This is a presentation I made at the Saudi MOH many years ago, but it is still good for teaching purposes. I am dividing it into multiple parts because of its size.
To Be Continued:
11/8/20
Includes compatibility testing (AHG, electronic, immediate-spin), antigen typing, antibody screening and identification, direct antiglobulin testing, elution, transfusion reaction and drug reaction workups, component typing tests upon receipt in hospital blood bank, release and return of components
This is a presentation I made at the Saudi MOH many years ago, but it is still good for teaching purposes. I am dividing it into multiple parts because of its size.
To Be Continued:
11/8/20
Transfusion Medicine includes laboratory and non-laboratory functions. The non-laboratory and purely clinical functions are unique and have no analogy within the general laboratory.
The transfusion service/hospital blood bank laboratory is the closest to a laboratory operation, but there is component modification and complex manual testing, especially for reference immunohematology testing. The staff must make detailed manual decisions, the errors for which could be life-threatening for the patient.
The blood donor center manufactures a pharmaceutical, i.e. blood components with collection, donor qualification, donor abnormal results review, infectious disease marker testing, component production, and donor immunohematology testing—all subject to Good Manufacturing Practices. Never forget: Blood is a drug!!
No other laboratory section is directly responsible for treatment of critically ill patients. Therapeutic apheresis is essential for organ and stem-cell transplants, nephrology, neurology, etc. No other laboratory section is directly responsible for treatment of critically ill patients. Transfusion Medicine physicians are functioning as intensivists. There is no hiding in the laboratory from clinical medicine.
There may also be an industrial manufacturing plant to extract various blood derivatives (e.g. factor concentrates, albumin, Rh immune globulin, etc.) This is pharmaceutical manufacturing on a large-scale basis. There is medical, technical, and special administrative expertise.
Many functions may operate 24/7. The transfusion medicine physician may be on-call for donor issues and review of complex immunohematology problems to acutely decide which blood component (and phenotype) should be given as well as review all adverse reactions to transfusion.
The unique blend of clinical skills is unlike anything else in the laboratory. Also, those outside the blood bank rarely have the skills or judgments for the best course of action for transfusion medicine or for its operations.
The clinical transfusion medicine physician must make acute, life-threatening decisions unlike anyone else in the laboratory. The blood bank technologist is at the cutting edge of the battle with his testing and interpretations. No other area of the laboratory is at such risk for injuring or even killing the patient. There is high stress and burn-out.
I have talked with many blood bankers and many seem to share the exasperation that the laboratory does not understand us. The latter looks at blood bank testing like that coming off a hematology or chemistry analyzer—although patients rarely would have severe morbidity or mortality like the blood bank from errors in those analyzers.
No laboratory pathologist has the pressure of the blood bank physician on-call. It really is 24/7 and requires a broad, clinical background to make the right decisions. It is very stressful and does not permit a good night’s sleep.
Thus, I make my case to separate us from the laboratory. We can form our own more effective administrative organization and optimize our own planning. Regretfully, I have never worked in such an administrative structure. I also am a realist that cost-containment nowadays makes it much less likely high administration would permit this change for a mere cost center. This will probably never happen during my career.
Finally, Transfusion Medicine is an essential service. Blood components are essential drugs. The operations and staff must be free of political influences. This is a service for the entire region or country like the fire department, civil defense, etc.
8/8/20
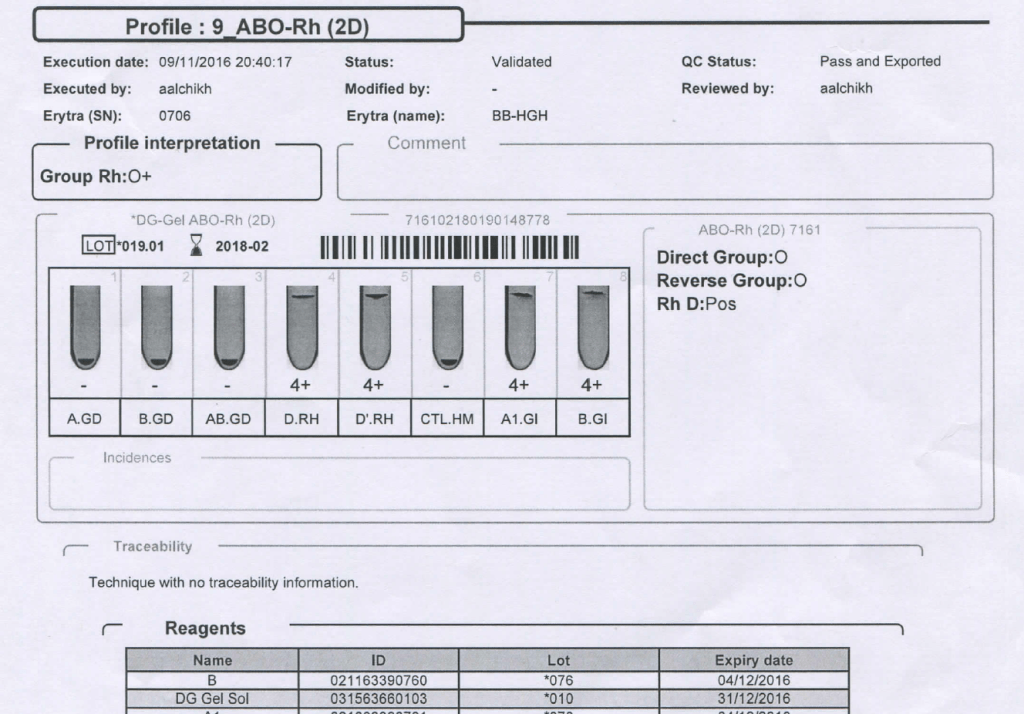
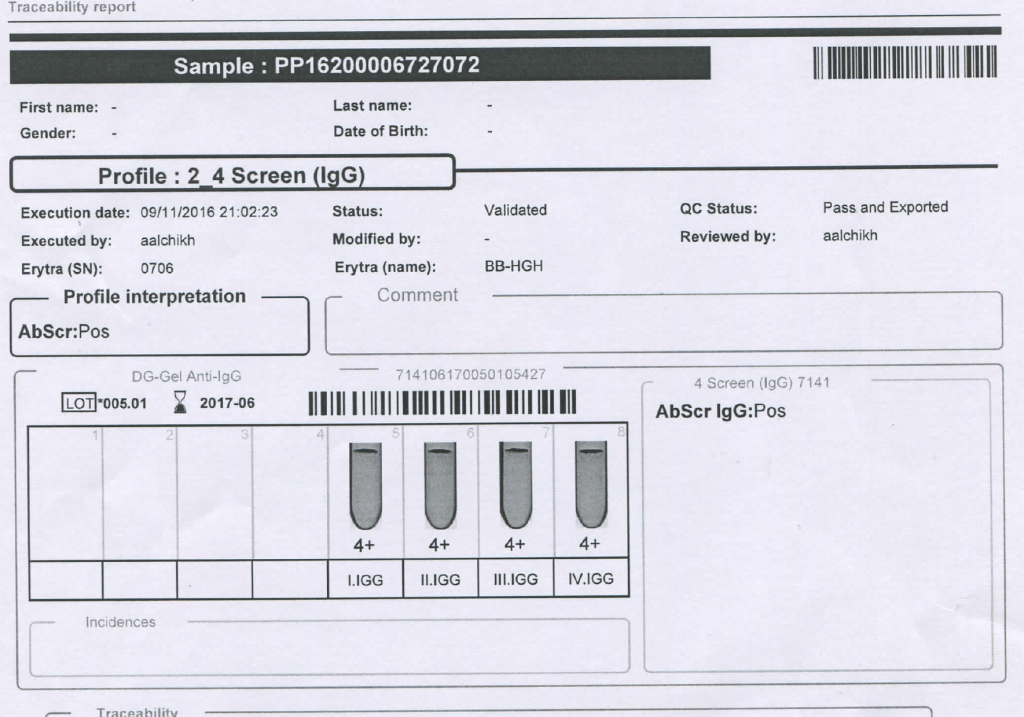
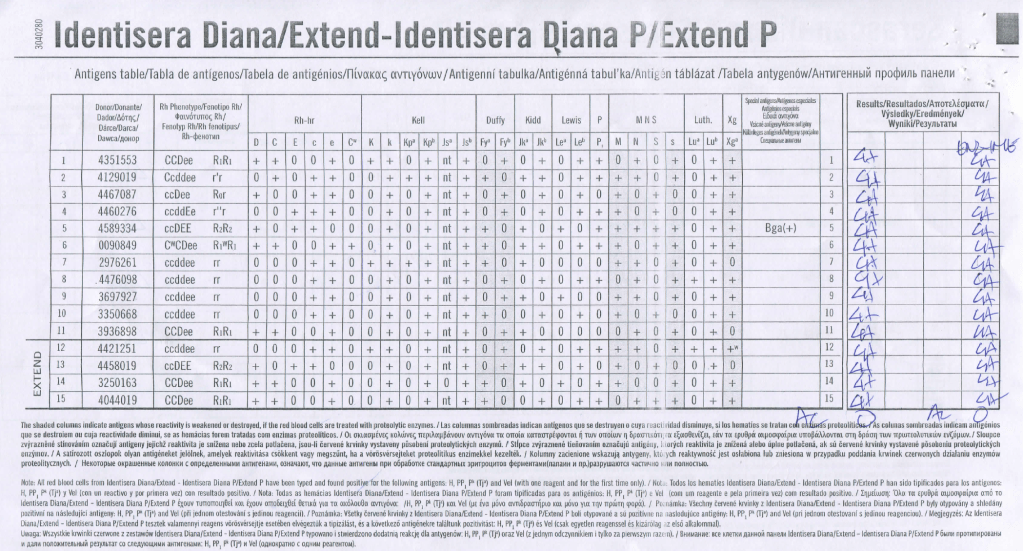
We had a mother (R1R1 K-neg) from Tamil Nadu who had several visits to our hospital. Anti-H lectin was negative. Here is a summary of her workup:
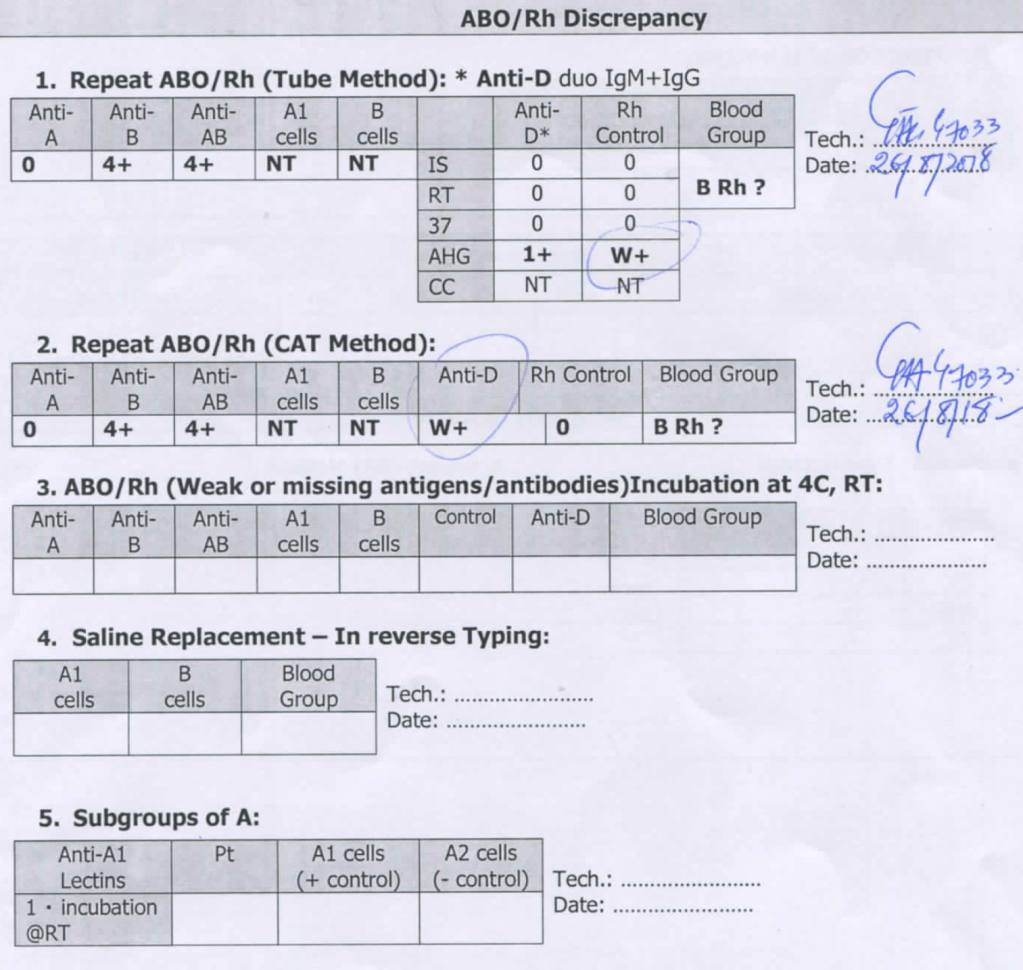
Mother’s ABO/D Typing:
Mother’s Antibody Screen:
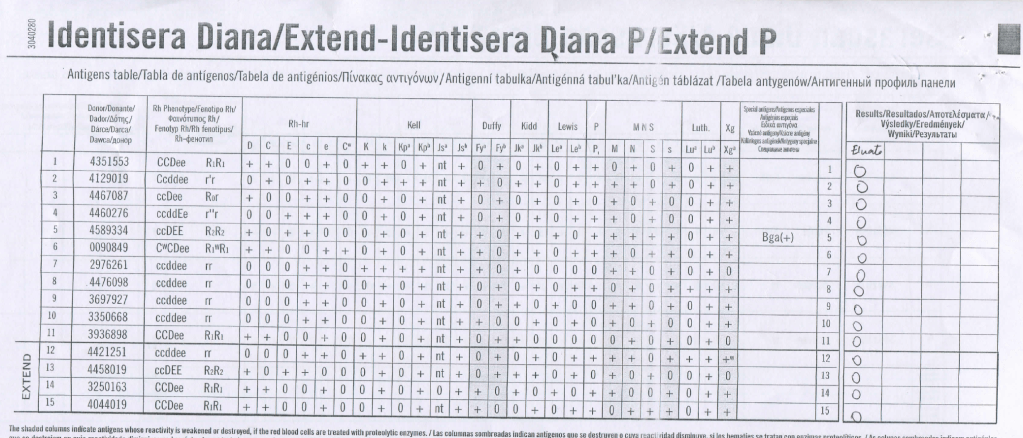
Mother’s Antibody Identification:
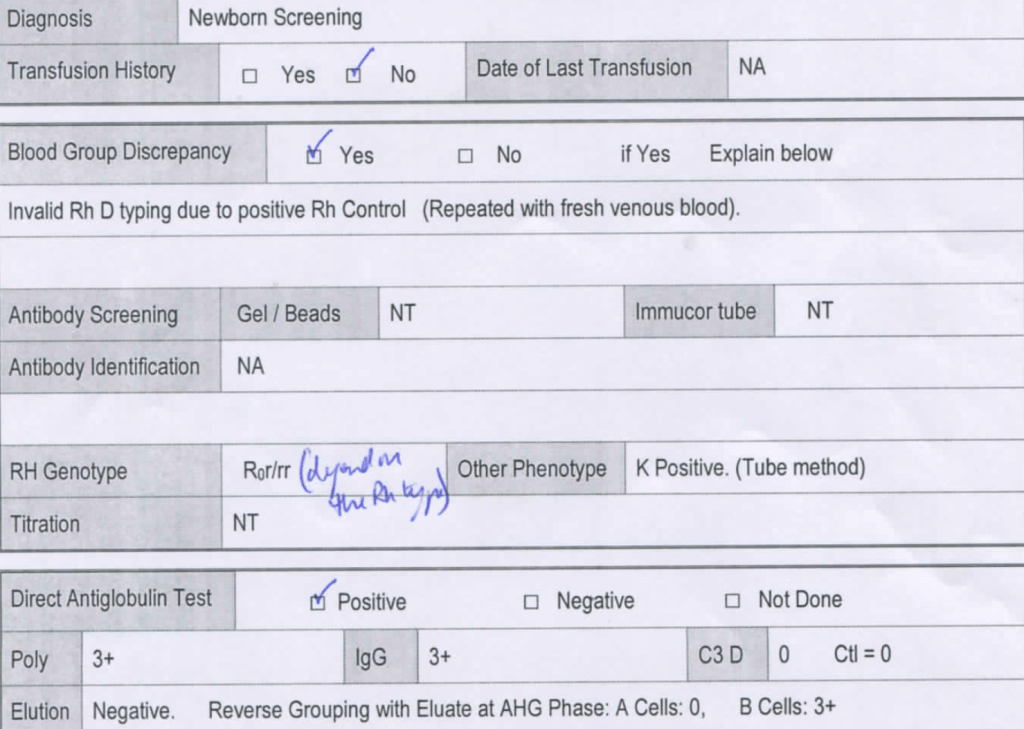
She gave birth to a baby girl, group B, R1R1 K-neg. This is the neonate’s workup:
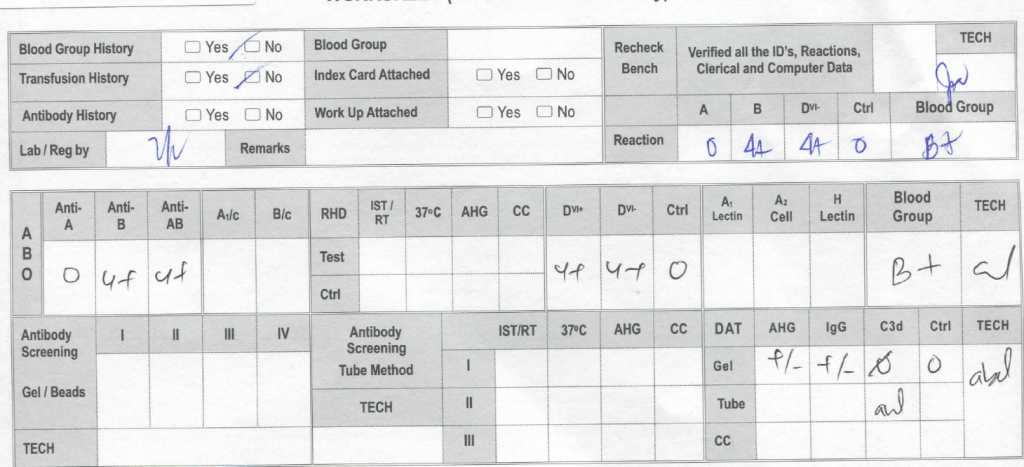
Despite the weakly positive IgG DAT, the eluate was negative. The neonate was asymptomatic.
Anti-H is mainly an IgM antibody and does not cross the placenta, thus no HDFN was noted.
6/8/20
I have had many medical students, residents, and fellows rotate through my Transfusion Medicine department. Hardly anyone has had any interest in making my discipline his/her career. It is a required rotation or an “easy” rotation during which the trainee may take his vacation. The trainee will cram for the examination and then promptly forget it.
I left practice in the USA in 1990, in what I consider the golden age of laboratory medicine. We had supervisors for each laboratory section. In the blood bank, we had many staff with SBBs or who were SBB students. We were very self-sufficient in handling immunohematology problems except for rare blood types or antibodies to high incidence/prevalence antigens.
When I returned to visit my old laboratory. I sensed a deprofessionalization of the laboratory and blood bank in particular. Blood Bank now is a cost center, not an area of revenue. Why hire experienced blood bankers for most hospitals? Send the antibody workups to the Blood Center. There are limited jobs for transfusion medicine consultants. Minimize testing, don’t do extended antigen typings, etc.
Nowadays, I feel like one of the dinosaurs marching into oblivion as in Walt Disney’s Fantasia film, the section called The Rite of Spring. Who will replace those of us retiring? Have you ever noted the average age of attendees at the AABB annual convention? I feel young when I go there (and don’t worry about the gray hair!)
I want to attract new doctors and scientists to Transfusion Medicine. I really try, but most have no interest and look on their rotations as a necessary evil.
I have lowered my expectations for most medical trainees in Transfusion Medicine. They don’t like it, they just want to pass it, and move on. What must I impress them with for their future careers? What is essential for them to remember?
I have had both pathology and non-pathology trainees. Surgical and ob/gyn doctors used to spend one month whereas the hematology and pathology residents/fellows spent on average three months. The few interested in the field might do multiple rotations.
I still gave them lectures on a variety of topics, especially how to transfuse blood components, basic ABO/Rh antigens, compatibility testing, and direct antiglobulin testing. They would forget most of this, but I wanted them to remember TURN-AROUND-TIMES:
How long does it take to perform the test?
Find compatible blood?
Thaw the plasma?
Release a massive transfusion protocol shipment?
Complete a transfusion reaction workup before releasing more blood?
I am not discouraging people from entering the field, but I am a realist to know that few will share my passion for serology or want to take call on difficult immunohematology cases. At least if they understand the pressure the technical staff are in and these turn-around-times this will make both their work as clinicians and mine as transfusion medicine more congenial.
Principle:
Daratumumab is a monoclonal antibody that binds to CD38 antigen, which is expressed weakly on the surface of all RBCs. It may thus cause a positive direct antiglobulin test DAT and so interfere with compatibility testing if an antiglobulin phase is required.
This effect may persist up to 6 months after discontinuing the drug. The monoclonal antibody does not interfere with routine ABO/D typing.
Special techniques (neutralization of CD38 antibodies by CD38 anti-idiotypic antibodies, or soluble CD38 antigen) may remove the panreactivity but are not generally available. DTT, a sulfhydryl reagent may denature the native CD38 antigen on RBCs but it should be used under a biologic hood.
Kell antigens will be denatured so Kell antibodies cannot be detected after treatment so Kell-negative RBCs should be used. In the Gulf Area, this is about 72% of RBCs. In the Medinfo software a rule to require K-negative RBCs has been built.
Policy:
References:
Trick or Treatment, Anti-CD38 Reactivity and How to Treat It, AABB Satellite Symposium transcript, U. Cincinnati and RedMedEd, October, 2015 (attachment)
Principle:
This policy outlines steps taken to minimize the risk of data entry errors and is based on a dualistic approach: review of results by a senior technologist and/or supervisor and various computer safeguards built into the Medinfo Hematos IIG blood bank computer HIIG system. This policy also discusses the verification (here called authorization) and purge processes of HIIG.
Policy:
References:
Recently, I had a case where the blocking antibody was not an anti-D, but rather an anti-B in a case of ABO hemolytic disease of the fetus/newborn HDFN. The D typing result was weak but the D control in the gel was positive so the result was indeterminate. DAT was 3+ IgG and anti-B was identified in the eluate (mother was antibody screen negative, regular elution panels (group O cells) were negative. Some of the actual workup follows:
29/7/20
If there is strong antibody binding to an RBC, this may interfere with a typing reagent attaching to the cell and cause a false-negative, i.e. a “blocking” antibody. Such cells may interfere with the indirect antiglobulin test IAT, i.e. the antibody screen. The autocontrol and direct antiglobulin test DAT will be strongly positive.
The manufacturer’s instructions should be strictly followed for using its reagents in the presence of a strongly positive DAT. If there is no reaction with the typing reagent, the result must be indeterminate.
One could try a (relatively) nondestructive elution method such as gentle-heat elution to remove some of the antibody and then retype the cells. I have found this to be a simple and effective method for my staff to use. Just remember that despite being “gentle,” there will still be some hemolysis present, but here it is the cells we are trying to save.
Usually, we find this situation in a neonate born of a mother with anti-D. The baby has a strong DAT but the D typing is negative. Check the D control carefully: if it is positive, the result is indeterminate, try another method. Usually gel/glass bead methods are subject to less interference. Finally, there is always the classic saline anti-D!
In Medinfo software with a blocking antibody, a nonnegative control will trigger a manual review of the results. There will be no automatic release.
Here is my process for handling blocking antibodies, which I set up for HMC Doha:
INTERIM POLICY: ANTIGEN TYPINGS IN PRESENCE OF STRONGLY POSITIVE DIRECT ANTIGLOBULIN TEST (DAT): RULE OUT BLOCKING ANTIBODY
Principle:
Antigen typing of cells with large amounts of coating antibody (i.e. strongly positive DAT 3-4+) may not always be possible because the bound antibody may block available antigen sites. This policy is to clarify how to recognize and handle such situations.
Policy:
References:
The following was my process at HMC Doha for TRALI/TACO. It includes proactive measures to minimize the risk of TACO and the procedure for surveillance and workup of such cases.
In the Medinfo blood bank computer system, we did not prepare plasma or platelets from female donors. If approved by a transfusion medicine physician, a manual override was made in exceptional cases (e.g. mother donating platelets for her child in neonatal alloimmune thrombocytopenia cases.). In some other countries, they do HLA antibody testing to allow females to donate platelets.
I emphasize that the diagnosis of TRALI and/or TACO is clinical, but the transfusion medicine physicians must always consider the possibility whenever there is an adverse effect associated with progressive respiratory distress.
Principle:
Since TACO and TRALI are major causes of serious adverse effects from transfusions, this policy outlines actions being pro-actively taken to mitigate the risks in Transfusion Medicine. TACO and TRALI may be difficult to distinguish so this policy addresses both.
Objectives:
Tracking:
Risk Management:
Notifications:
Algorithm for Diagnosis and Management of Donors:
References:
Principle:
In accordance with the College of American Pathologists’ accreditation standards, all report structures (content, formatting) are reviewed at least biannually and upon modification by staff designated by the Chairperson, DLMP, here the Division Head, Transfusion Medicine/Laboratory Information System.
Policy:
Reference:
GEN.41077, Content/Format Report Review, CAP Checklist, Current Edition
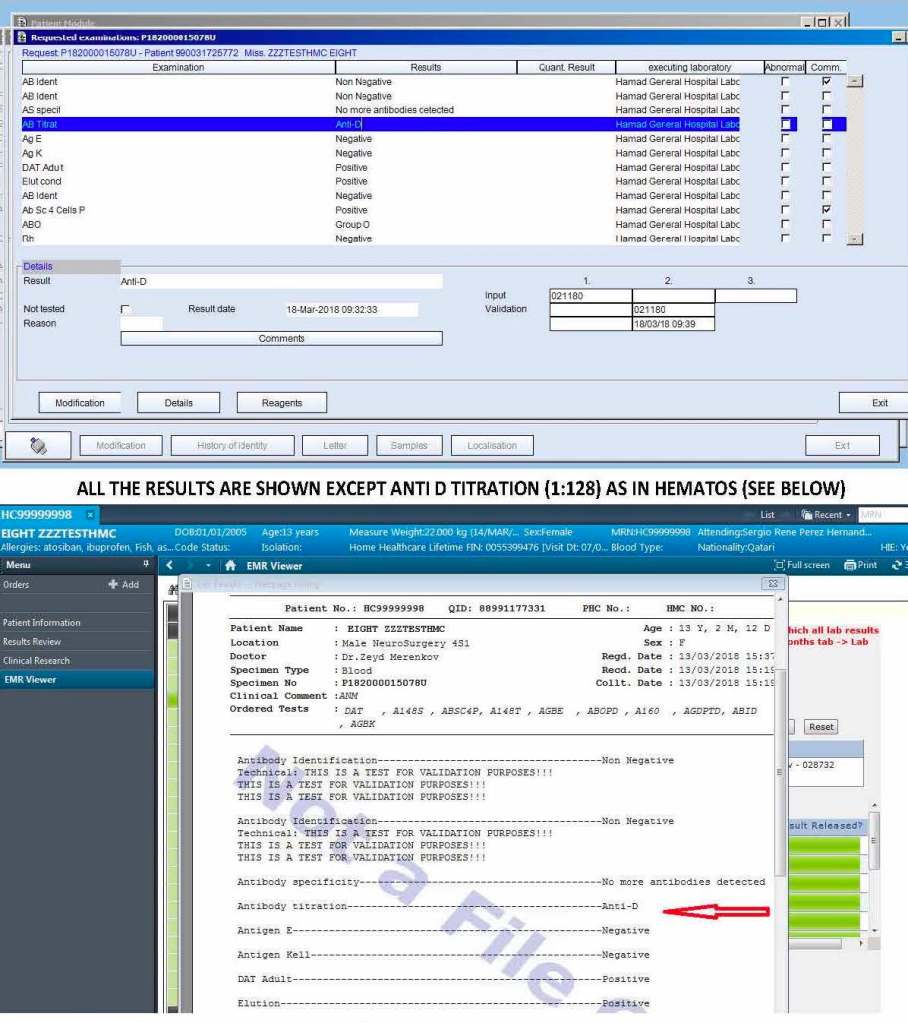
The following is a sample report I prepared during my tenure at HMC Doha:
On the left-hand side of this composite PDF there are embedded attachments, which can be accessed by clicking on each one. In this document, I have shown a sample page from the actual screenshots generated. The data showing is a dummy test patient (no real patient data is exposed).
Note that our design of Medinfo did not include printing copies of reports. The only available reports were the screens. Staff outside Transfusion Medicine viewed the blood bank reports through a separate database viewer. In the example below, the Medinfo screen appears first followed by the EMR Viewer report.