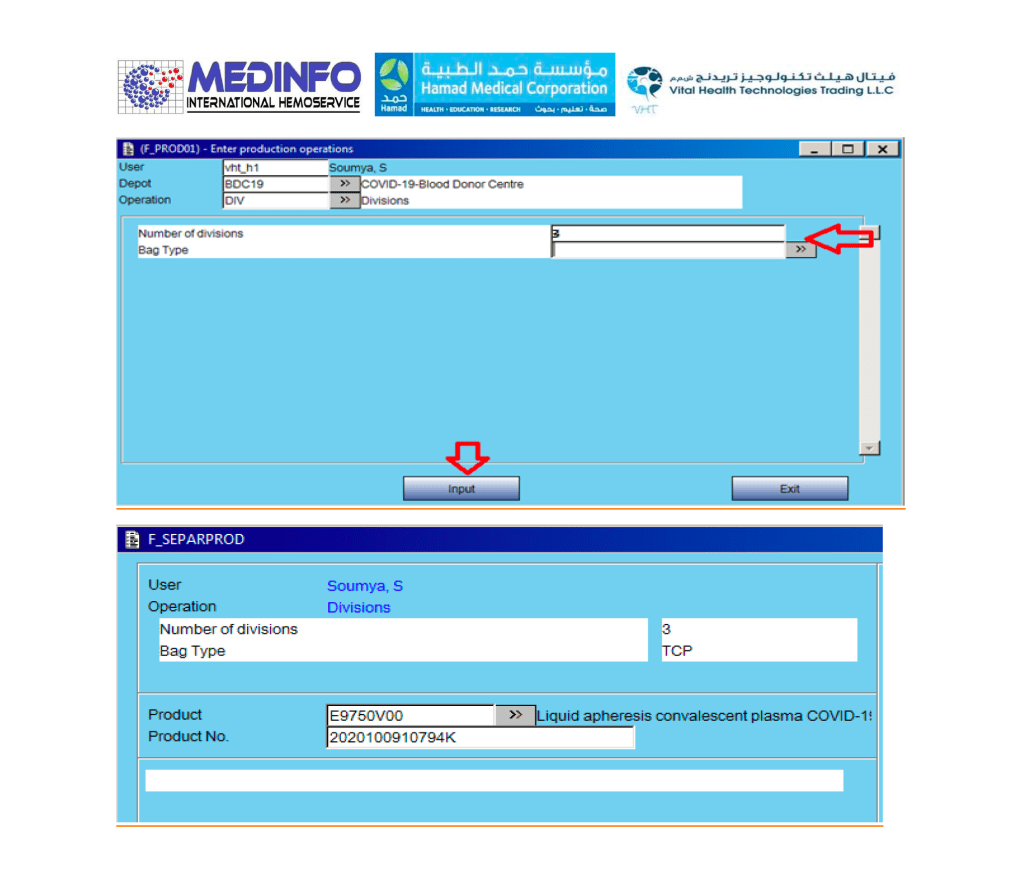
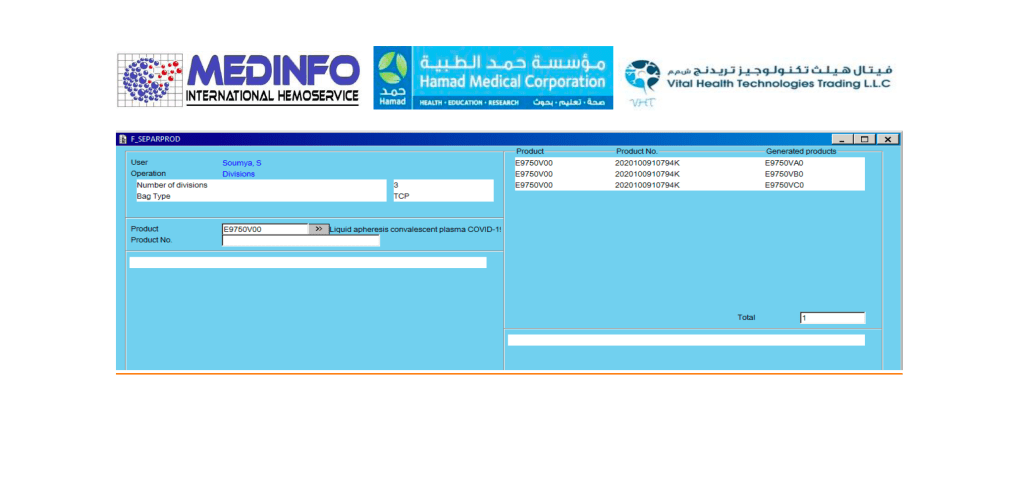
This is a part of a series of posts on the actual Medinfo design of the CCP donation and release processes. The registration of the donor and site, donor questionnaire/collection, and receipt/division of the product were covered in recent previous posts.
This is a part of a series of posts on the actual Medinfo design of the CCP donation and release processes. The registration of the donor and site and donor questionnaire/collection were covered in recent previous posts.
\
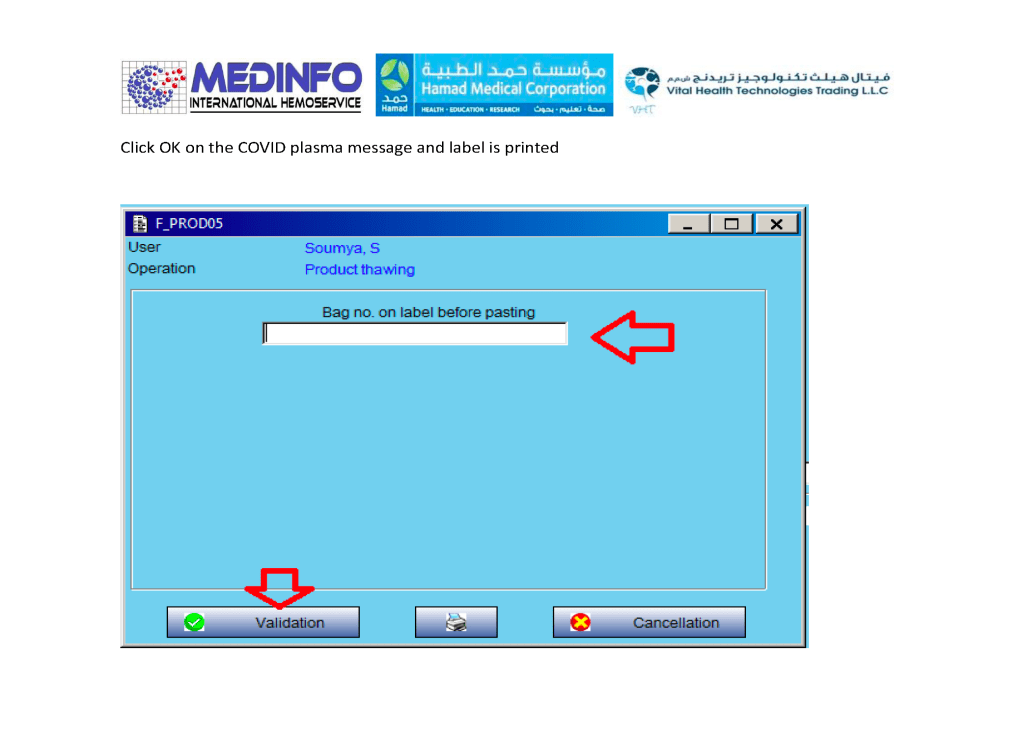
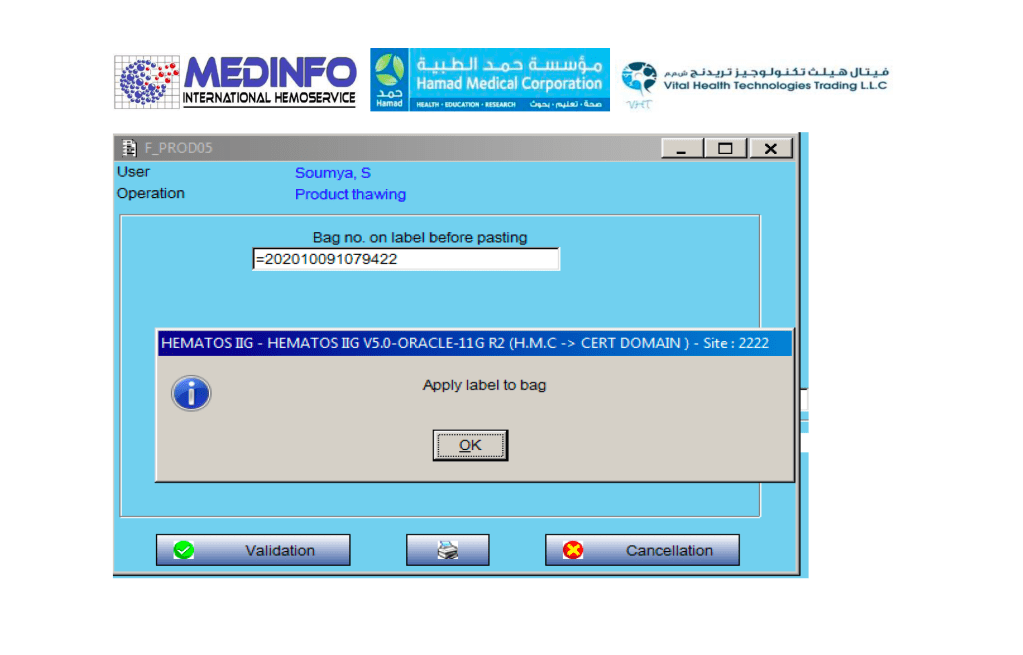
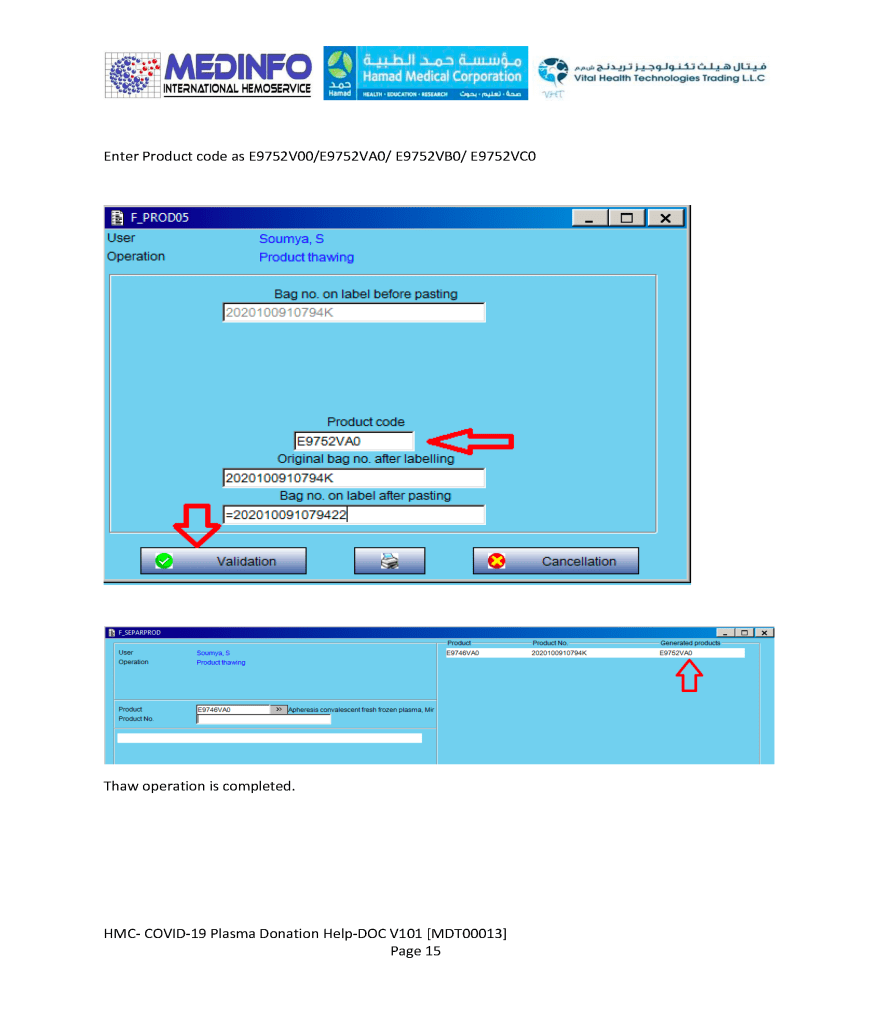
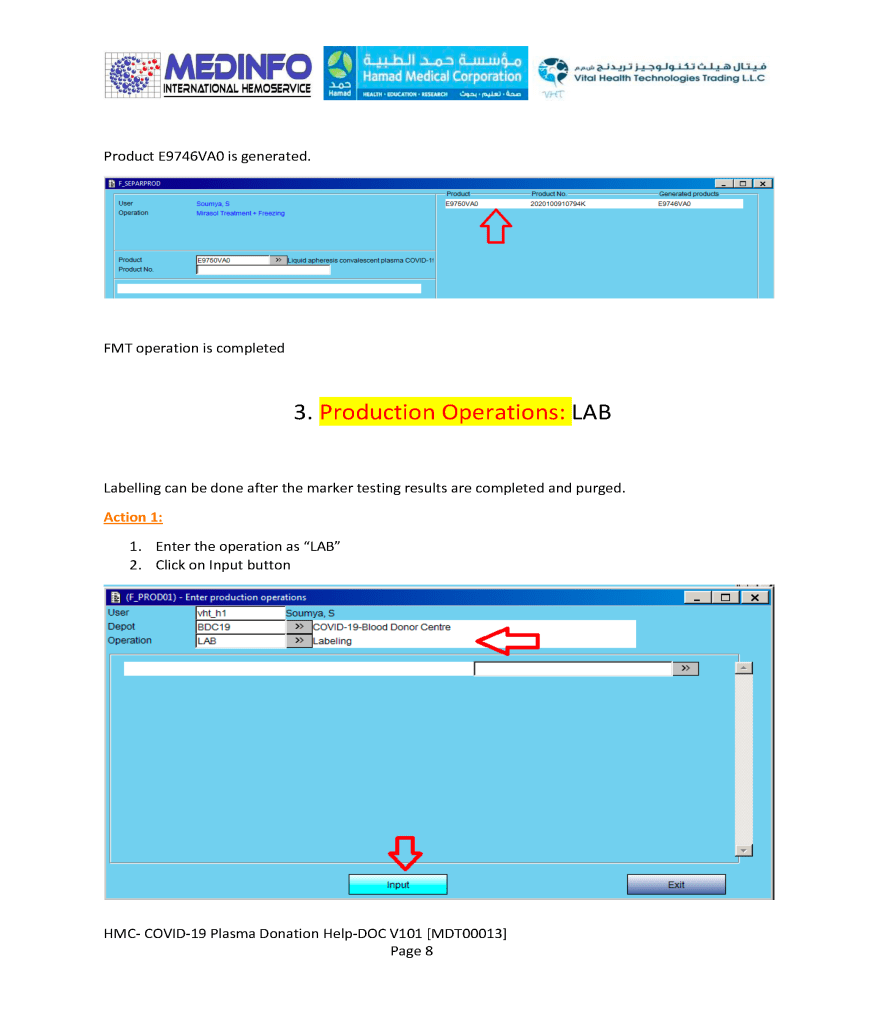
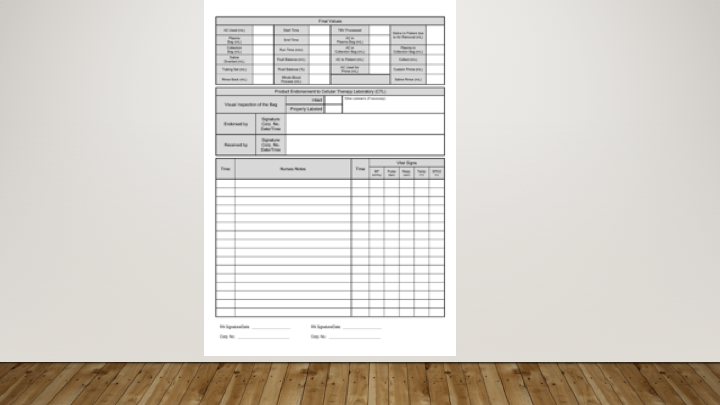
The process (pathogen-inactivation with Mirasol and freezing) wiil continue in a subsequent post.
Everyone is excited at the potential of using stem cells for research and therapy. Below is my presentation of the logistics necessary to get those stem collected in an orderly manner, especially in this time of the COVID-19 pandemic. It will also consider blood bank software logistics.
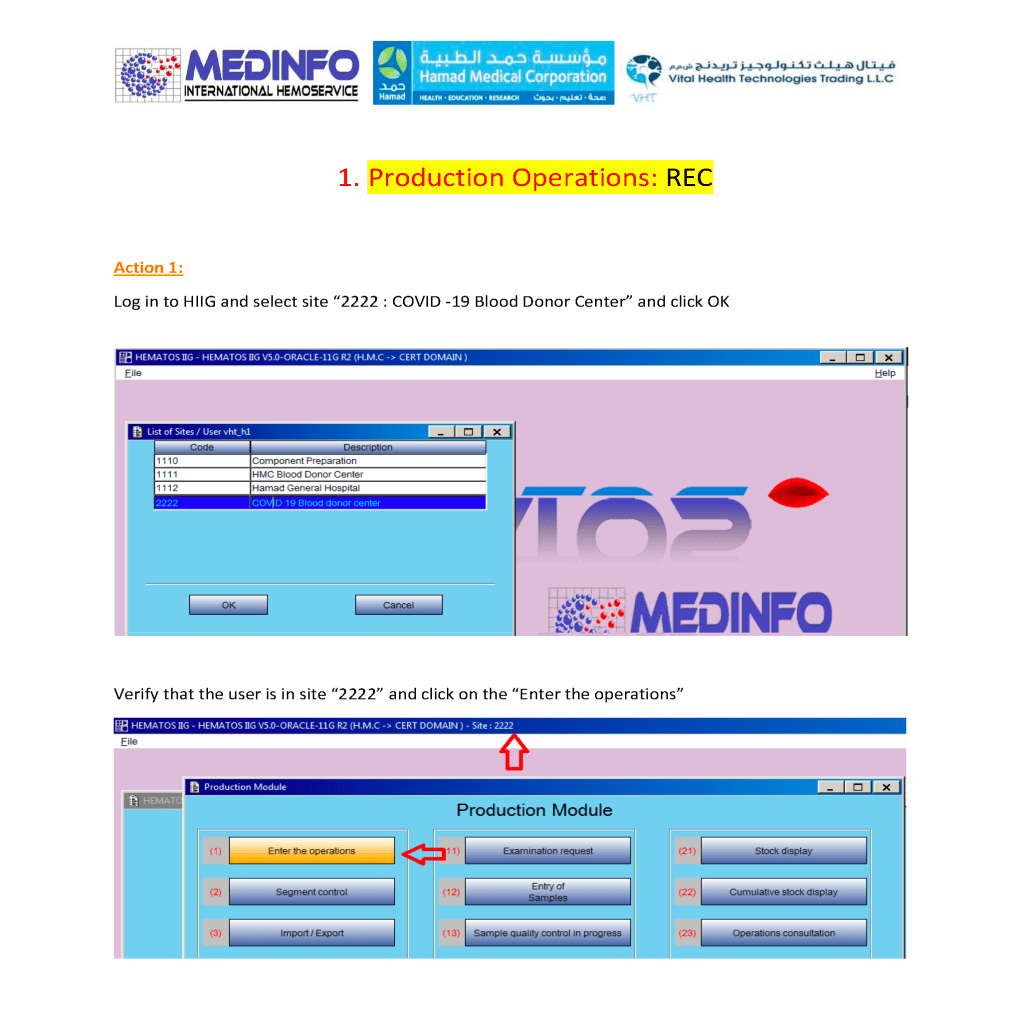
This is a part of a series of posts on the actual Medinfo design of the CCP donation and release processes. The site and donor registrations were covered in a recent previous post.
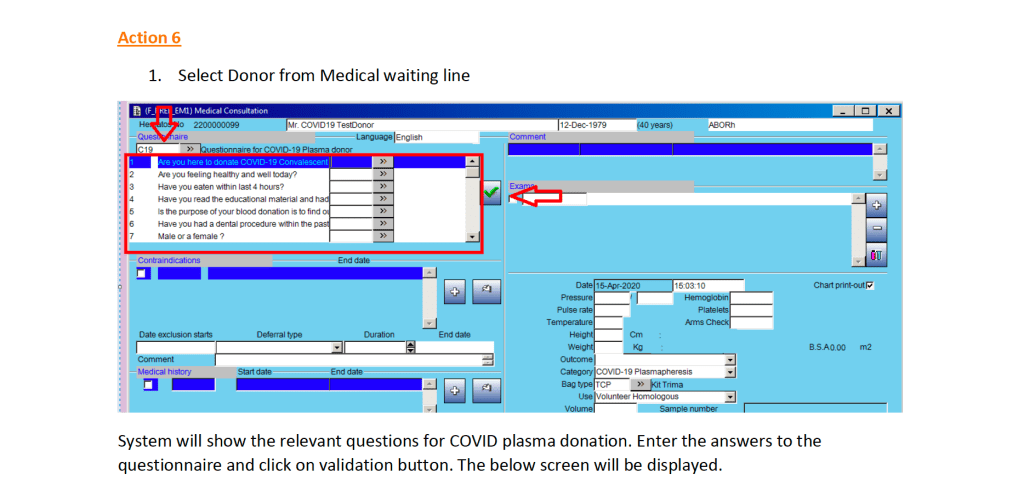
Donor Questionnaire and Physical Examination:
After registration, there is the online CCP donor questionnaire and vital signs entry.
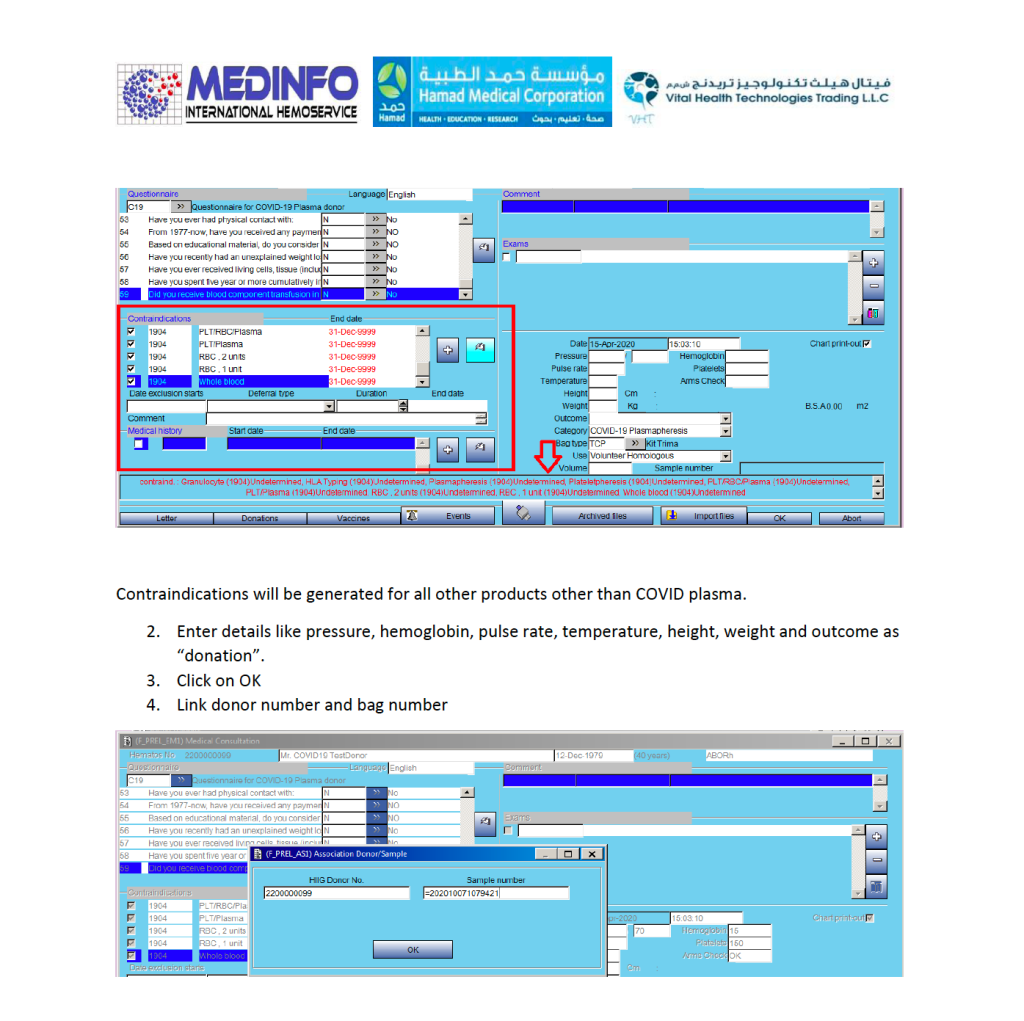
Note that the CCP donor will automatically be excluded from other types of donation. All other types will appear as contraindications in RED below.
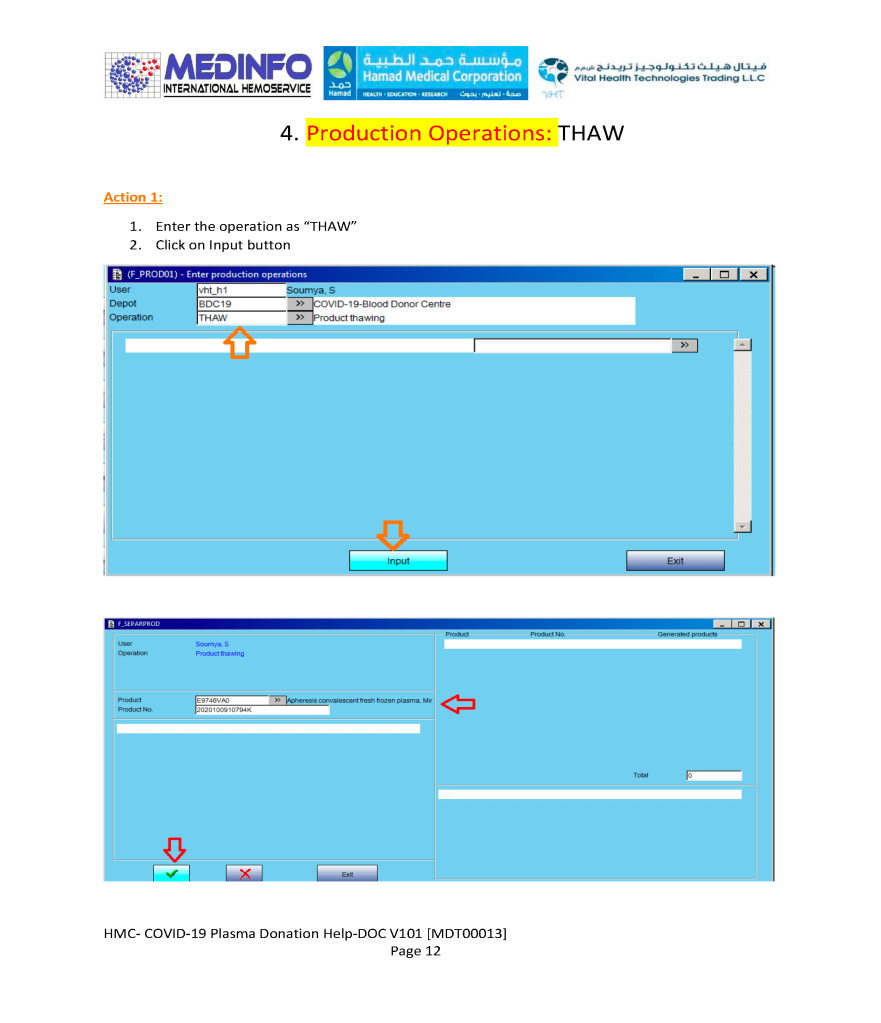
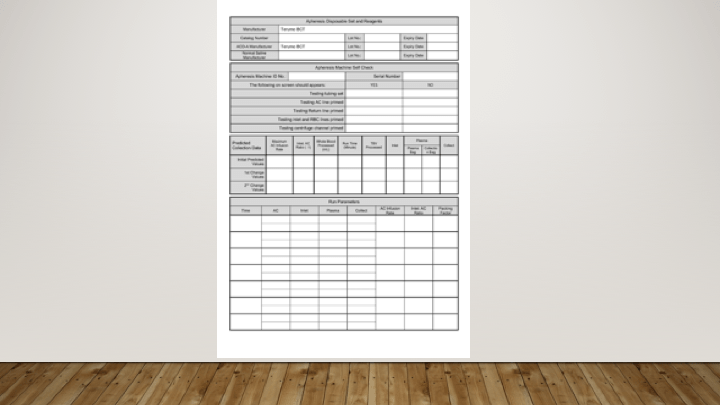
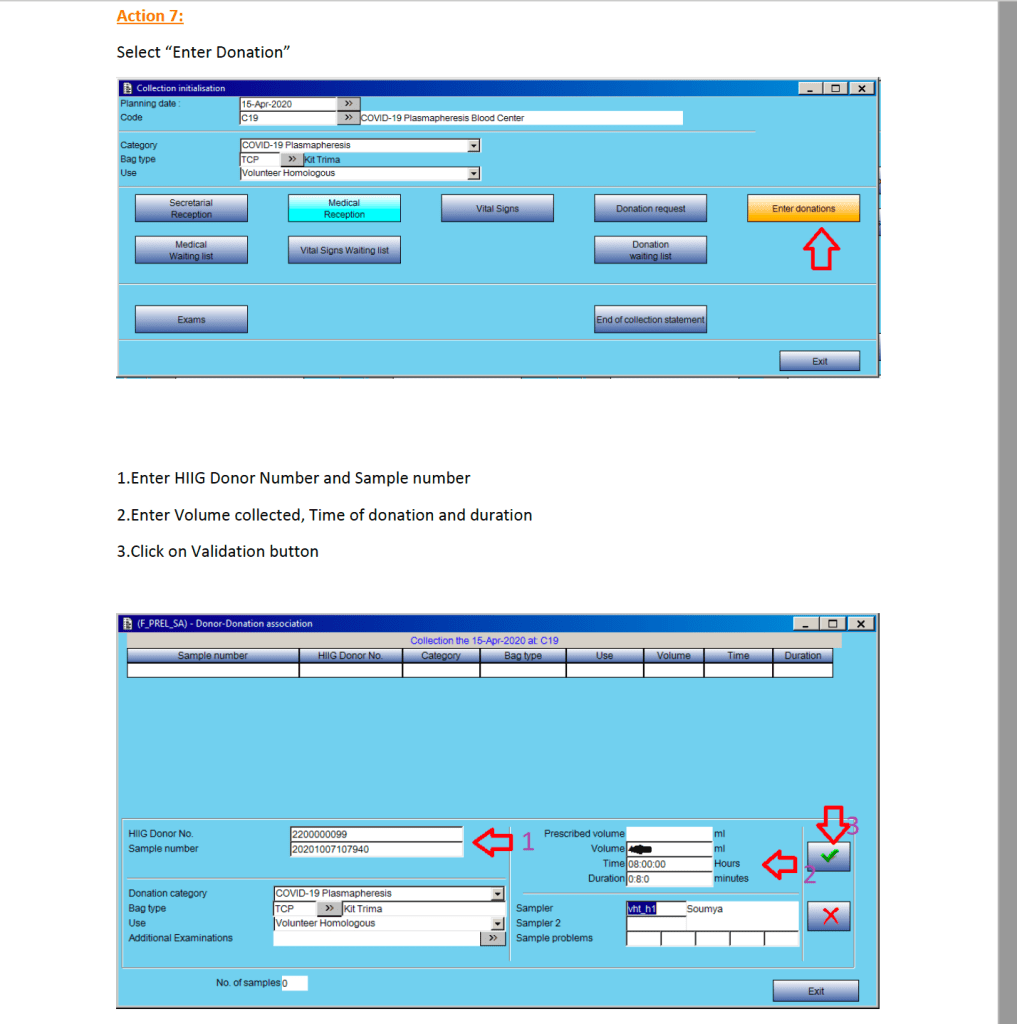
Donor Apheresis Collection:
The actual donation process is the same as for plasmapheresis donors:
At HMC Doha, we had a limited bidirectional interface between Medinfo Hematos IIG blood bank software donor and patient modules and the hospital information system HIS Cerner Millennium for blood component and limited blood bank testing ordering and return of the blood component ordering statuses and all blood bank test results.
For the purpose of COVID Convalescent Plasma CCP, the following specifications applied:
Ordering of CCP was either by number of units (average 220 ml each) or volume in ml (up to 200 ml).
Maximum order was 2 units.
Only designated physicians could order CCP.
A valid type and screen (72 hour maximal validity) had to be in effect to place an order for CCP.
If not valid, a new type and screen must be ordered before ordering CCP.
Selection of the ABO type of CCP was at the discretion of blood bank using its standard algorithms.
Status of order (ordered, received in blood bank, in process in blood bank, or released) would show in the HIS.
Note: Bedside documentation of the component transfusion was the NOT the responsibility of Transfusion Medicine or Medinfo Hematos IIG.
In my career, I have dealt with many different laboratory software vendors. Regretfully, not all encounters have been straight-forward. Since ultimately these products are used for patient care, I had hoped that there would be a sacred trust to do what is best.
Things that bother me:
Current state: whoever prepared it for the client, didn’t care or understand the local processes and came up with a generic: Order it, collect it, receive it, do it, report it for each and every test.
No training for super users: more like lambs being led to the slaughter. They will obey the vendor out of fear of making a mistake.
No discussion of options: pushing us to take the default setting—not even offering the available options. The only way you find out there are available options is because other staff have used the same software at other institutions which used these options.
Corrections to build: only giving one shot to do it right, further corrections cost $$
Scenarios: vendor shows specially crafted scenarios that “work” but when you ask the vendor to do a random, non-scripted scenario, it crashes.
Scalability: limited scalability on client’s chosen platform. That may force a rebuilding of the software when the limit is reached.
Reference site does not match the test volume or activities of the client, uses different platform, and thus you cannot make a valid assessment.
Performance issues: if you don’t know why the system is slow, you can add more hardware (RAM, disk space, etc.) and try again—it can’t be due to the software design!
Handling of requests: does not permit your local IT staff to make changes, must send it back to the vendor for $$
Waiting until hell freezes over: will we get the corrected/updated package during this reincarnation?
Interfaces: an acceptable communication link is when one side speaks Sanskrit and the other Algonquin and they both hear each other, but who cares if they understand?
Waiting for Godot: God forbid if your equipment needs an interface not currently available: how many cycles of the big bang can you wait?
Champions or Heroes: make a class of users who are to be evangelists for the new system and have them undergo sensitivity training including actions that are culturally irrelevant. Don’t tailor it to local sensitivities or customs. Will this convince the staff how useful the software is?
Relevance of vendor experts: Assume everyone understands what maple syrup is or comes from Kansas. The expert assumes everyone has the same background as his/hers. Who in the Middle East has seen maple syrup being made? How can that analogy be useful for building software?
Describe all reference units in feet/pounds/inches/furlongs/fortnights—no metric. Do not use SI.
Mix 24-hour clock with 12-hour clock: what does 12:00 mean? How do you measure time intervals?
Consulting companies: They are supposed to assist the client with the settings, but do they have the client’s best interests at heart? Some are good spin-doctors and transfer blame to the client’s software staff when it is really their responsibility for the build.
Rush, rush, rush: Administrative powers who just want everything done quickly whether or not it is correct or validated properly, who cares if the processes built are right?