Enumeration: 5.8
Policy:
- All processing will be in accordance with good manufacturing practices.
- All testing will follow manufacturer’s recommended testing methods.
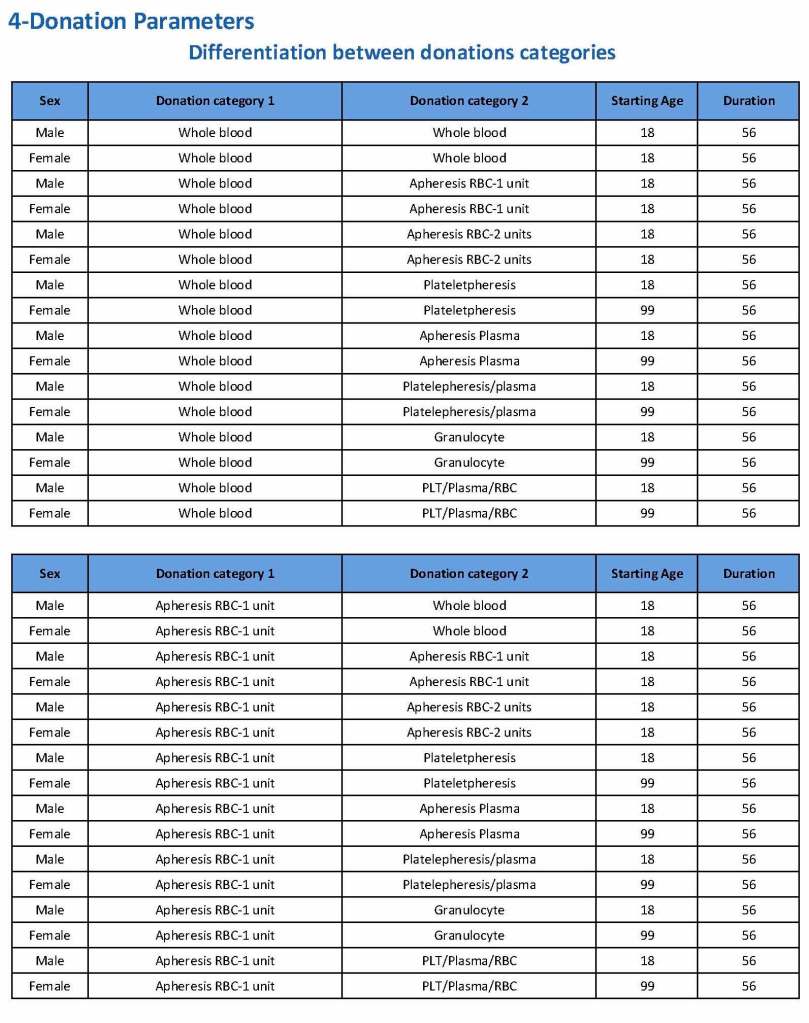
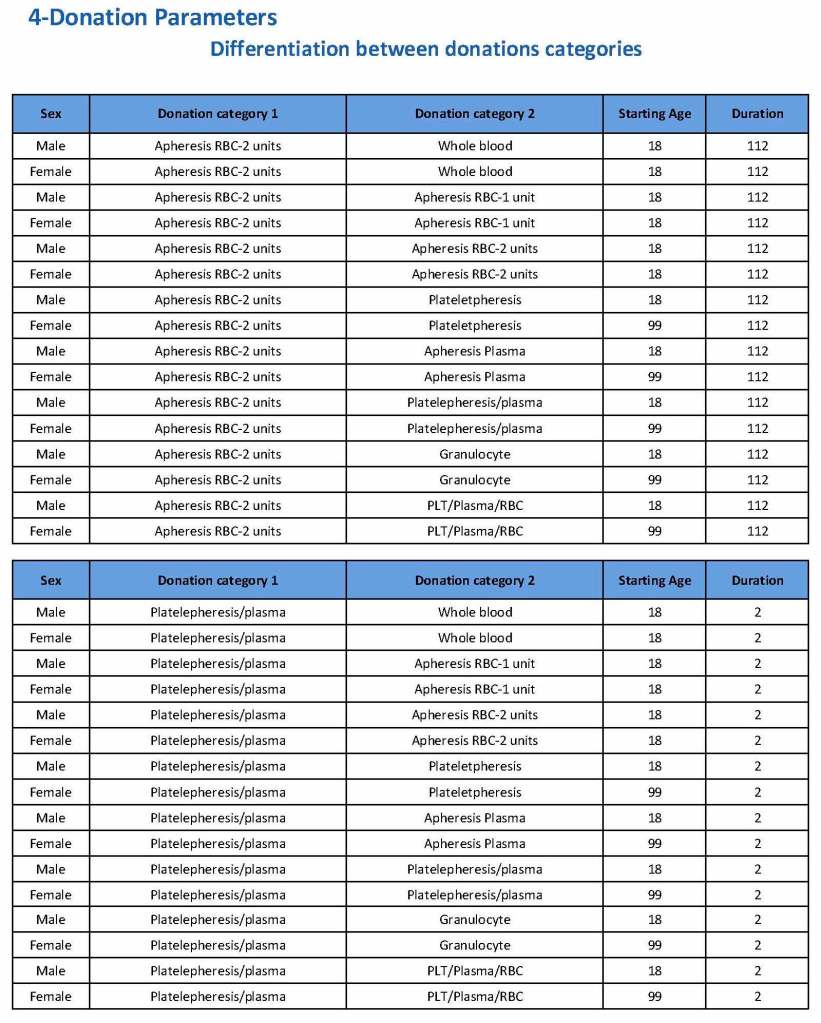
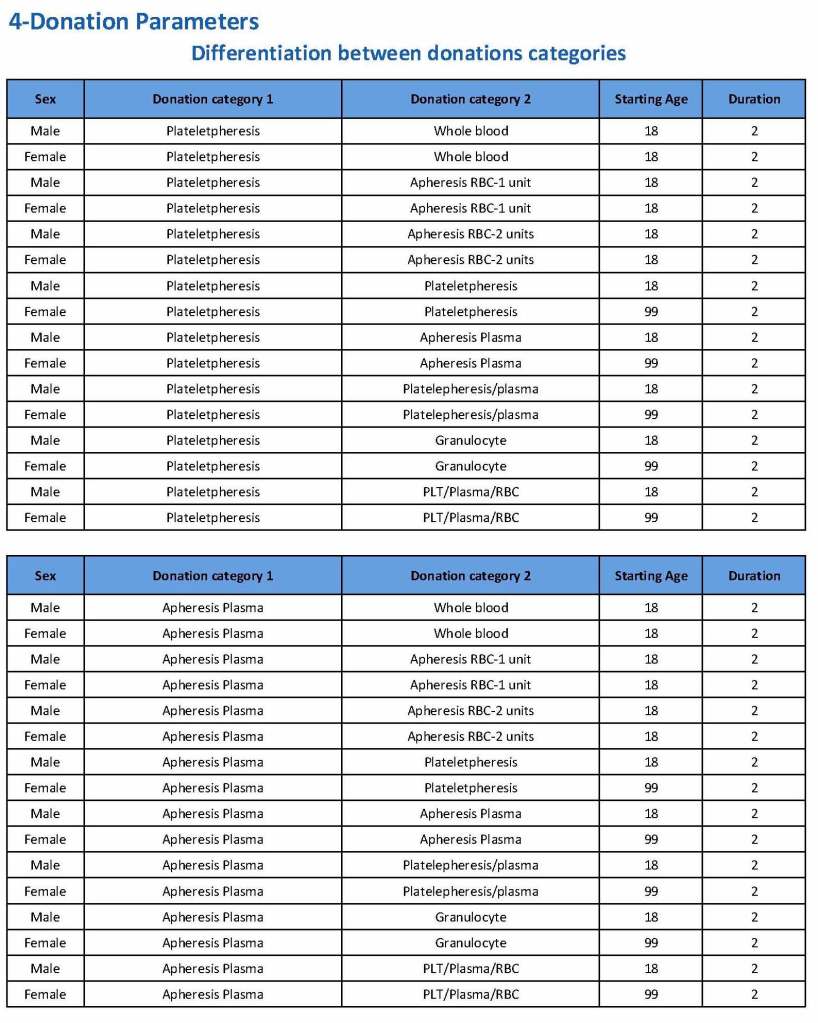
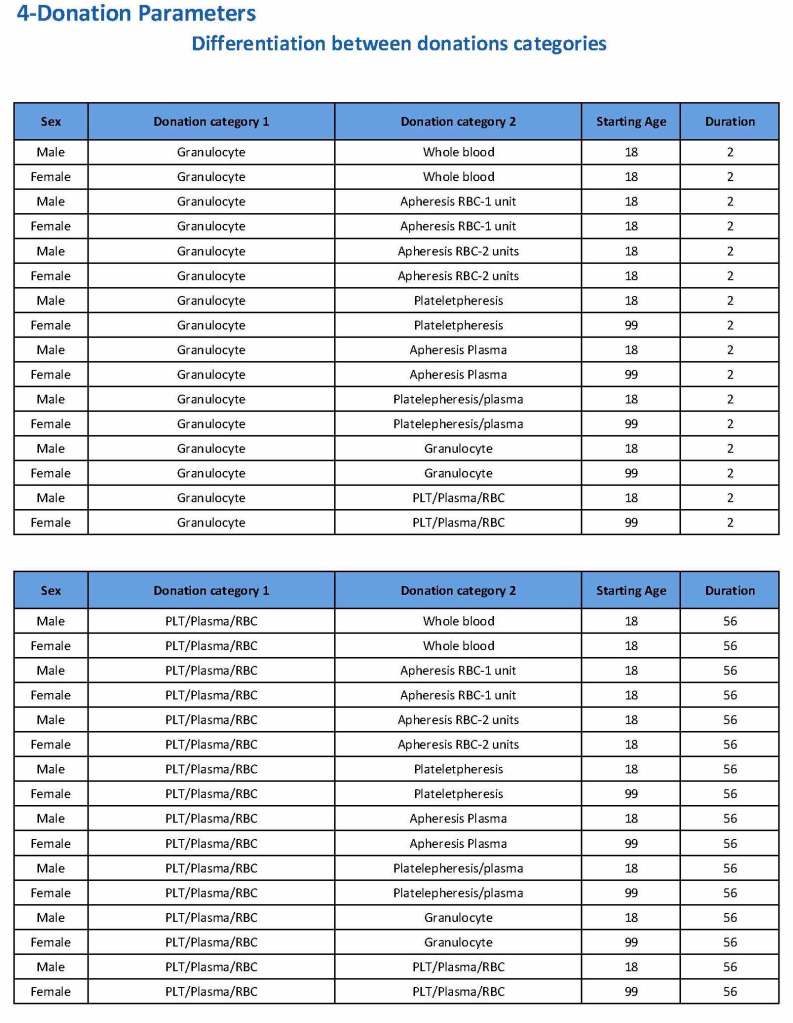
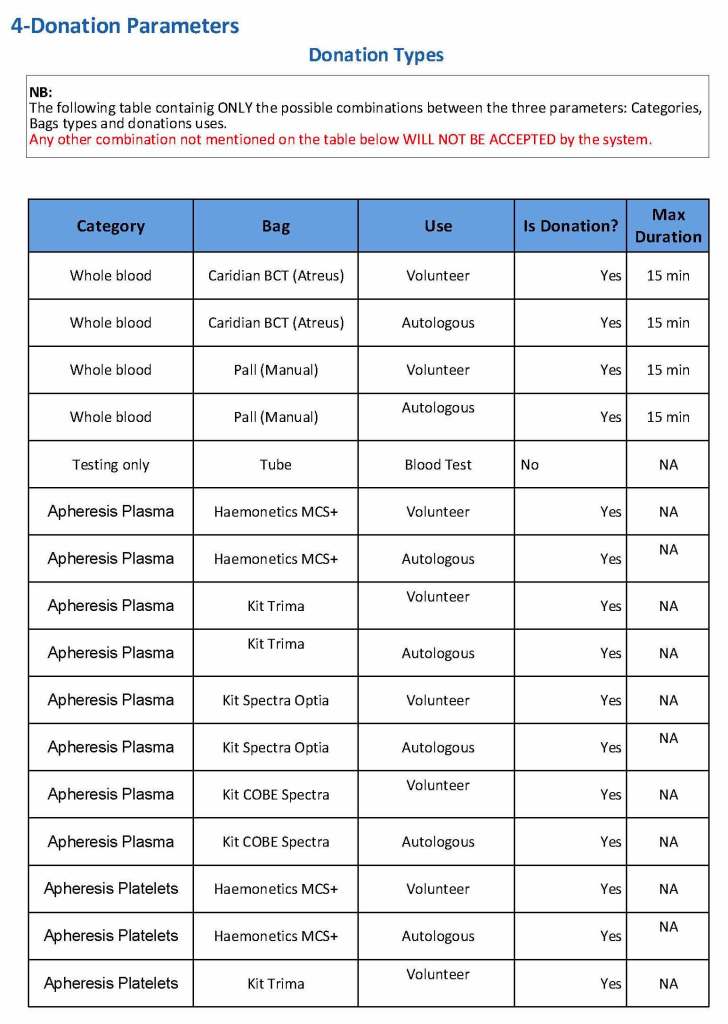
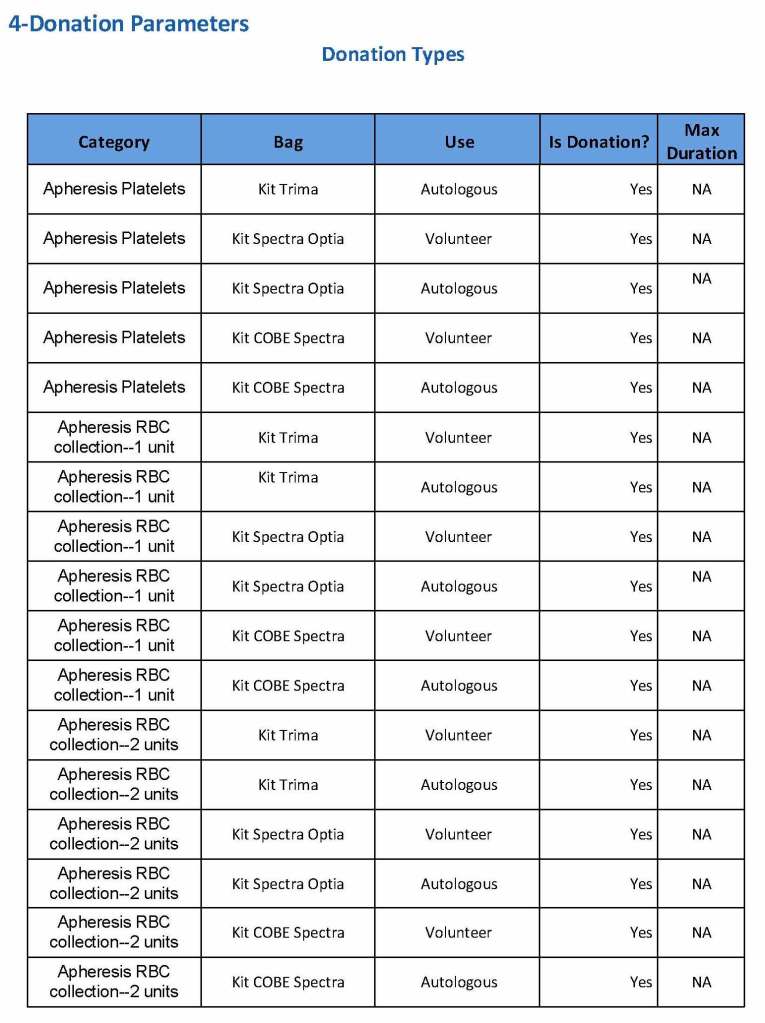
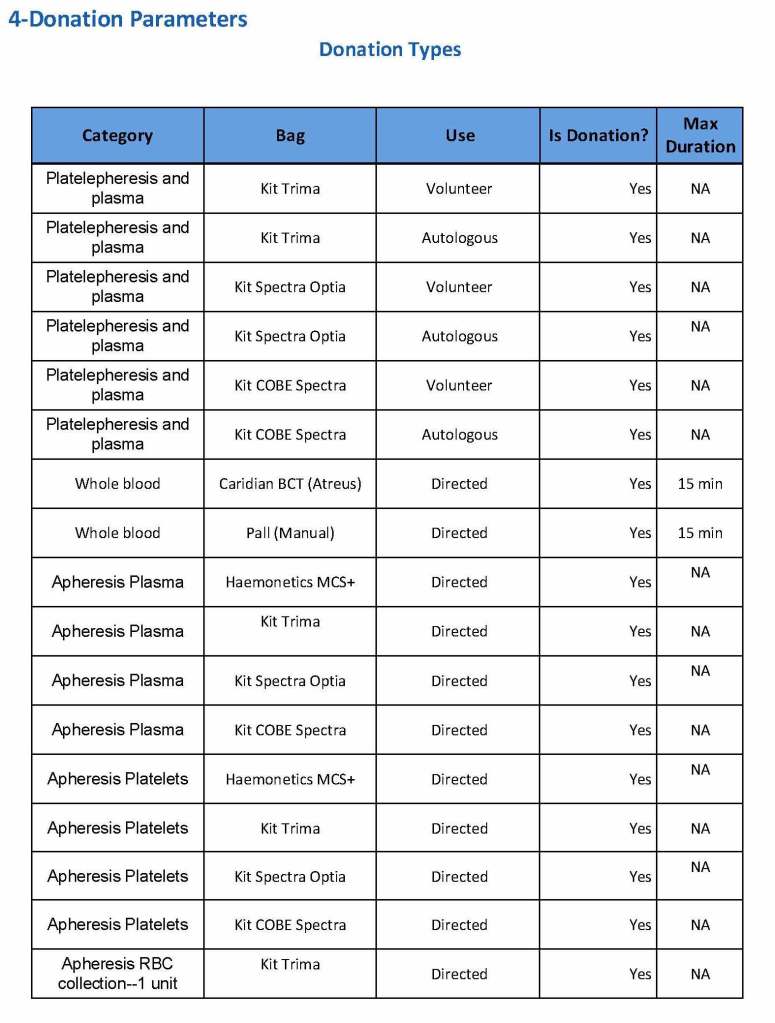
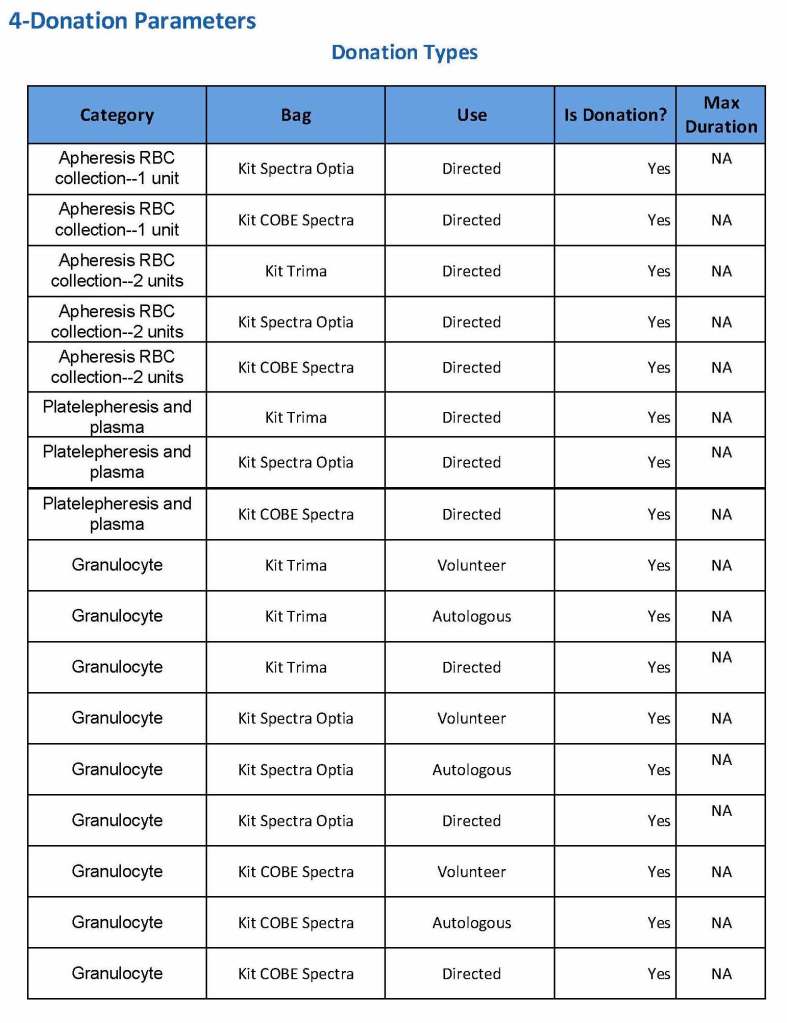
- The specific processing algorithms will be programmed into the Hematos IIG software.
- Validation of the processing will be performed by Hematos IIG, which will control final ISBT labelling
- All abnormal results will be reviewed by a transfusion medicine physician.
- All policies, processes, and procedures must comply with Qatari, HMC, and applicable accreditation standards (i.e. AABB, CAP, and JCI).
References:
- HMC 1001 Setting Specification, Version 1.5, Hematos IIG, Medinfo
- Standards for Blood Banks and Transfusion Services, Current Edition, AABB, Bethesda, Maryland, USA