I started building this using the Uniform Donor Questionnaire UDQ from the AABB; however, I modified it to include coverage for Chikungunya, Zika, etc. and to include enhanced processes for malaria based on the Australian Red Cross.
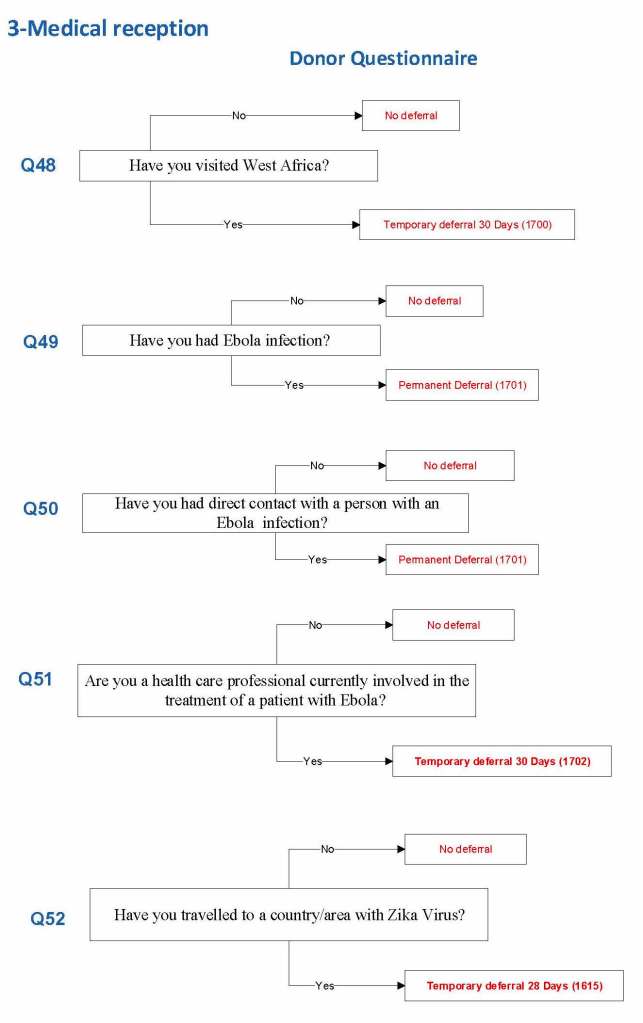
For each screening question, I prepared the exact wording (usually the UDQ’s) and set the deferral to temporary (how many days) or permanent.
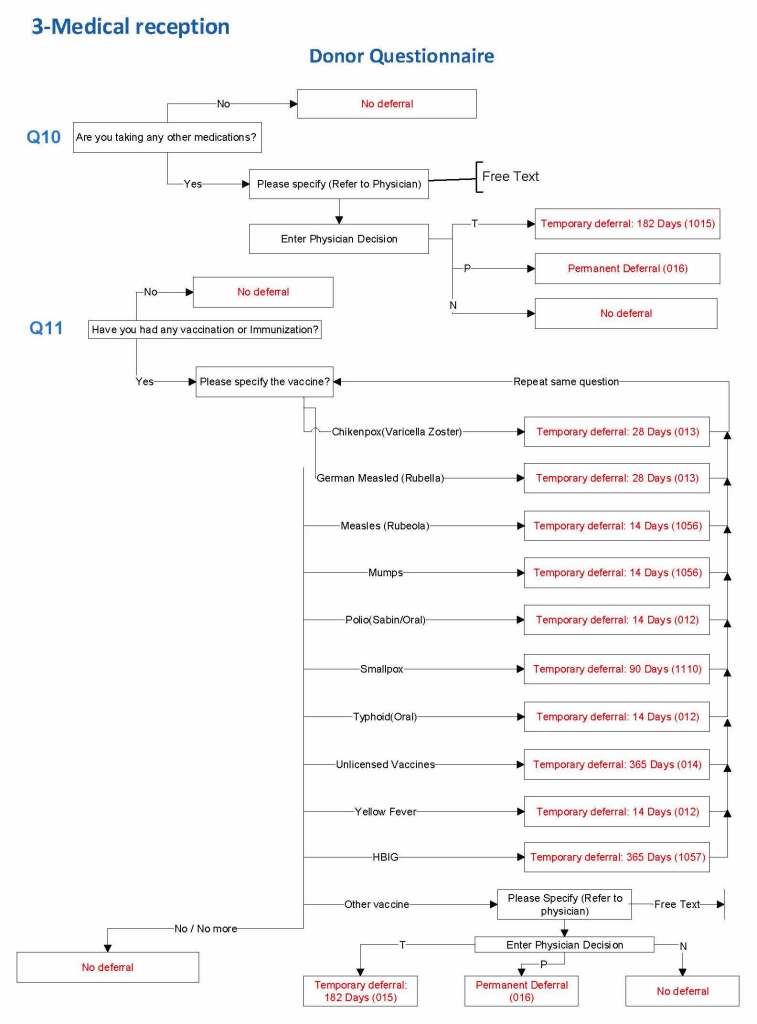
Some questions were more open-ended, and the interviewer manually entered a medication, surgical procedure, etc. The transfusion physician would review this and assign a temporary (specifying the interval) or permanent deferral.
The questionnaire was constantly being updated by changes. My role was to review different accreditation systems (AABB, CE, etc.) and the World Health Organization’s websites. I would then prepare an interim policy and pass the specifications for the changes to the Medinfo software engineer and when ready, finally to the Super Users for testing. If there was an urgent change, the whole process could be completed in less than one day including validation testing.
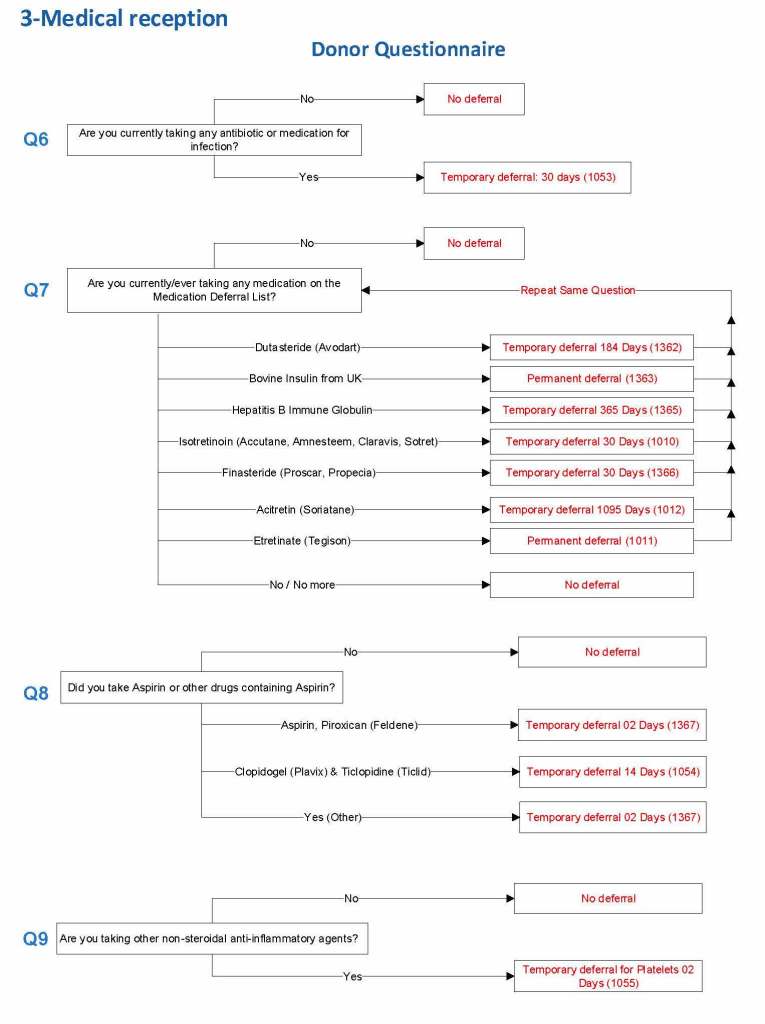
The following shows examples of the software processes:
Medications
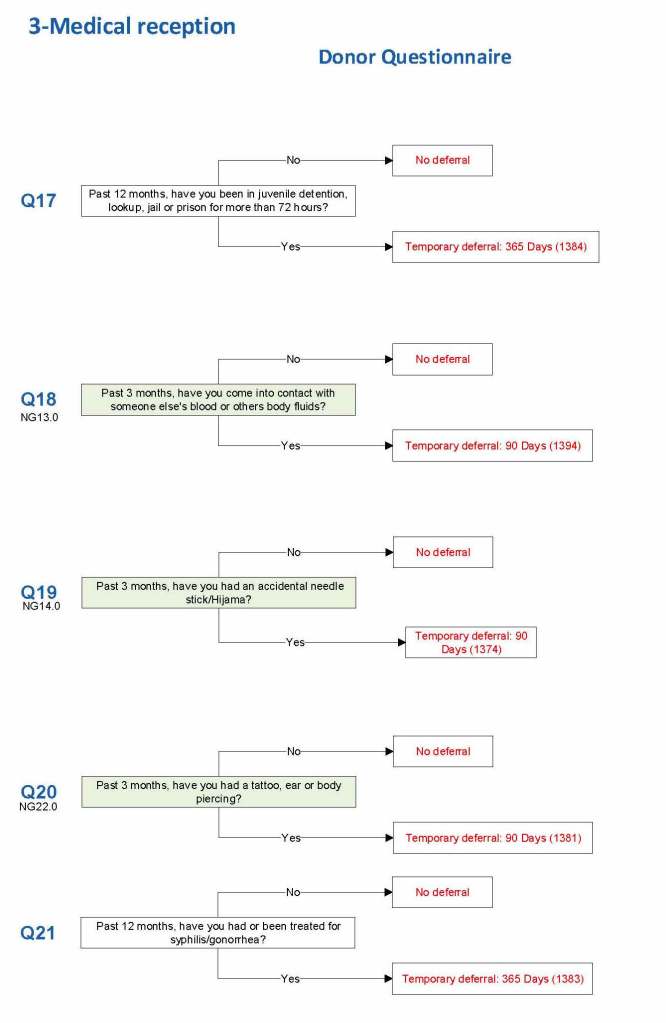
Body fluid exposures
Vaccinations
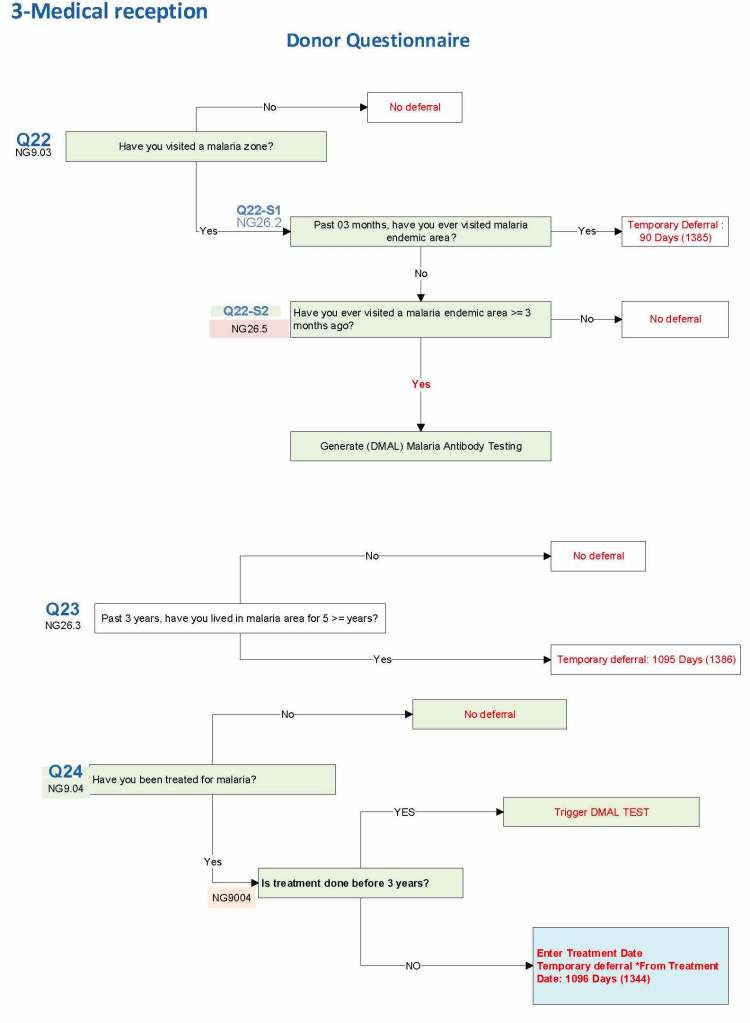
Malaria
Ebola/Zika
I emphasize that all of these settings are user-definable (at least in jurisdictions that permit all open, non-turnkey software).
Medication Questions:
Vaccinations:
Blood and Body Fluid Exposures:
Malaria Example: DMAL refers to the malaria antibody test.
Building the Software Processes for the Donor Collection 5:Donor Physical Examination and Adverse Reaction Reporting
Donor Physical Examination and Adverse Reactions
Donor physical examination, along with the donor questionnaire, are important both for donor and patient safety. In general:
Is it safe for the donor to donate?
Is it safe for the patient to receive the blood even if it is safe for the donor to donate.
Any donor who does not feel well must not donate. This may be the single most important step in ensuring a safe blood supply.
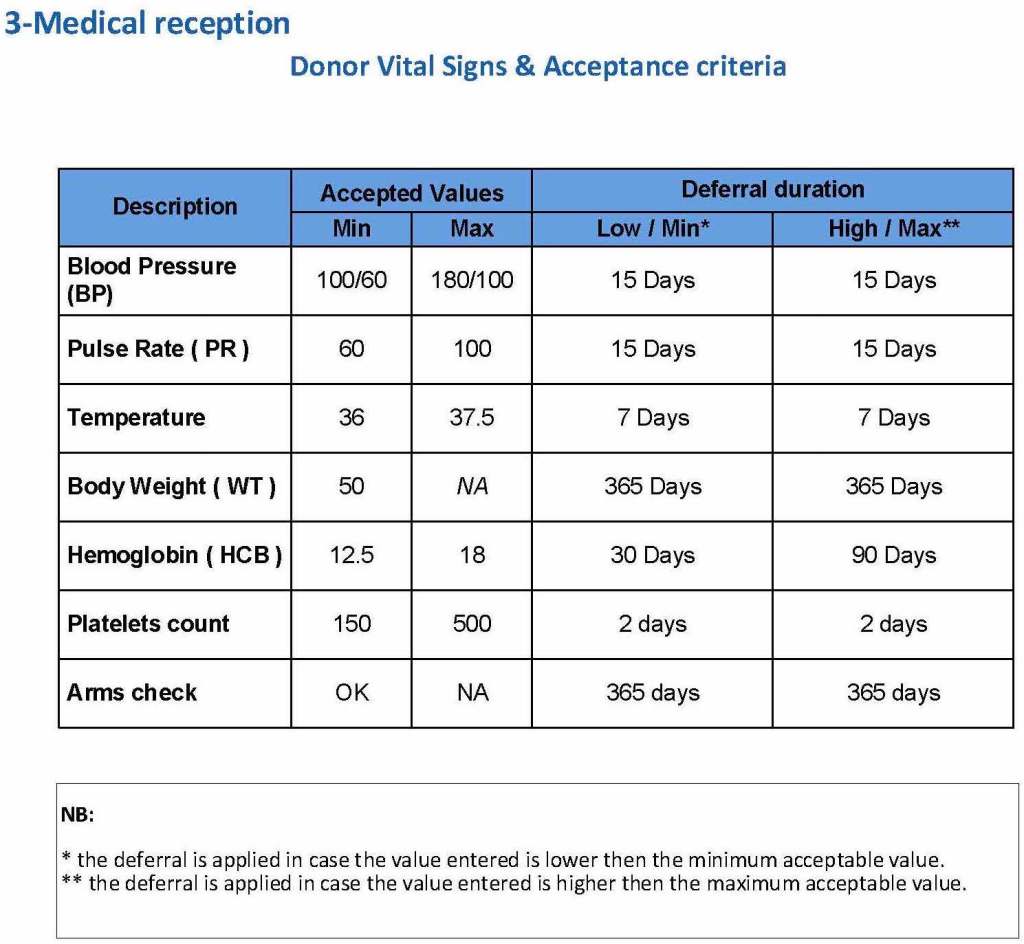
The donor physical examination includes the vital signs (blood pressure, pulse, temperature, heart rate, and temperature). I have attached a sample set of criteria for review. All are user-definable. Note how the arm examination is also included (looking for scarring, skin lesions, etc.)
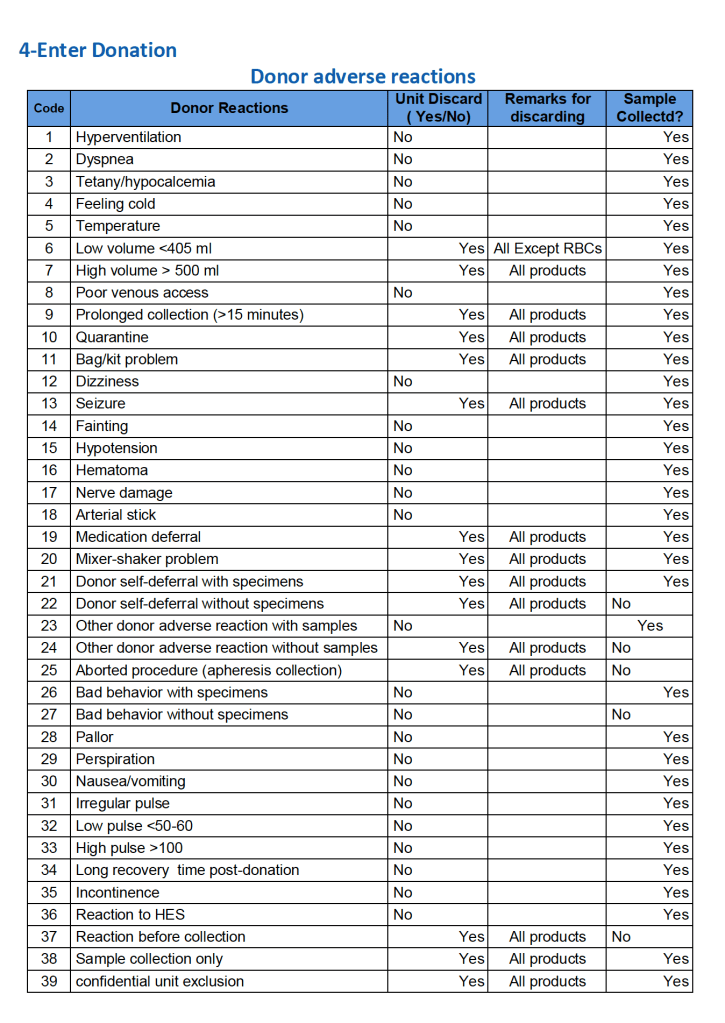
For all types of donations, there may be adverse reactions. These must be documented in the record along with the disposition of the donation. Will the donor need an extended deferral if the RBCs in the apheresis run are not returned? This can be built from the reaction documentation. Note the following sample table of reactions.
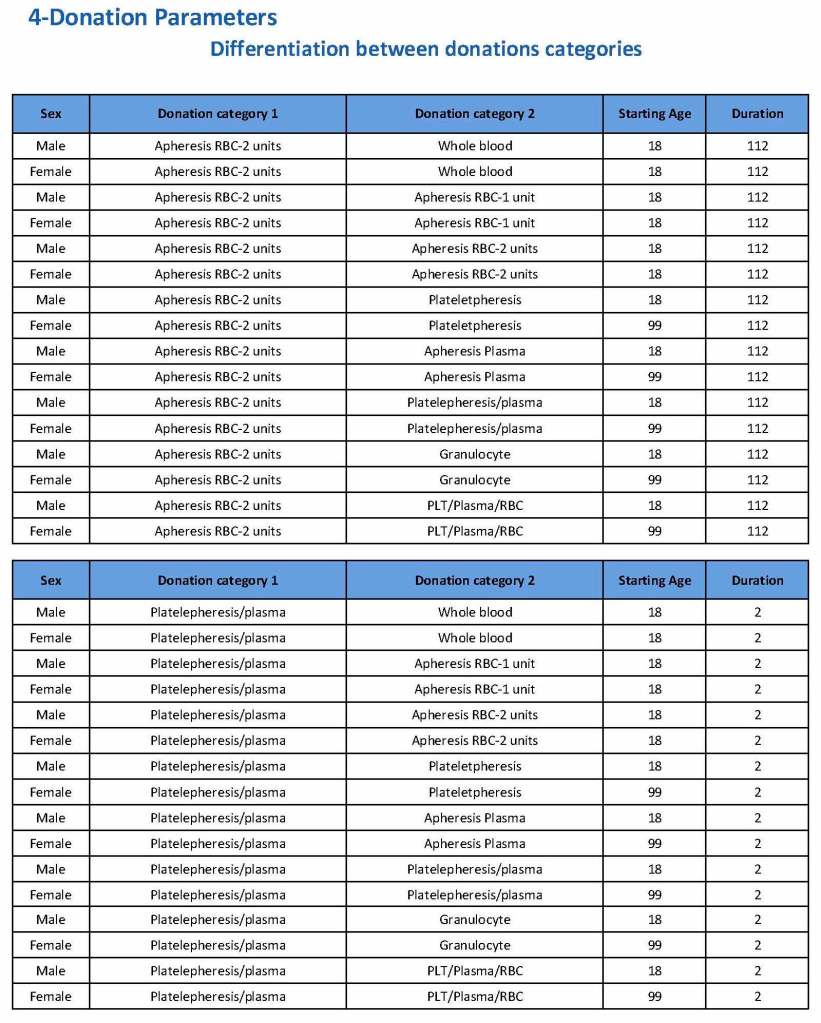
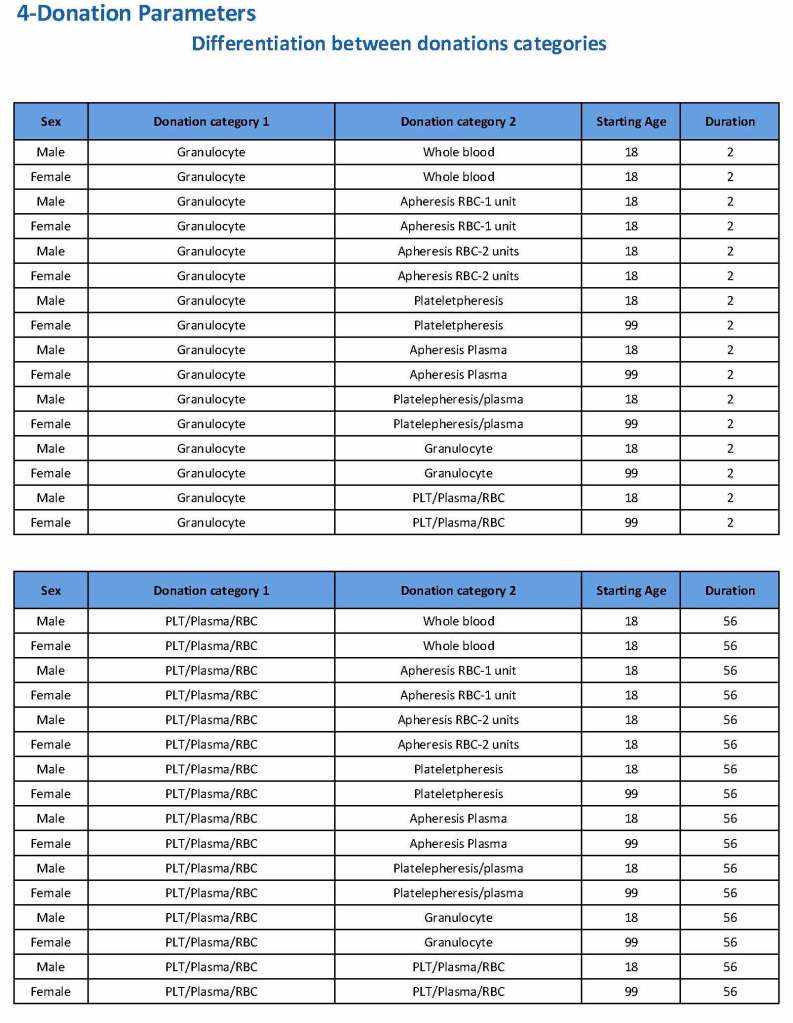
Donation can be whole blood or apheresis-based. The sex and age for each donation type is specified. At HMC, we did not accept females for platelet or plasma donations, so the starting age is listed as 99 years. Otherwise, in accordance with Qatari law, the starting age for donation is 18. All these parameters are user-definable, and a transfusion medicine physician can override the rules if necessary.
For each and every combination of donations, the deferral interval must be specified. Examples follow. The temporary deferral period is in days:
Previous donation whole blood, current donation whole blood: 56
Previous donor platelets, current donation whole blood: 2
Previous donation whole blood, current donation platelets: 56
Also note how for each possible combination there is an entry for male AND female. Females are restricted to whole blood donation and only RBCs will be made from the collection.
If there is a collection incident and the apheresis procedure is not completed, the interval will be set to 56 days. This will be covered in the post on donor adverse effect reporting.
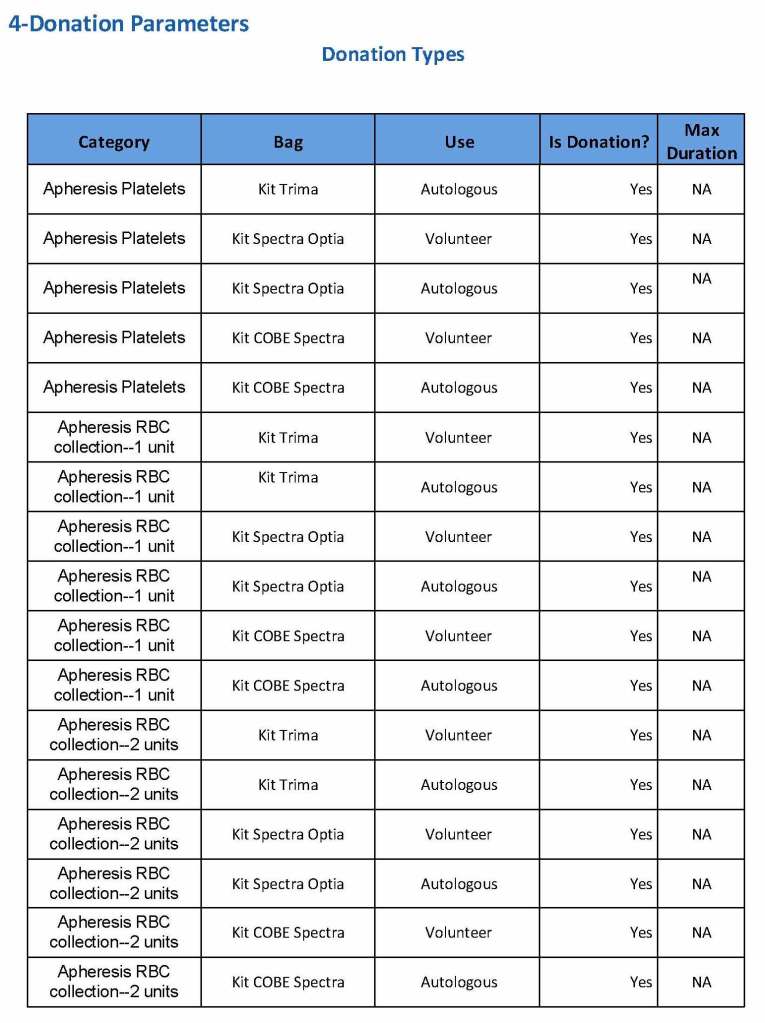
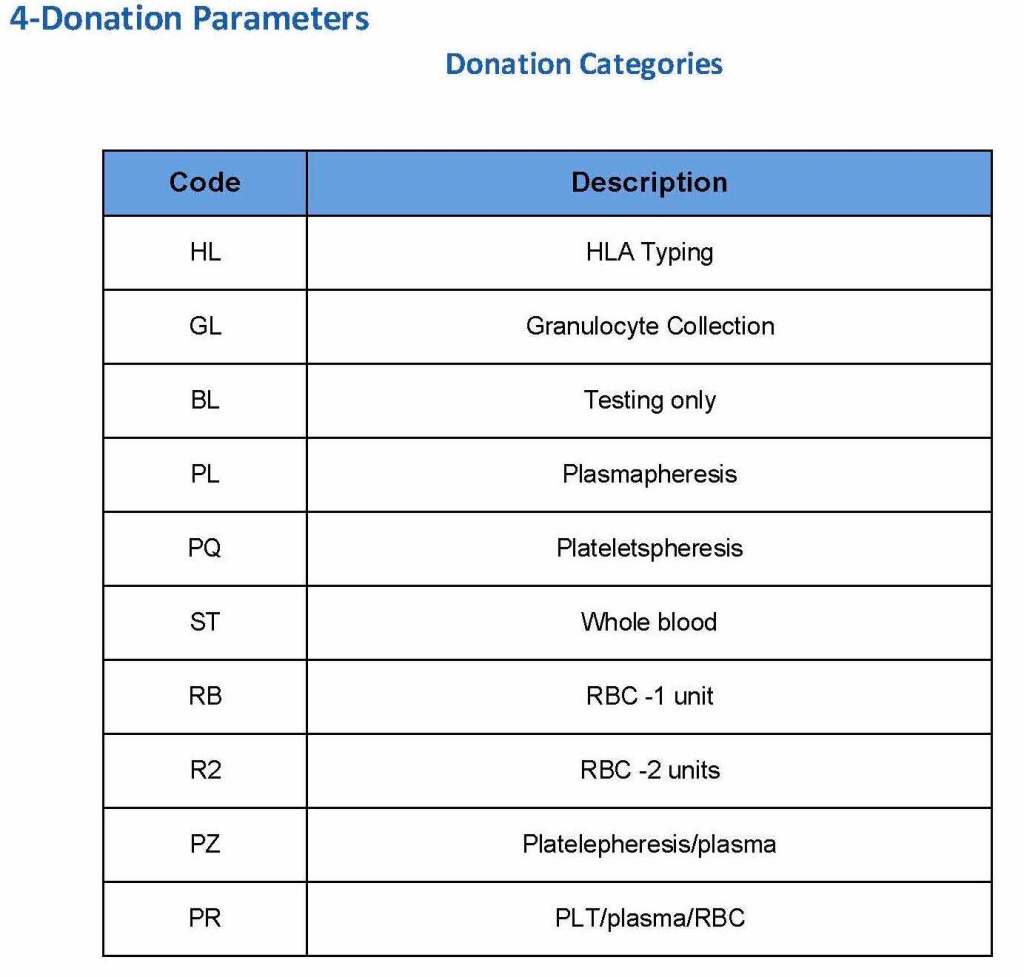
At the time of registration, the type of donation must be specified. In my last position, this could include whole blood for automated Reveos, whole blood for cryoprecipitate, plasmapheresis, COVID 19 convalescent plasmapheresis, plateletpheresis, concurrent platelet and plasmapheresis, concurrent platelet, plasma, and RBC apheresis, RBC apheresis-one unit, and RBC apheresis-2 units.
There is also a specimen-only donation without actual collection that includes database check, assignment of an ISBT specimen number, donor questionnaire, physical examination, and specimen collection only..
We specified which bag or kit could be used for each type of donation so when it was selected, only that bag type would be accepted by Medinfo
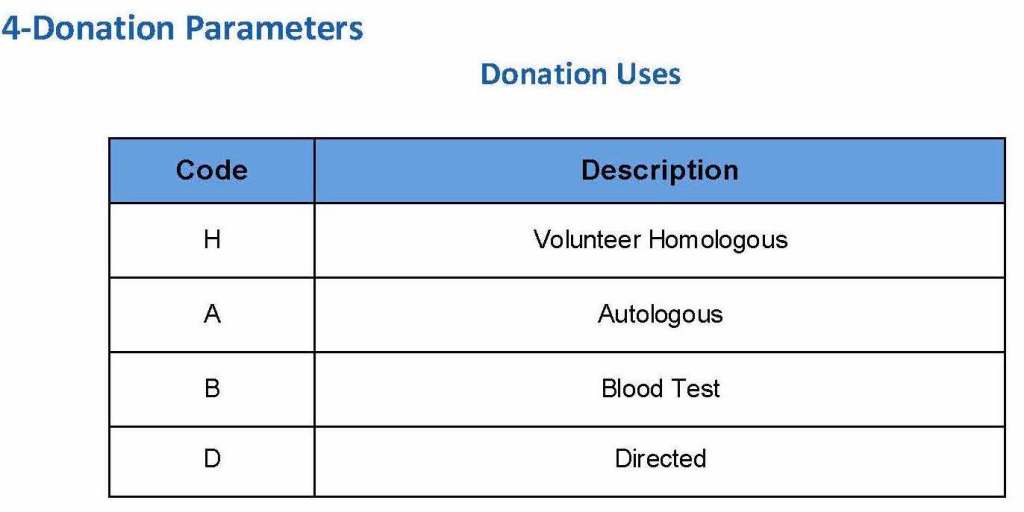
For each of these types we must specify what type of donation is permitted: volunteer, autologous, or directed.
Finally, we must indicate the maximum length of the procedure permitted. This applied to whole blood only and we set this at 15 minutes—this is user definable.
The following are a sample set of parameter settings for the above:
Note how we included contingencies for old bag sets and equipment (that we later discontinued) and for granulocyte collection (which we did not actually perform).
This policy outlines steps taken to minimize the risk of data entry errors and is based on a dualistic approach: review of results by a senior technologist and/or supervisor and various computer safeguards built into the Medinfo Hematos IIG blood bank computer HIIG system. This policy also discusses the verification (here called authorization) and purge processes of HIIG.
Policy:
Review by senior technical, supervisory, or transfusion medical staff:
Designated test procedures require review by a second technologist before authorization.
Complex immunohematology testing and specimens showing aberrant results (e.g. ABO/D discrepancies) are reviewed by the supervisors or designates and ultimately a transfusion medicine physician before authorization.
Computer system HIIG rules:
Privileges:
System restricts which staff can perform specific tests
Patient/donor identity:
System asks end-users to verify patient/donor identity before starting any access to the patient/donor record.
System performs historical database checking and flags any inconsistencies (e.g. historical ABO/D typing differences, etc.)
Testing:
Only selected staff have privileges to authorize or purge.
ABO/D testing algorithms require entry of reactions, not interpretation of results and are compared to a truth table.
Aberrant results require special review before ABO/D typing results can be authorized/purged.
D-controls must be negative to allow D typing results to be authorized for liquid D-typing reagents.
DAT results require appropriate controls to meet truth-table criteria.
Eluates require last wash to be negative before authorization
Blood components:
Selection of RBC or plasma units requires two independent sample determinations within 72 hours of each other.
ABO-incompatible RBC or FFP/FP24 transfusions are not allowed.
Donors with any detectable antibodies are permanently deferred.
Depending on the patient’s antibody history, release of RBC units may require antigen-matched units. Examples:
Mandatory matching (only antigen negative matched units allowed—no antigen positive or antigen-untyped units): Antibodies against H, D, c, K, k, Kpa, Kpb, Jsa, Jsb, Jka, Jkb antigens, anti-PP1Pk
Priority matching (incompatible or untested can be approved by a transfusion medicine physician): C,E, e, Fya, Fyb, M, S, s
Antigen matching not required: Lea, Leb, N
Least-incompatible crossmatch require special authorization to release
Protocols to force irradiation or other modified components can be setup in HIIG.
Donors:
Donor tests have same criteria as the same test used in patient testing for controls, etc.
Donor demographics are read directly from the Ministry of Interior database—no manual entry (bar code only used).
References:
Workflows for Hematos IIG (1001 through 1005), 2013
Standards for Blood Banks and Transfusion Services, Current Edition, AABB, Bethesda, MD, USA
Guidelines to the Preparation, Use, and Quality Assurance of Blood Components, European Committee (Partial Agreement) on Blood Transfusion (CD-P-TS), Current Edition
Building the Software Processes for the Donor Center 2:
Donor Collection and Screening—Registration and Pre-Donation Parameters
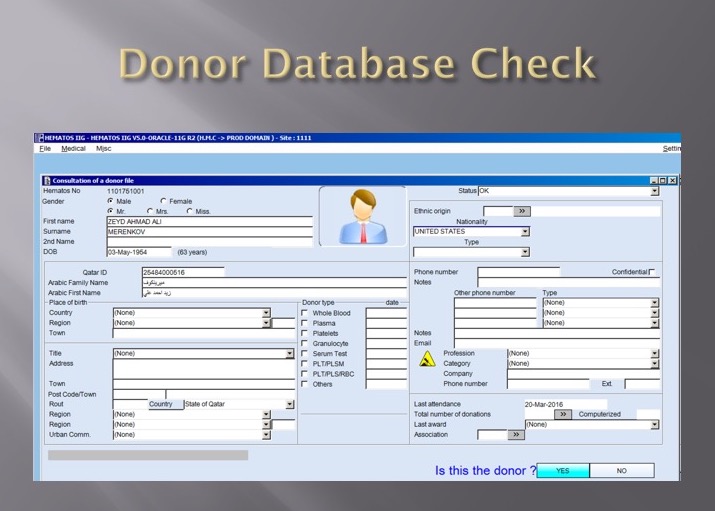
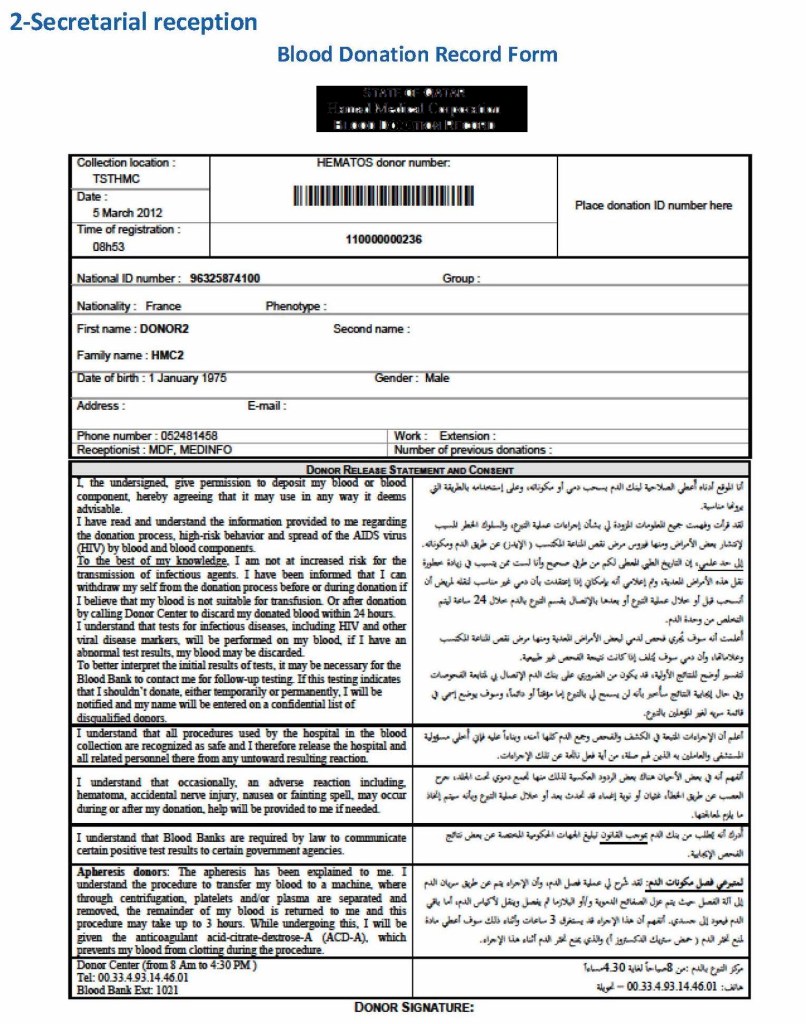
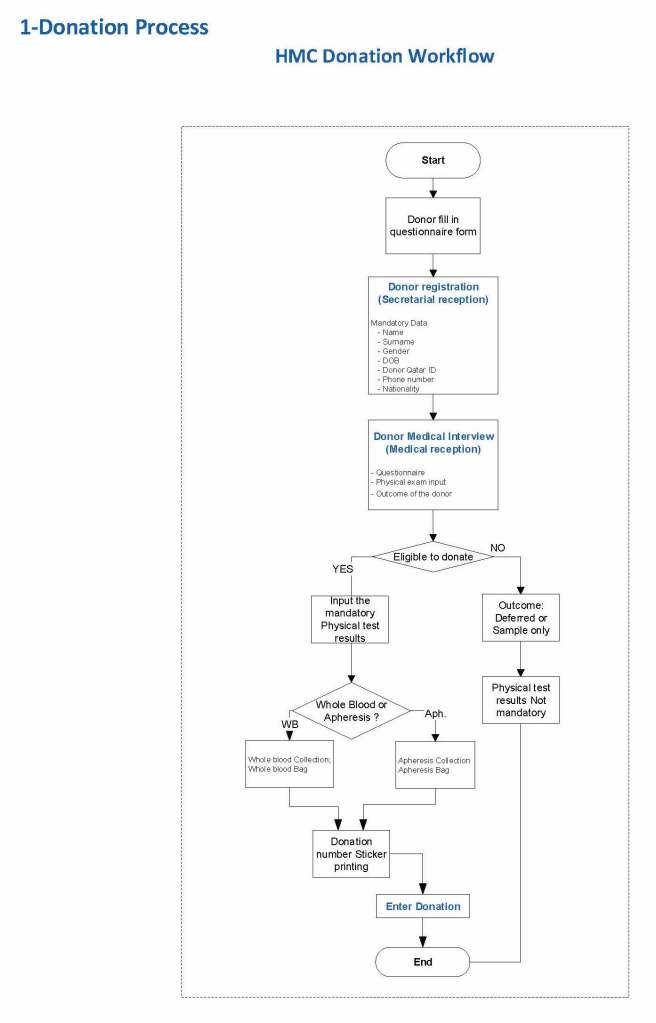
The potential donor enters the collection area. He takes a number and waits to be called. When called, he shows a picture identification card with a unique alphanumeric sequence. This is entered into the donor module software and the system checks the donor deferral database for temporary and/or permanent contraindications. If none are found, a consent form with an ISBT specimen number is generated.
In this post, we will consider:
Registration process in multiple languages
Donor deferral database
Donor consent with generated unique ISBT specimen number
Registration Parameters
Registration:
In the Middle Eastern region, multiple languages are used. Although Arabic may be the main language, not all the registration staff may speak it. English is commonly used as the main work language. The date may be entered as Common Era (Gregorian) and/or Hijri.
An issue is that for native Arabs, the only precise, unambiguous name spelling is in Arabic. English transliterations vary. Example, Muhammad in Arabic is very simple to write, in English it may be rendered as Mohamed, Mohammed, Muhammad, etc. The donor’s name should be recorded exactly as in his native alphabet. How do you register when the staff do not speak or type Arabic?
Fortunately, I have worked with software that is in UNICODE, meaning that the data does not have to be restricted to English or Latin script (I wonder why the hospital information system we had at one institution could be sold in the Middle East and not have this capability!). That means one could perform registration and donor questionnaire tasks in multiple languages, and preferable the native language of the donor. One could even prepare database reports in Arabic.
Medinfo had an elegant solution to the registration process in Qatar. It read the local identity card’s barcode issued by the Ministry of Interior and accessed (read-only) the demographic data on that donor and received back both the English and Arabic name fields:
This would generate the demographic fields in the registration:
The blood bank software would check the national donor deferral database and list any deferrals/contraindications to donation and the next eligibility date. It would also list what type of donations were permitted (e.g. for females, only RBCs could be collected and processed: if a whole blood unit was collected, then the platelets and plasma would NOT be permitted to be processed and were discarded.)
Medinfo used a unique key field, the Medinfo Hematos Donor ID for the database. This was not the same as the national ID card. All records were indexed against this number with strong security.
Donor Deferral Database:
Medinfo had already imported donor data from a previous computer system and added this to its own database. Thus, there was only one database to check. The database listed all previous donations: dates, type, status (complete, aborted). Any contraindications would be prominently shown in RED.
Donor Consent and Assignment of Donor Unit (ISBT Specimen) Number:
If there were no contraindications, Medinfo generated a donor consent in English and Arabic and the unique donor unit number for the current encounter:
Registration Parameters:
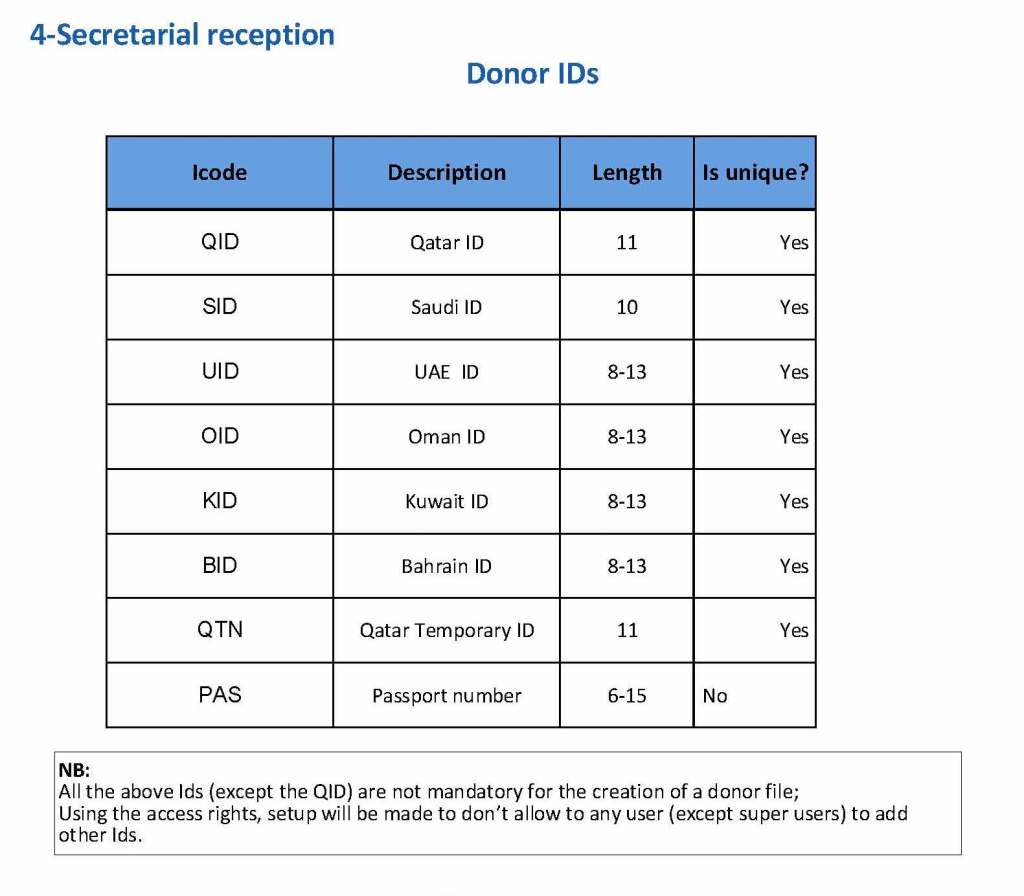
Medinfo enforced registration according to the format of the identity card. The donor ID format was built into Medinfo. If the entry deviated from this, it was rejected and registration could not continue:
The registration type would be selected (volunteer, autologous, directed, or paid). In Qatar, paid donations were not permitted:
Next, the donation type had to be selected:
At the time of registration, the type of collection bag (or kit if using Reveos) was automatically set in Medinfo. I will consider this further in the next post of this series to determine eligibility based on the previous donation interval and type.
At each donation site, the allowable types of donations and kits could be set. Based on the donation parameters above, staff could not select the wrong type of bag/kit (e.g. an apheresis kit for a mobile donation).
If there is strong antibody binding to an RBC, this may interfere with a typing reagent attaching to the cell and cause a false-negative, i.e. a “blocking” antibody. Such cells may interfere with the indirect antiglobulin test IAT, i.e. the antibody screen. The autocontrol and direct antiglobulin test DAT will be strongly positive.
The manufacturer’s instructions should be strictly followed for using its reagents in the presence of a strongly positive DAT. If there is no reaction with the typing reagent, the result must be indeterminate.
One could try a (relatively) nondestructive elution method such as gentle-heat elution to remove some of the antibody and then retype the cells. I have found this to be a simple and effective method for my staff to use. Just remember that despite being “gentle,” there will still be some hemolysis present, but here it is the cells we are trying to save.
Usually, we find this situation in a neonate born of a mother with anti-D. The baby has a strong DAT but the D typing is negative. Check the D control carefully: if it is positive, the result is indeterminate, try another method. Usually gel/glass bead methods are subject to less interference. Finally, there is always the classic saline anti-D!
In Medinfo software with a blocking antibody, a nonnegative control will trigger a manual review of the results. There will be no automatic release.
Here is my process for handling blocking antibodies, which I set up for HMC Doha:
INTERIM POLICY: ANTIGEN TYPINGS IN PRESENCE OF STRONGLY POSITIVE DIRECT ANTIGLOBULIN TEST (DAT): RULE OUT BLOCKING ANTIBODY
Principle:
Antigen typing of cells with large amounts of coating antibody (i.e. strongly positive DAT 3-4+) may not always be possible because the bound antibody may block available antigen sites. This policy is to clarify how to recognize and handle such situations.
Policy:
Always follow the manufacturer’s instructions for the use of the typing reagent.
In particular, note whether a control must be run with the test (e.g. D-control, D-diluent, etc.) or if it is included in the gel or glass bead card.
If a control is required, use exactly what the manufacturer recommends.
DO NOT SUBSTITUTE ANYTHING ELSE AS THE CONTROL!!
Interpret the reactions exactly as the manufacturer indicates.
If the test is invalid because of the control or any other reason, report the antigen typing as indeterminate and send for Transfusion Medicine Physician review.
If the DAT is 3-4+ and the antigen typing shows no reaction (apparent negative), send the case to the Transfusion Medicine Physician for review and final interpretation. DO NOT ENTER THE RESULT AS NEGATIVE UNLESS THE TMP INSTRUCTS YOU TO DO THIS!!
To rule out a blocking antibody, a special elution to gently remove the coating antibody may be needed so that the RBCs can then be typed (not acid glycine technique—rather, gentle heat elution.) The Transfusion Medicine Physician will decide whether to do this additional testing.
References:
Standards for Blood Banks and Transfusion Services, Current Edition, AABB, Bethesda, MD, USA
Technical Manual, Current Edition, AABB, Bethesda, MD, USA
Guidelines to the Preparation, Use, and Quality Assurance of Blood Components, European Committee (Partial Agreement) on Blood Transfusion (CD-P-TS), Current Edition
This is a first is a series of detailed posts of how I collaborated with Medinfo (Nice, France) to build customized donor software for both Saudi National Guard Health Services and Hamad Medical Corporation Doha.
In particular, we were using a non-turnkey software which could be built to order. If we didn’t know what we were currently doing, how could we build something better?
At both sites, we had good manual systems in effect and prepared detailed mapping of the current state. We reviewed our variance reports to see where we needed to bolster the system and improve the critical control points.
We studied the software options and prepared a draft Medinfo future state from which we started to build the system. We did this in small stages so we could test it and adjust our settings as needed—without being charged extra (unlike a general laboratory software I had been working with at the same time, which always charged an arm and a leg).
To do this, I engaged early a team of my most computer-literate staff to work as Super Users. In the Donor Center, this consisted of nurses and technologists.
I resigned from HMC on 16/4/20. Here are a set of my major accomplishments during that period. None of my work after this date has any relationship to HMC.
2011
Established automated component production using Atreus technology, plasma and platelet pathogen inactivation (Mirasol)—made HMC component production Good Manufacturing System GMP compliant
Adopted non-PCR-based NAT technology (Grifols/Novartis Tigress) and Qatar becomes world reference site for this
Based on the above, Qatar can now completely process all whole blood into blood components (red cells, platelets, and plasma) in as little as 5 hours from collection!
2011-2020:
Prepared policies and procedures for the hospital blood banks/transfusion services, blood donor center, therapeutic apheresis, and laboratory information systems to bring HMC in compliance with the Council of Europe, international AABB, and other standards. I customized our own standards for our local needs based on them.
2012-2013
Implemented custom build of the multilingual blood bank computer system (Medinfo) for both patient and donor services, including development of interfaces to all production equipment including Atreus and Mirasol (world’s first) and a direct link to Ministry of the Interior to obtain patient demographics in English and Arabic—Qatar became the world’s first site to combine fully-interfaced, automated component production with pathogen inactivation: Qatar becomes world reference site for this.
2013-2014
Built, validated, and implemented laboratory build of hospital information system, Cerner Millennium
2015
Replaced and updated Atreus with Reveos automated component production to allow faster throughput and capacity with a full bidirectional interface (world’s first), introduced platelet-additive solution PAS with pathogen inactivation (Mirasol)—Medinfo interfaces updated to Reveos for all equipment: this doubles the capacity to process whole blood into components using the same physical space
2015-2019
Updated dedicated blood bank software Medinfo Hematos IIG by several versions using Division Head, LIS, and internally trained Super Users—at great cost savings to HMC by not using outside consultants (e.g. Dell Consulting)
2019
Established column absorption technology using Terumo Optia therapeutic apheresis machine for treatment of ABO-incompatible renal transplants: I validated using the Ortho Vision MAX to perform ABO antibody titers for this system and correlated it with the reference method at Karolinska Institutet in Stockholm (manual gel) to bring rapid throughput and labor savings—Qatar being the first-site in the world to do this. We saved money by using the same apheresis machine to use this column absorption technology (no need for second machine to use the columns)
2020
Expedited setup (two weeks total) of COVID-19 convalescent plasma production, initially manual and then fully integrated into the Medinfo computer system as a customized module with separate quarantine collection, production, and transfusion service functions
Other:
I was awarded two HMC Star of Excellence Awards:
2013—Liver Transplantation Transfusion Support
2019—ABO-Incompatible Renal Transplantation Support
The following was my process at HMC Doha for TRALI/TACO. It includes proactive measures to minimize the risk of TACO and the procedure for surveillance and workup of such cases.
In the Medinfo blood bank computer system, we did not prepare plasma or platelets from female donors. If approved by a transfusion medicine physician, a manual override was made in exceptional cases (e.g. mother donating platelets for her child in neonatal alloimmune thrombocytopenia cases.). In some other countries, they do HLA antibody testing to allow females to donate platelets.
I emphasize that the diagnosis of TRALI and/or TACO is clinical, but the transfusion medicine physicians must always consider the possibility whenever there is an adverse effect associated with progressive respiratory distress.
Principle:
Since TACO and TRALI are major causes of serious adverse effects from transfusions, this policy outlines actions being pro-actively taken to mitigate the risks in Transfusion Medicine. TACO and TRALI may be difficult to distinguish so this policy addresses both.
Objectives:
Implement measures to minimize TRALI and TACO
Track cases of transfusion-associated acute lung injury TRALI and TACO
Develop algorithms for suspected cases of TRALI and TACO
Tracking:
All transfusion reactions are reviewed by the Division Head, Transfusion Medicine or his designee on a STAT basis, 24 hours a day, 7 days a week
Any reactions with respiratory distress are reported as “rule-out TRALI/TAC” to the clinician
All transfusion reactions are recorded in Medinfo HIIG for tracking and reporting.
Risk Management:
Female blood donors routinely are only used for making RBC components (i.e. not for FFP, cryoprecipitate, or platelets).
RBCs are in additive solution SAGM so only 35 ml residual plasma is present per unit.
All platelet components are in platelet additive solution with only 35 ml residual plasma per component.
All platelets and plasma are pathogen-inactivated which may reduce the risk of TRALI.
If the female has a rare phenotype (e.g. IgA deficient, rare platelet antigen typing) she will only be considered for a directed donation of platelets or FFP/cryoprecipitate for that special-needs patient if she does not have HLA antibodies (anti-human-neutrophil antibody testing to be implemented in such cases when it is available on-site).
Solvent-detergent treated plasma SDP is available for patients with a confirmed or suspected history of TRALI.
All cellular components are leukodepleted (< 1E6 residual WBCs/component as per CE Standards) in the blood bank at the time of production.
Blood bank computer system Medinfo Hematos IIG limits the number of components released at any one time (excluding emergencies).
Notifications:
Transfusion Medicine TM will notify the outside blood supplier of any units implicated or associated with TRALI.
A transfusion medicine physician will notify the most responsible physician of any workup results suggesting the possibility of TRALI/TACO.
TM will notify all donors of their disqualification from blood donation based on the following algorithm.
Algorithm for Diagnosis and Management of Donors:
Evaluation of the Donor and Recipient in Suspected TRALI:
The medical technologist will process all transfusion reactions as STAT and immediately contact the TMS Director or physician designate with the results.
The medical technologist will convey information to the TMS Director or designate about ALL blood components issued recently, especially in the last 6 hours prior to the event.
The TMS Director or designate will specifically check if there is evidence of respiratory distress listed on the transfusion reaction investigation form. If so, he will contact the responsible clinician immediately for further assessment.
If the signs and symptoms suggest ALI (see Table 1 above), the TMS Director or designate will inquiry about the left atrial pressure to rule out left-sided heart failure as a cause for the pulmonary edema.
Based on the clinical information, the TMS Director or designate may elect to order any or all of the following tests if available:
Quarantine all remaining components from possibly implicated/associated donor(s) while the workup is in progress.
Recipient HLA, platelet, and/or granulocyte antibody screen, or a crossmatch between recipient plasma/serum and donor leukocytes
Donor HLA and/or platelet antibody screen, granulocyte antibody screen, crossmatch donor plasma/serum and recipient leukocytes, inter-donor crossmatch between plasma/serum of one and leukocytes of another donor.
The usual algorithm to be followed is as follows:
Consult patient medical record and clinical care physician to determine if the diagnosis of TRALI is likely.
Check all components transfused within 6 hours prior to the onset of symptoms.’
Immediately quarantine other components from the same donations and contact outside blood suppliers if indicated.
Obtain donor antibody testing of only highly suspect cases, based on the clinical manifestation and initial diagnostic tests:
If multiple units transfused within hours, only investigate components donated by multiparous females and/or last two units transfused.
First test for presence of HLA class I and class II antibodies in donor components.
If antibody positive, HLA type recipient’s lymphocytes to detect corresponding antigen or perform crossmatch with donor plasma and recipient lymphocytes.
If HLA antibody negative, proceed with neutrophil-specific antibody testing of donor plasma.
If matching antigen-antibody identified or if positive crossmatch, defer implicated donor immediately.
If no such concordance found or if crossmatch is negative, donor eligible to continue donating.
If no antibodies found in donor plasma, test recipient plasma for antibodies to HLA class I and II antigens:
If recipient antibody positive, HLA type donor’s lymphocytes to detect corresponding antigen or perform crossmatch with recipient plasma and donor lymphocytes.
If recipient HLA antibody negative, proceed with neutrophil-specific antibody testing of recipient plasma
Donor Disposition:
For donors implicated in TRALI or associated with multiple events of TRALI, one or more of the following options may be selected at the discretion of the Head, Transfusion Medicine or designate:
Defer donor from donation
Divert plasma for fractionation or discard plasma from future whole blood donations from that Blood and Apheresis Donor Main Questionnaire
Manufacture no platelet or plasma components from that donor
Wash or freeze/deglycerolize RBCs from that donor
Permanently defer the donor from future plasmapheresis or plateletpheresis donations
Evaluate the previous donations from that Blood and Apheresis Donor Main Questionnaire Avoid giving the same recipient future transfusions from the same donor implicated in TRALI
If the implicated unit(s) are from another facility, that blood center should be notified to initiate a workup for possible TRALI in the donor.
Interpretation:
The diagnosis of TRALI is not clear-cut:
The AABB interim standard does not apply. It is at the discretion of the TMS Director or designate whether to conduct donor assessments.
The donor is associated with a single event of TRALI:
This applies where the diagnosis of TRALI has been established based on clinical and radiographic findings:
Each donor from each and every component associated with TRALI must be identified and traced.
Co-components from the current donation and components from previous donations should be evaluated for recipient complications.
The donors medical history should be evaluated for previous pregnancies, transfusions or other events that may have resulted in antibody development.
Based on the results of this investigation, the Head, Transfusion Medicine or designate should decide:
Whether to perform laboratory testing
Whether to discard the remaining blood components from the donor
Whether to allow or indefinitely defer the donor
The donor is associated with multiple events of TRALI:
This applies where the diagnosis of TRALI has been established based on clinical and radiographic findings:
Each donor from each and every component associated with TRALI must be identified and traced.
Co-components from the current donation and components from previous donations should be evaluated for recipient complications.
The donors medical history should be evaluated for previous pregnancies, transfusions or other events that may have resulted in antibody development.
Based on the results of this investigation, the TMS Director or designate should decide:
Whether to perform laboratory testing
Whether to discard the remaining blood components from the donor
Whether to allow or indefinitely defer the donor
Triage based on laboratory testing for TRALI:
The donor associated with TRALI is antibody-negative:
The donor may continue to donate.
The donor associated with TRALI is antibody-positive but the specificity is NOT directed against a recipient antigen by either antigen typing or crossmatching (i.e. the donor is NOT implicated in TRALI—see definition above):
Indefinitely defer the donor from all donations OR
Allow donation of washed/frozen-deglycerolized RBCs only
The donor is implicated in TRALI (see definition above):
Indefinitely defer the donor from all donations OR
Allow donation of washed/frozen-deglycerolized RBCs only
The recipient has antibodies implicated in TRALI (determined by crossmatch or antibodies directed against specific HLA class I, HLA class 2, and/or human neutrophil antigens):
The recipient must receive leukodepleted blood components
TACO
TACO is due to cardiac overload. Our mitigations are to restrict release of the number of components outside emergency events.
References:
AABB Association Bulletin 14-02, TRALI, Bethesda, MD, USA
Han Y. and Goldfinger D., Transfusion Medicine TM 07-5 (TM-297) Checksample, American Society for Clinical Pathology, Chicago, IL, USA. July 2007
Goldman M, Webert, KE, Arnold DM, et al., Transfusion Med Rev 2005; 19:2-31.
Fung YL, Goodison KA, Wong JK, Minchinton RM., Investigating Transfusion-Related Acute Lung Injury (TRALI), Intern Med J. 2003 Jul;33(7):286-90.
Standards for Blood Banks and Transfusion Services, Current Edition, AABB, Bethesda, MD, USA
AABB Association Bulletin #05-09, Transfusion-Associated Acute Lung Injury, 11/8/05
AABB Association Bulletin #05-04, Proposed Interim Standard for Deferral of Donors Implicated in TRALI, 9/3/05.
TRM.42110, CAP Transfusion Medicine Checklist, 15/6/09