Principle:
Levels of blood inventory must be maintained to meet usual and unexpected needs and yet still minimize component wastage. The HMC Blood Donor Center is the only source of blood components in Qatar. Because Qatar’s demand for blood components is rapidly increasing, we must assess our desirable and critical inventory levels at frequent intervals.
Definitions:
HGHBB: HGH Transfusion Service/Blood Bank
HIIG: Hematos IIG dedicated blood bank computer software by Medinfo (Nice, France)
TMP: Transfusion Medicine Physician
Policy:
- Establishing desirable and critical inventory levels:
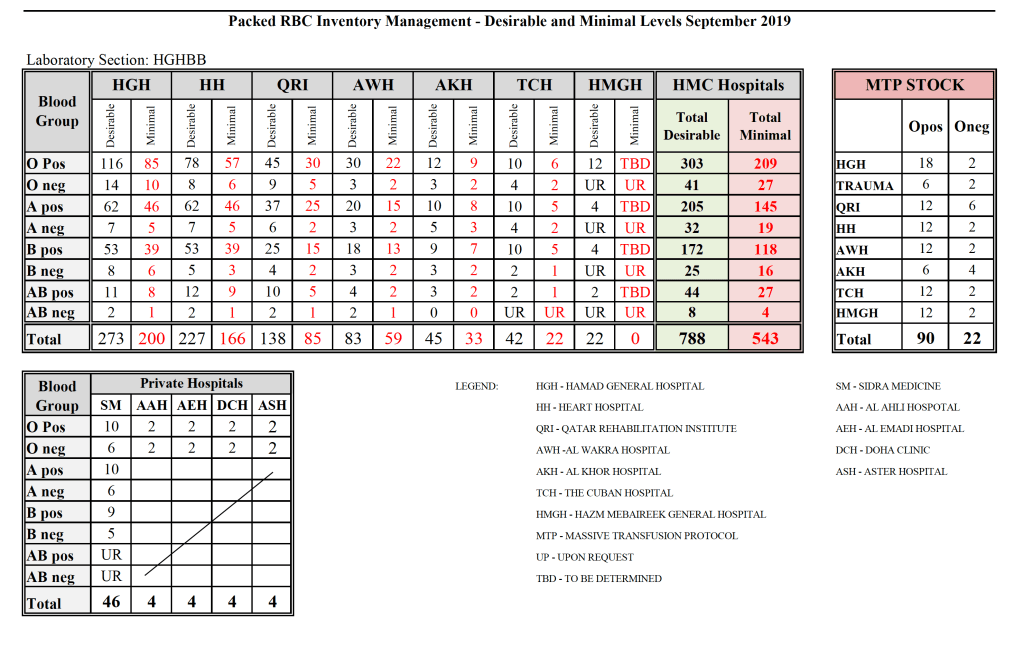
- At least once per year, a review of blood component usage must be made to determine both desirable and minimal (critical) inventory levels for all blood components by group.
- Determine the maximal daily usage of each component in this period.
- Add 10% as a buffer to the maximal usage to determine the critical inventory level.
- Add 50% as a buffer to the maximal usage to determine the desirable inventory level.
- After each disaster and after every period of “critical” shortage, reassess the critical and desirable inventory levels.
- Minimally, even if there are no disasters or critical shortages, the recalculation of critical and desirable inventory levels must still occur at least once per year.
- Contact the HIIG software engineer to change the desirable and critical inventory levels in the computer (cumulative stock entry screen).
- Preventing shortages:
- Maintain adequate stocks of blood bags, Mirasol, and platelet additive solution, reagents, functioning equipment with backup site (at least two of EIA and NAT analyzers, two Reveos and two Mirasol machines)
- Request additional resources (space and staffing) as far as possible in advance.
- Develop an additional testing/processing site for blood components (requested but not effected)
- During shortages:
- Inventory depot (currently HGHBB) technical staff will contact the Senior Consultant/Division Head, Transfusion Medicine or designate on-call whenever there is a critical shortage of any blood component:
- Depending on the severity of the shortage in consultation with the Division Head/Senior Consultant, Transfusion Medicine or TMP on-call will liaise with the key technical, nursing, and recruitment staff.
- Donor Recruitment: Medical Manager, Recruitment/Logistics
- Nursing/Apheresis: Head Nurse, Blood Donor Center
- Donor Marker Testing: Supervisor, Donor Marker Testing
- Blood Component Processing: Supervisor or Senior Technologist, Processing
- Hospital Transfusion Services: Supervisor of Blood Depot (currently at HGHBB) and supervisors of all other hospital transfusion services/blood banks
- Medinfo HIIG Software Support/VHT Services:
- Depending on the severity of the shortage various actions may be approved by the Senior Consultant/Division Head, Transfusion Medicine:
- Transfusion Physician/Medical:
- Refer to Medical Director to review all requests for the critically short component(s) and provide initial triage usage
- Maintain close contact with clinical team(s) about request, emphasize need to minimize ordering if possible
- Refer cases of catastrophic blood use to a multidisciplinary ad-hoc team of physicians as designated by the Corporate Transfusion Committee and Medical Director (appointment of ad-hoc team currently under consideration by Medical Director)
- Transfusion Physician/Medical:
As of this date (23/9/19), the Medical Director has not yet appointed a triage team for severe blood shortages. The Transfusion Medicine physicians DO NOT serve as gatekeeper at these times. It must be a committee including clinical medical staff who are the principal end-users of blood components
- Recruitment:
- Mobilize recruitment/registration/aide staff
- Generate SMS lists to contact donors of the affected component type
- Contact media (radio, TV) and hospital intranet to put out messages to recruit donors
- Prepare mobile blood donor vehicles for emergency donor campaigns
- Arrange emergency transport of prepared units to affected site
- Extend Blood Donor Center hours of operation
- Nursing:
- Mobilize nursing/phlebotomy staff
- Extend staff working hours as needed
- Reschedule therapeutic apheresis cases as determined by the TMP
- Marker Testing:
- Mobilize staff to perform extra infectious marker testing run
- Component Processing:
- Mobilize staff for component processing (including filtration, pathogen-inactivation, and use of platelet-additive solution)
- Inventory Depot/Hospital Transfusion Services/Blood Banks:
- Maintain critical inventory level monitoring
- Report to Senior Consultant/Division Head, Transfusion Medicine or TMP on acute inventory levels
- Cancel non-emergency requests for critically short components
- Release components on expedited basis (MTP, emergency release, immediate-spin crossmatch, etc.)
- Computer:
- Medinfo/VHT software engineers to monitor system, provide support as needed
- Notifications:
- Contact the Chairperson, DPLM, and/or the HMC Medical Director as needed, especially if stocks are in danger of depletion.
- Any alterations in the blood orders must be communicated to the patient’s most responsible physician by TM technical staff, TMP, or Senior Consultant/Division Head Transfusion Medicine
- Post-Event Analysis
- Review effectiveness of all actions taken
- Modify process based on review
- Update Interim Policy
- Request additional resources as required
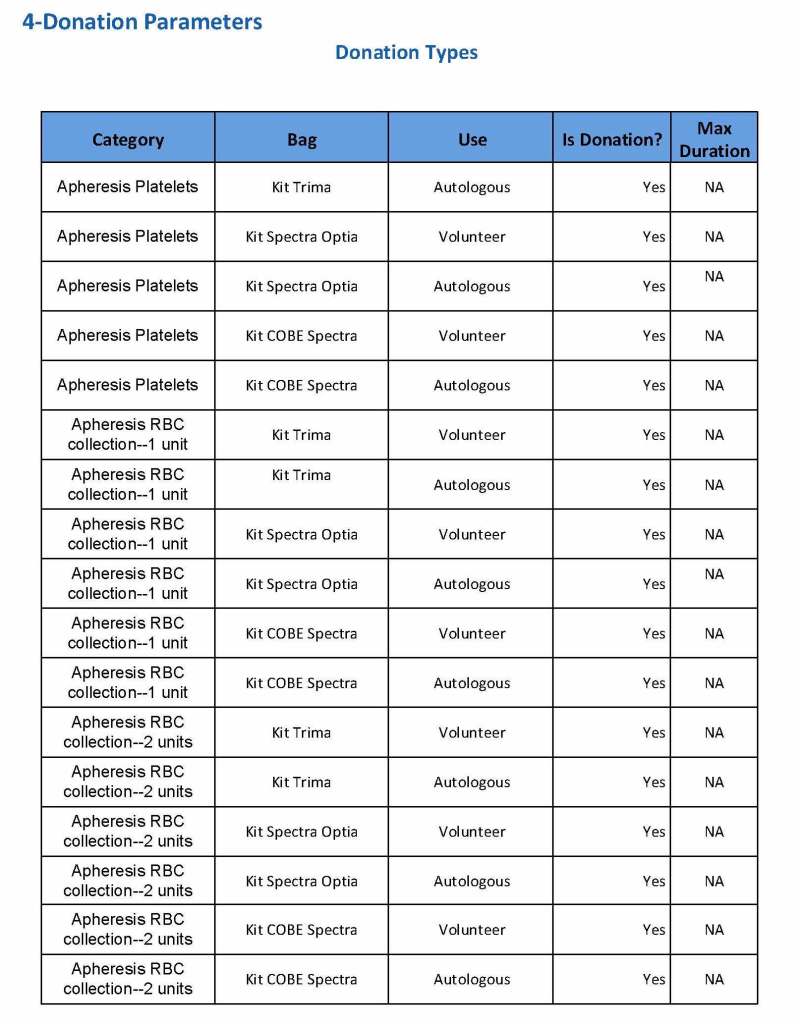
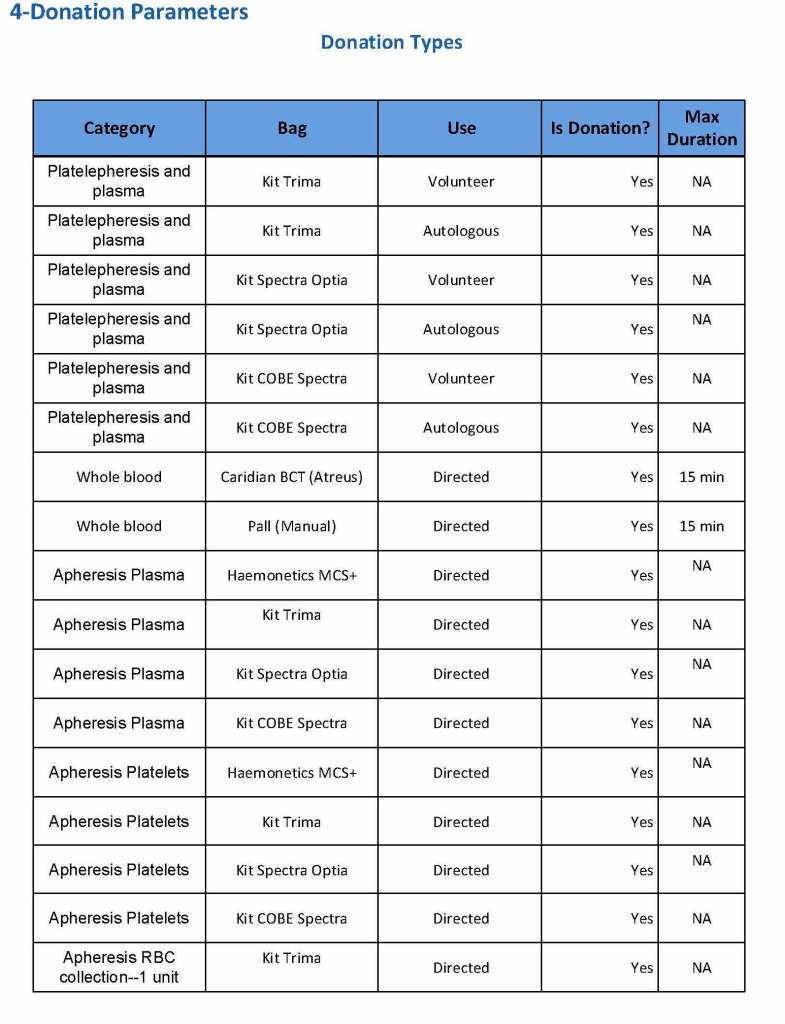
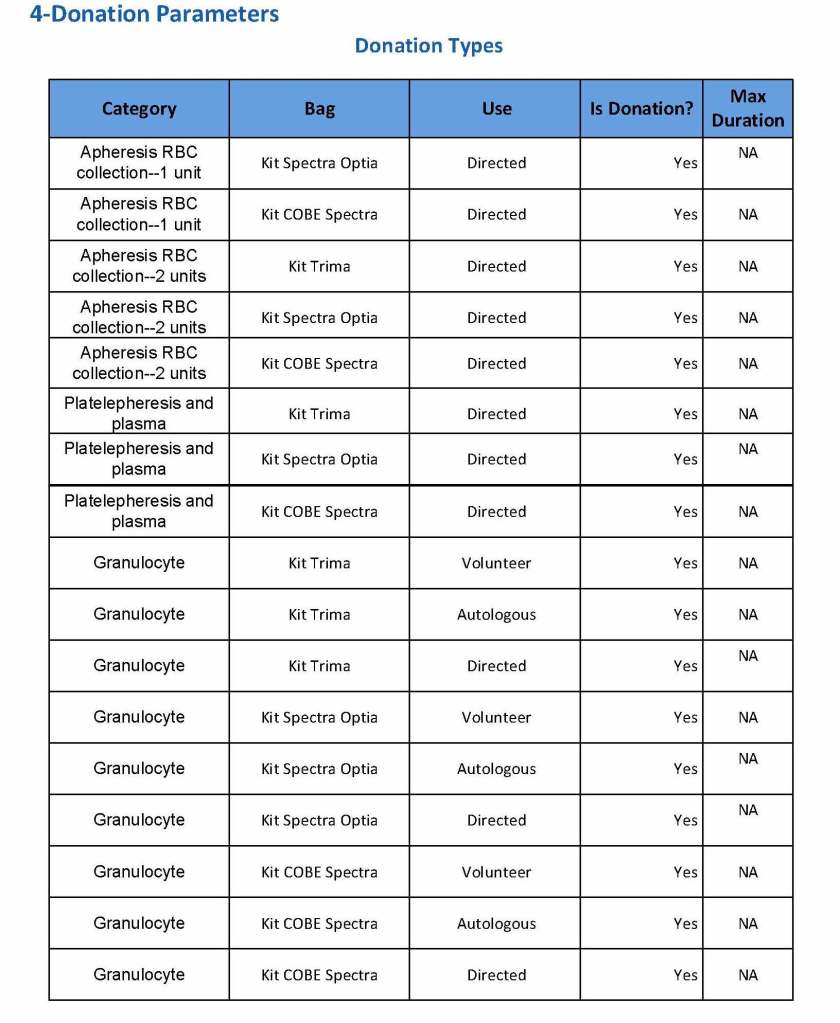
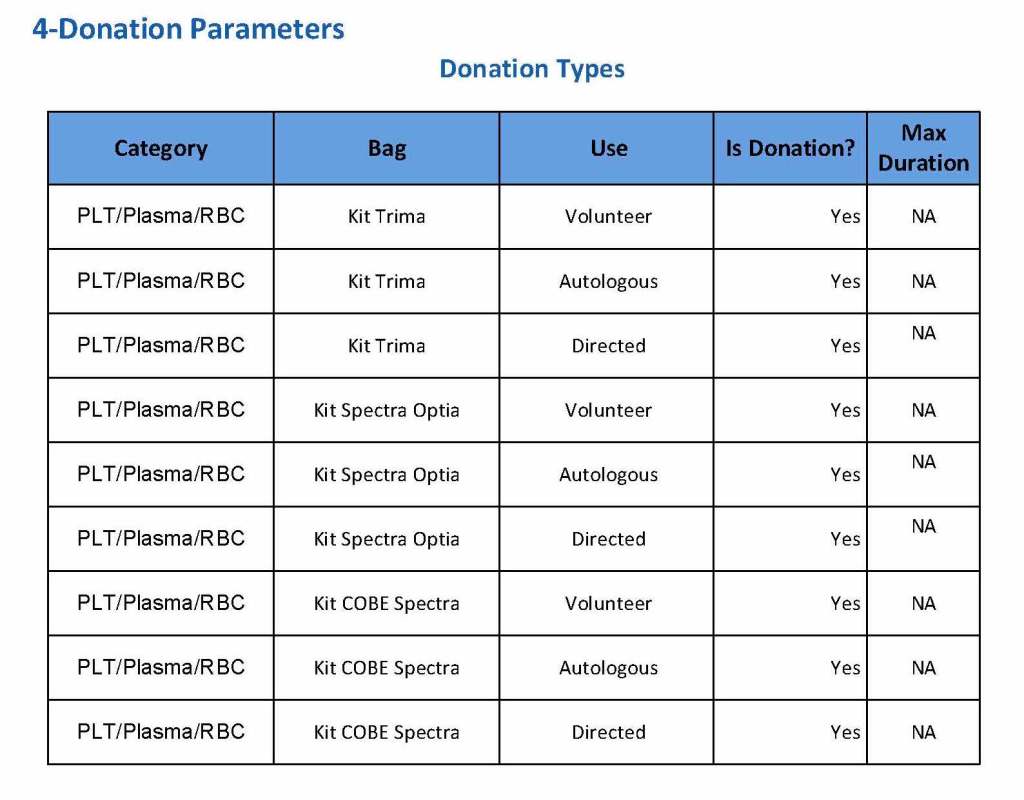
Attachment:
Current inventory calculation (follows)
References:
- Standards for Blood Banks and Transfusion Services, Current Edition, AABB, Bethesda, MD, USA
- Guidelines to the Preparation, Use, and Quality Assurance of Blood Components, European Committee (Partial Agreement) on Blood Transfusion (CD-P-TS), 17th Edition, 2013