Hepatitis B donor screening consists of HBsAg and HBcAb for all donors, the latter to detect the window period. In the USA, a non-negative HBcAb result will trigger a deferral. In the Gulf area/KSA, there HBV was positive higher than in the West so there was a high rate of HBcAb positivity often from recovered HBV infection.
Here was my last algorithm before I left HMC Doha, which allowed use of donors with protective titers of HBsAb. Note that the WHO cut-off for this is 10 IU/L whereas we used 100 IU/L as our threshold:
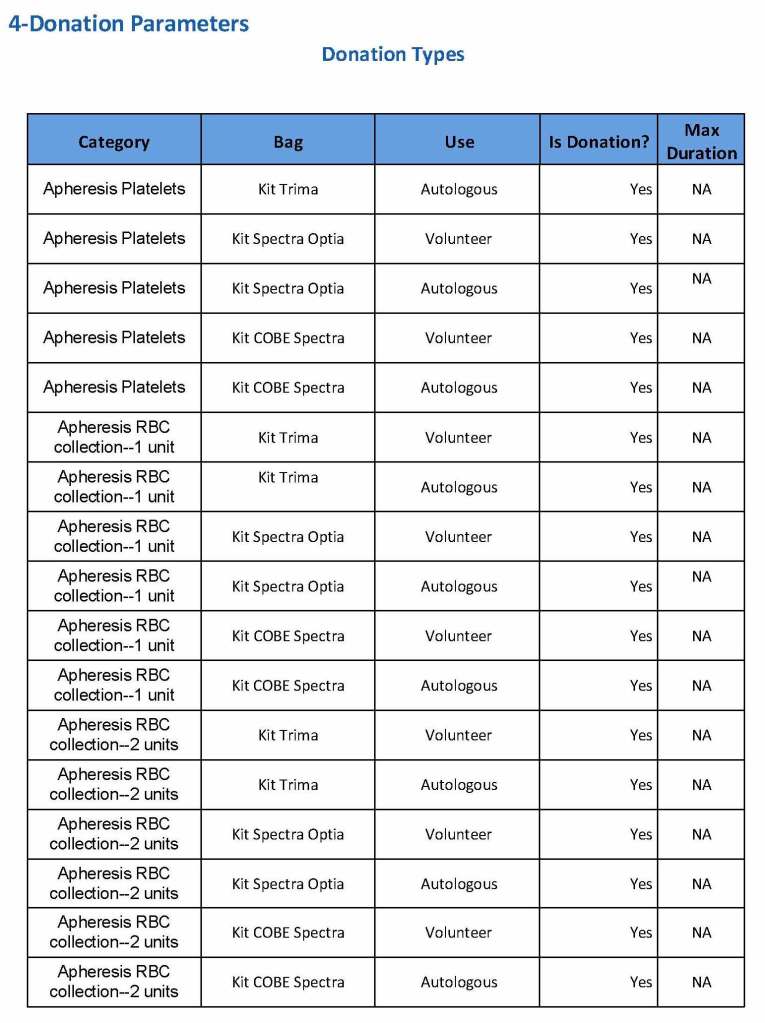
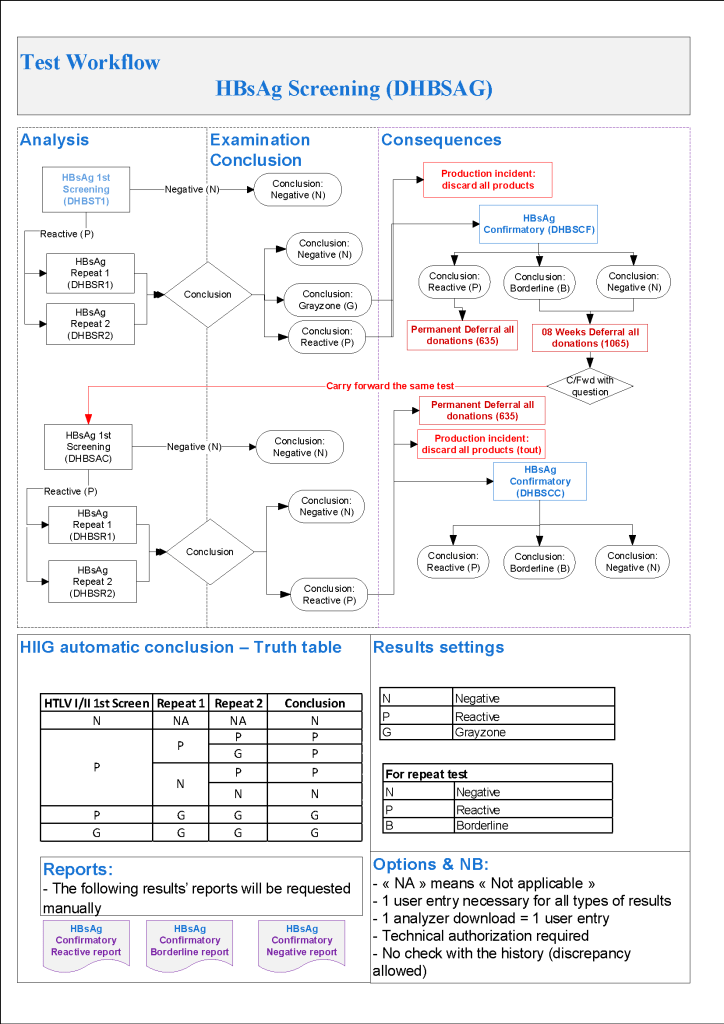
- Hepatitis B:
- HBsAg non-negative, then:
- HBsAg positive with HBsAg confirmatory positive, regardless of other results: permanent deferral, refer to Infectious Disease clinic
- HBsAg positive with HBsAg confirmatory borderline or negative, repeat all HBV testing after 8 weeks
- HBsAg borderline: repeat all HBV testing after 8 weeks
- HBV-DNA positive confirmed, regardless of other results: permanent deferral, refer to Infectious Disease clinic
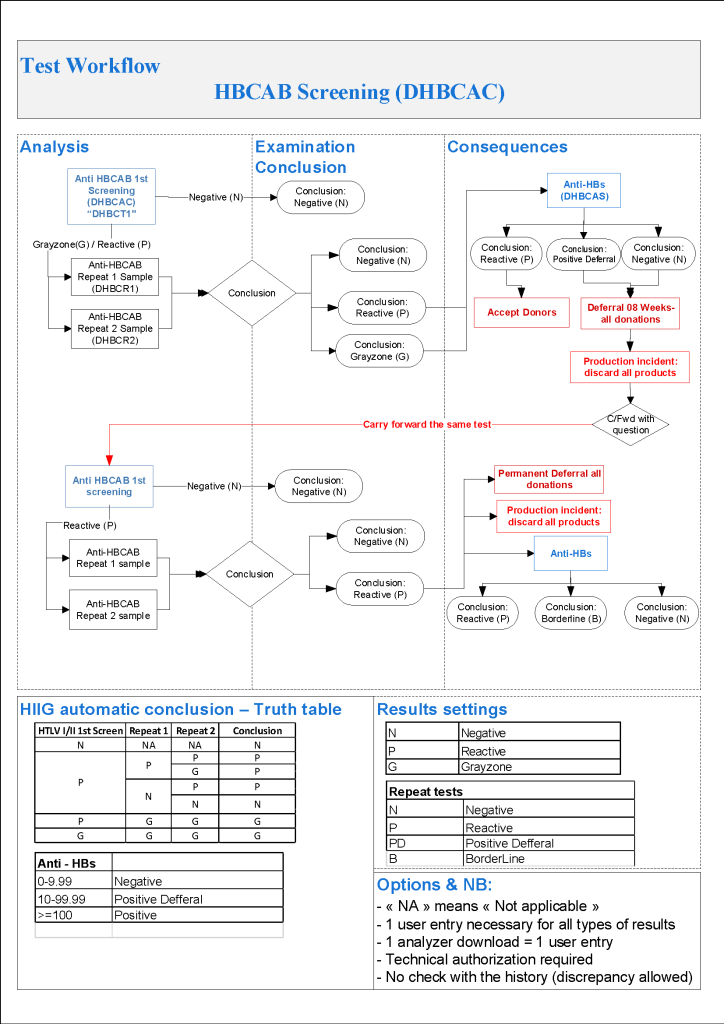
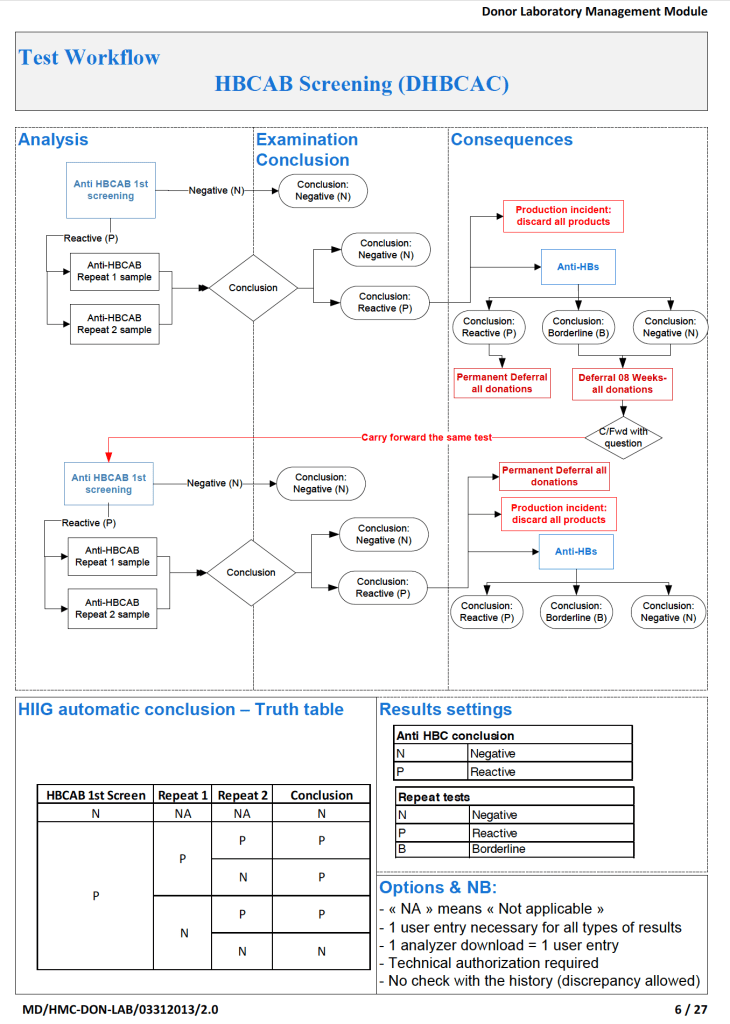
- If HBcAb positive, repeat after 8 weeks
- Repeat Hepatitis B Testing After 8 weeks:
- HBsAg positive with HBsAg confirmatory positive: permanent deferral, refer to Infectious Disease clinic
- HBsAg positive with HBsAg confirmatory borderline or negative: permanent deferral, refer to Infectious Disease clinic
- HBsAg borderline, permanent deferral, refer to Infectious Disease clinic
- HBV-DNA positive confirmed: permanent deferral, refer to Infectious Disease clinic
- HBcAb positive or borderline with negative HBsAg and negative HBV-DNA: review HBsAb level:
- If HBsAb level >= 100 mIU/mL (100 IU/L), donor may be reentered
- If HBsAb level < 100, then recommend to donor to receive booster HBV vaccine
- After HBV vaccine administration, retest after 30 days:
- If HBsAb level >= 100, donor may be reentered
- If HBsAb level < 100, donor is indefinitely deferred
- After HBV vaccine administration, retest after 30 days:
- HBsAg, HBcAb, HBsAb all negative: reenter into donor pool
- HBsAg non-negative, then:
Here is the HBcAb and HBsAb part of the algorithm:
Previously, we had we had disqualified any donor with a nonnegative HBcAb:
To Be Continued:
18/8/20