This is a review/update of this document prepared early in the course of our COVID-19 Convalescent Plasma CCP collections. It now includes testing of specimens not only for donor marker testing but also COVID-19 antibody titers.
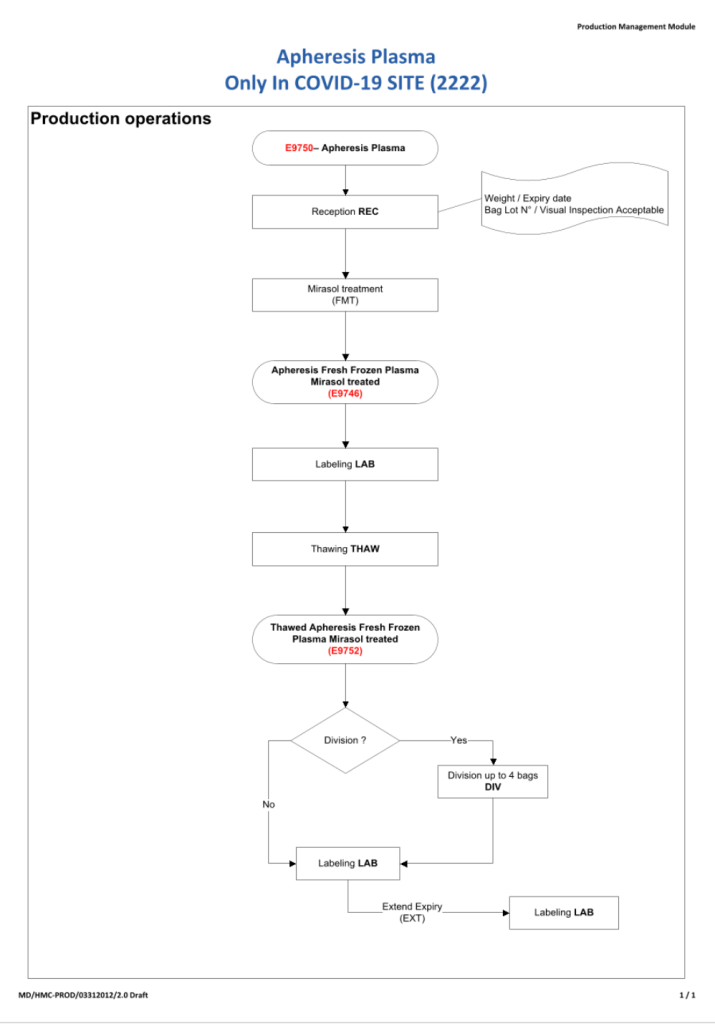
All blood components are considered medications and are subject to Good Manufacturing Practices as mandated by international accreditation standards. The whole process must be done reproducibly and precisely by specific personnel trained and documented to be competent. This includes collection of convalescent COVID-19 plasma.
Transfusion Medicine will provide staff who are deemed competent for the entire process of the collection, manufacture, and release of this unlicensed, emergency-contingency component.
It will help greatly if all candidates are prescreened to exclude the following candidates:
- Administrative:
- Donors must come with a valid Qatari identity card: no ID means no screening
- Sex:
- Males only to minimize the risk for transfusion-associated lung injury TRALI
- Donor Feeling:
- If the donor does not feel well, he should not come for screening/collection.
- Food/Drink:
- Donor must have eaten/drunk fluids within 4 hours of arrival for screening/collection.
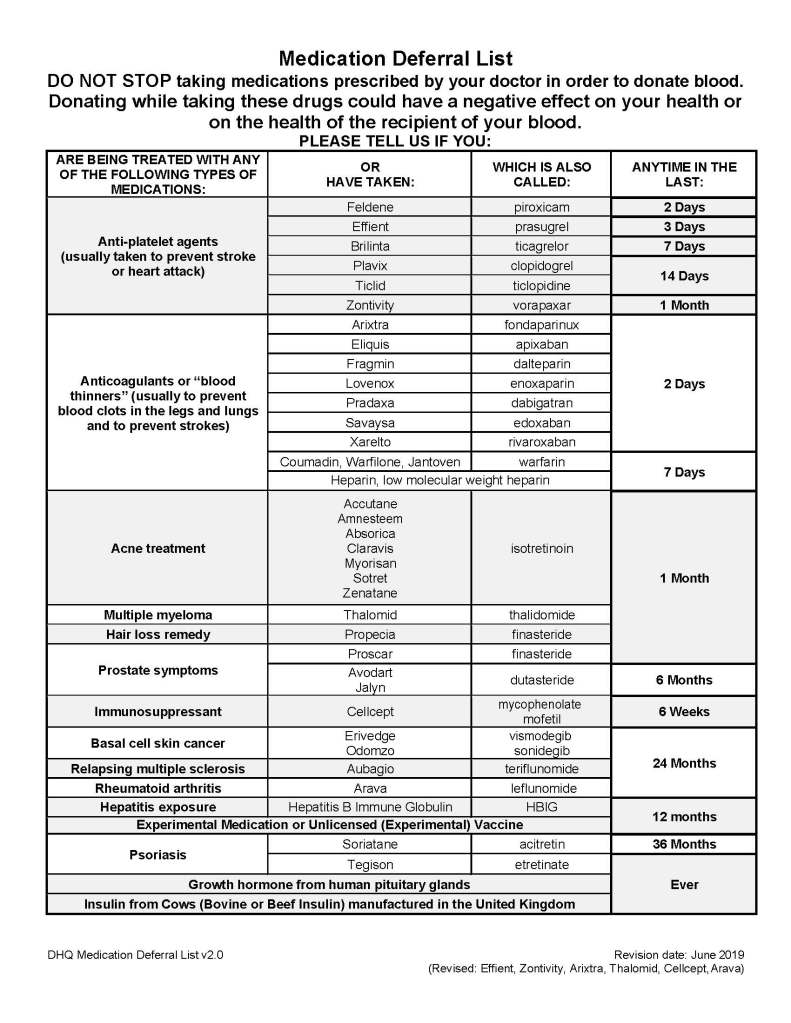
- Medication exclusions:
- Antibiotics within the past 14 days
- ACE inhibitors in the past 48 hours
- Beta blockers
- Anticoagulants
- Anti-anxiety or other psychotropic medications
- Other medications on the Unified Donor Questionnaire Deferral List
- Medical exclusions:
- Stable vital signs
- History of seizures
- History of dementia or other chronic neurologic disorder
- Family history of dementia or other chronic neurologic disorder
- Significant cardiac arrhythmias
- History of hepatitis B, hepatitis C, HIV, brucellosis, Ebola
- Travel history:
- 5 years cumulative residence in Europe including Ireland and France 1980-2001
- 3 months cumulative residence in the UK (and/or all its territories) 1980-1996
- Any visit(s) to West Africa
- Testing:
- Antibody titers should be performed to exclude candidates with low-titer or absence of antibodies.
- Regular donor marker testing (excluding malaria and HTLV 1/2)
All processes will continue to be performed in the dedicated blood bank computer system. The COVID-19 antibody titers will be part of the donation record.
This is NOT a complete list of criteria. Transfusion Medicine personnel will screen according to the full donor criteria. Thus, donors passing the pre-screening may still be otherwise disqualified based on the detailed process.
8/11/20