Includes registration, questionnaire, physical exam and arm check, collection, marker testing, component separation, donor immunohematology testing
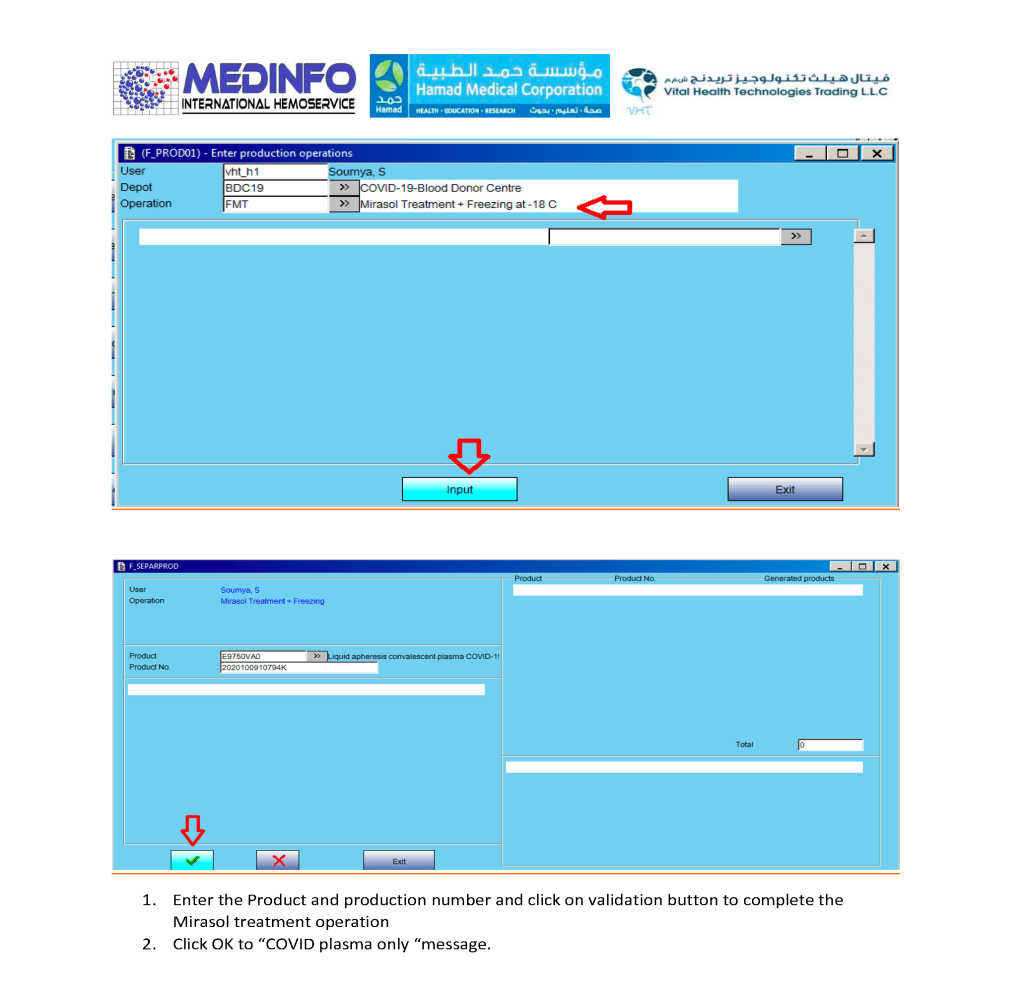
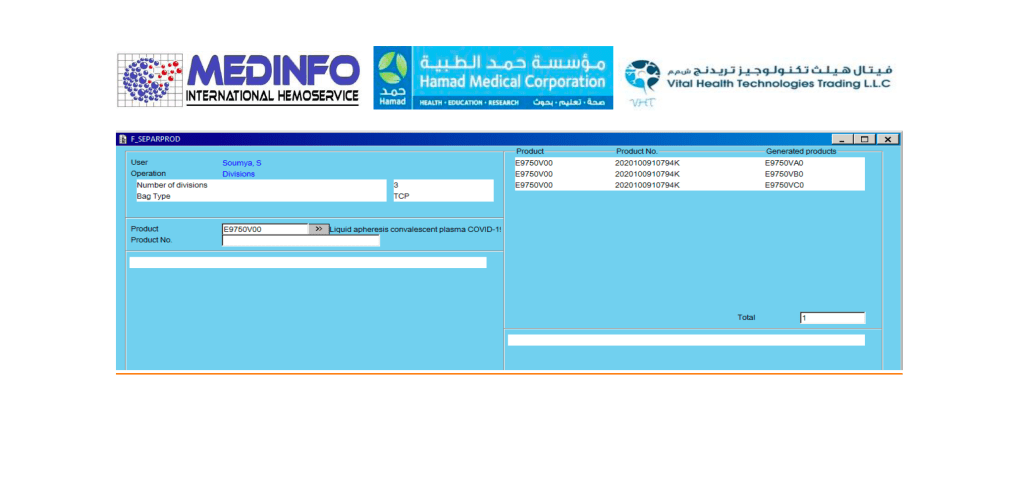
This is a part of a series of posts on the actual Medinfo design of the CCP donation and release processes. The registration of the donor and site, donor questionnaire/collection, and receipt/division of the product were covered in recent previous posts.

Principle:
For the purpose of typing blood donors, we want to detect weak and partial D types and consider them as D-positive since even a portion of the D molecule is immunogenic and sensitization to it may cause anti-D hemolytic disease of the newborn.
Background:
Ortho Diagnostics Reagents use three different monoclonal antibody cocktails that react variably with the antigen D (Rh1)—these are found on TWO (2) cards: Anti-A/B/A,B/D/CDE and Anti-DVI:
Anti-D/Anti-RH1—IgM monoclonal antibody clone D7B8 can detect most examples of weak and partial D including weak D types 1, 2, 3, 4.0, and D categories II, III, IV, V, VII, DBT, and R0Har. It does NOT detect category VI. Retest positive reactions of 2+ or less by an alternate method. It may show different serologic activity compared to other D typing reagents.
Anti-CDE/Anti-RH1,2,3—IgM monoclonal blend of clone MS24 (anti-C), clone MAD2 (Anti-D), and clone C2 (Anti-E) can detect most cells expressing C, D, or E antigens. Most examples of partial D including DVI and weak D express C or E antigens and will be detected directly by the included anti-D or indirectly by the anti-C or anti-E in the cocktail. It does NOT detect Rh:33 (R0Har).
Anti-DVI/Anti-RH1 will agglutinate cells with a DVI phenotype, analogous to our previous DVI+ reagents.
Policy:
| Pattern # | Anti-D/D7B8 | Anti-CDE | Anti-DVI | D-Interpretation |
| 1 | Positive | Positive | Positive | D-positive |
| 2 | Positive | Positive | Negative | Do additional testing |
| 3 | Positive | Negative | Negative | Do additional testing |
| 4 | Negative | Negative | Positive | Do additional testing |
| 5 | Positive | Negative | Positive | Do additional testing |
| 6 | Negative | Positive | Positive | D-positive, probable DVI variant |
| 7 | Negative | Positive | Negative | D-negative, probable rare genotypes r’ and/or r’’ |
| 8 | Negative | Negative | Negative | D-Negative |
If the reaction is 2+ or less with the Ortho anti-D/D7B8 reagent or 1+ with either the CDE or DVI reagents is patterns 2, 3, 4, or 5 above, repeat by another manufacturer’s reagents, including DVI+ and DVI- sensitivities.
Medinfo-Ortho interface settings for Blood Donor Center:
| Anti-D/D7B8 | Anti-CDE | D-Interpretation |
| 3,4 | 1,2,3,4 | D-positive |
| 3,4 | 0 | Indeterminate |
| 0 | 0 | Indeterminate |
| 0 | 1,2,3,4 | Do DVI REFLEX |
| REFLEX DVI | If DVI-pos, then D-positive | |
| REFLEX DVI | If DVI-neg, then D-negative | |
| 0 | 0 | D-negative |
| ~ | ~ | Indeterminate |
~ means any other result
Note all of the following:
References:
This is a part of a series of posts on the actual Medinfo design of the CCP donation and release processes. The registration of the donor and site and donor questionnaire/collection were covered in recent previous posts.
\
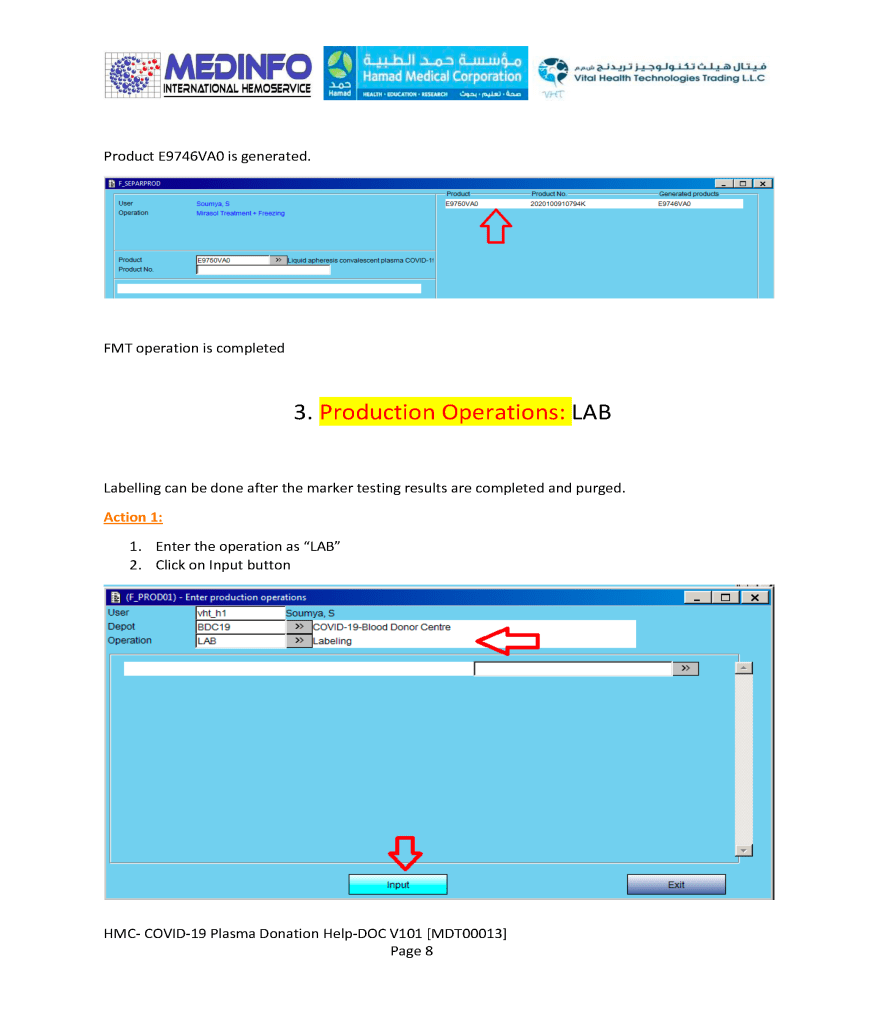
The process (pathogen-inactivation with Mirasol and freezing) wiil continue in a subsequent post.
I was recently interviewing a candidate for consultant in Transfusion Medicine. Several months previously he had completed a fellowship in Transfusion Medicine in the United States. He was applying for a position in my hospital in Qatar, which included seven hospitals and a blood donor center. He had no training in donor management or therapeutic apheresis.
The successful candidate was to rotate on-call to cover all hospitals and the blood donor center. He had never worked outside the United States. Routinely, he did not review antibody panels since those workups were usually sent to the local blood provider there. In his training, he had strictly followed US FDA and American version of AABB Standards. His training center did not routinely do extended phenotypes (C, c, E, e, and Kell). Extra testing and phenotyping had to be explicitly ordered by the clinician to get reimbursement. Thus, there was no prophylactic antigen matching done on patients. He did not feel comfortable reviewing antibody panels.
He had no experience with universal leukodepletion, pathogen-inactivation, platelet additive solutions, or automated component production such as the Terumo BCT Reveos. He did not interpret donor marker testing results.
On the contrary in our organization, the transfusion medicine physician had to review all antibody panels (usually he was the most knowledgeable person for this). We followed the Council of Europe CE and other practices that did prophylactic antigen matching. We were also in charge of donor qualification and therapeutic apheresis and reviewed any product deviations from the Reveos and donor marker testing.
Clearly, this candidate did not practice transfusion medicine in the way that was necessary for our operations. We could not cut him loose and make him responsible for a hospital transfusion service or the blood donor center.
Let us contrast this candidate for one being recruited for anatomic pathology/histopathology. Grossing specimens, performing frozen sections, reading slides, diagnosing cases are the same everywhere in the world. After completing his American certification, he could perform his profession almost anywhere in the world.
Transfusion medicine practices need to be localized and the selection of blood components and donor qualification are different. Most of the world does not follow US FDA and has access to blood components, tests, and other technology that is different and maybe more advanced than his training in the USA.
I gave him a clinical scenario to interpret. An AB patient with anti-K needs to be transfused with plasma. Are there any special requirements for the plasma? What if the only AB donor had anti-K would you use it? What if the only RBCs available had not been phenotyped for Kell? What would you do?
He did not know that we discard plasma with clinically significant alloantibodies routinely. He did not want to phenotype the RBC unit for this patient since this had not been explicitly ordered by the clinician.
My recommendation was not to hire this candidate if there were others who had worked in European or similar systems to our own practices. In effect, to use this physician, he would have to undergo a mini-fellowship to learn our practices since they were contrary to ours. Unfortunately, we were very short-staffed and did not have resources to offer this training.
In summary, blood bank practices are very localized. If you are considering to hire staff from other countries not following your standards, you must assess if the candidate is flexible to change his practices and/or whether you have the resources to train the physician.
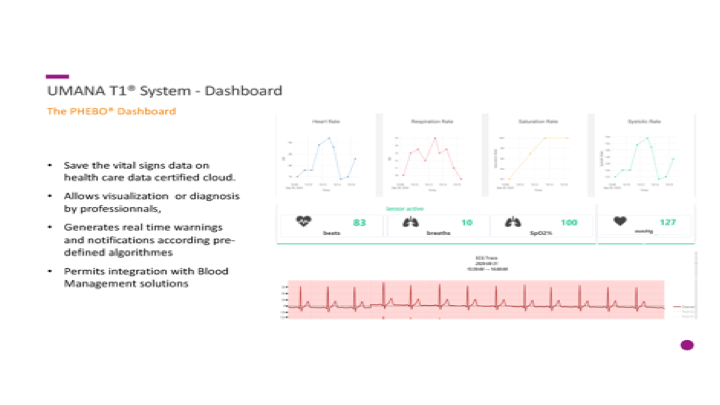
Everyone is excited at the potential of using stem cells for research and therapy. Below is my presentation of the logistics necessary to get those stem collected in an orderly manner, especially in this time of the COVID-19 pandemic. It will also consider blood bank software logistics.


I am a co-author on this paper just being released titled The impact of COVID-19 Pandemic on Blood Supplies and Transfusion Services in the Eastern Mediterranean Region. It compares the responses made by different countries in the region.
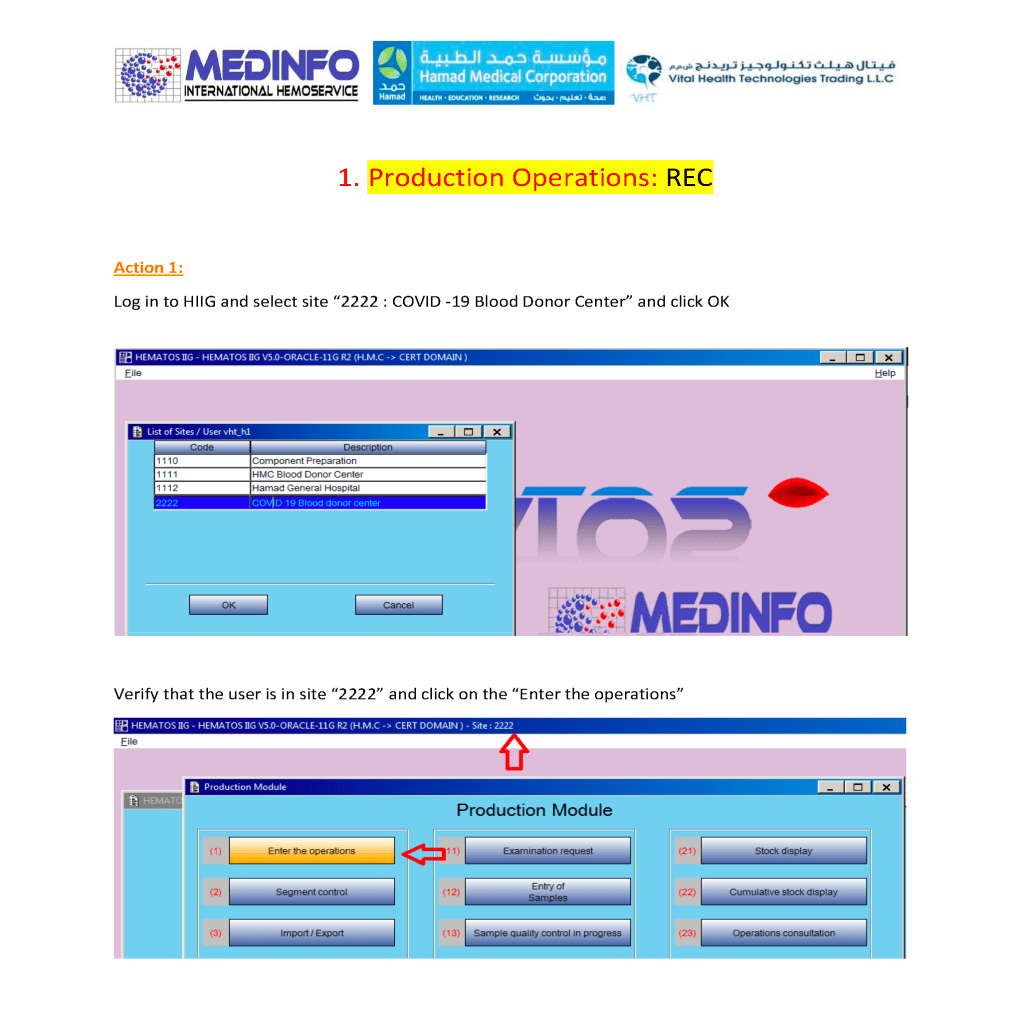
This is a part of a series of posts on the actual Medinfo design of the CCP donation and release processes. The site and donor registrations were covered in a recent previous post.
Donor Questionnaire and Physical Examination:
After registration, there is the online CCP donor questionnaire and vital signs entry.
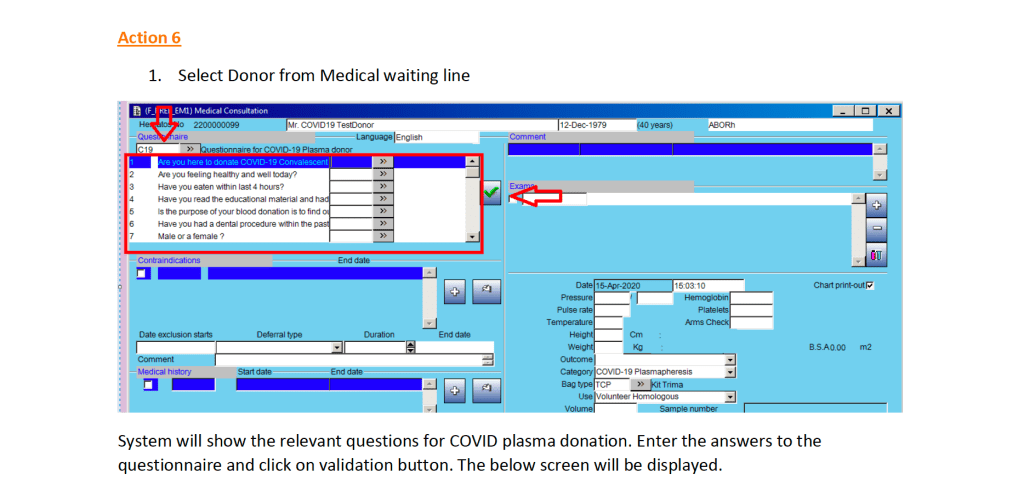
Note that the CCP donor will automatically be excluded from other types of donation. All other types will appear as contraindications in RED below.
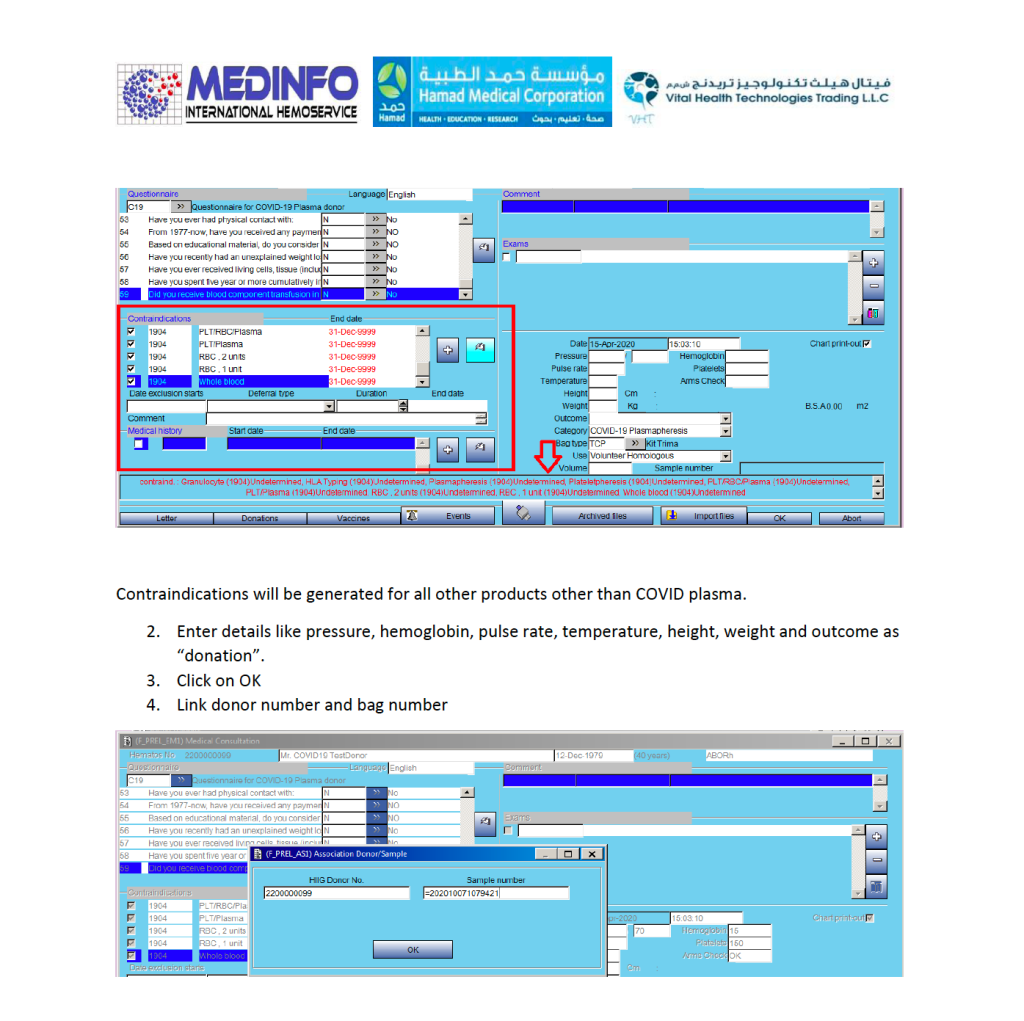
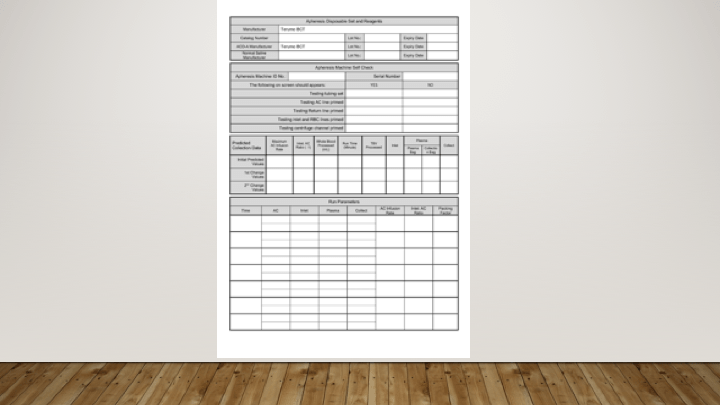
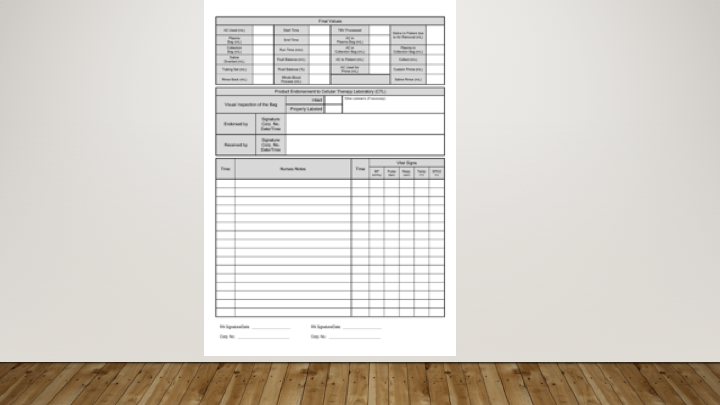
Donor Apheresis Collection:
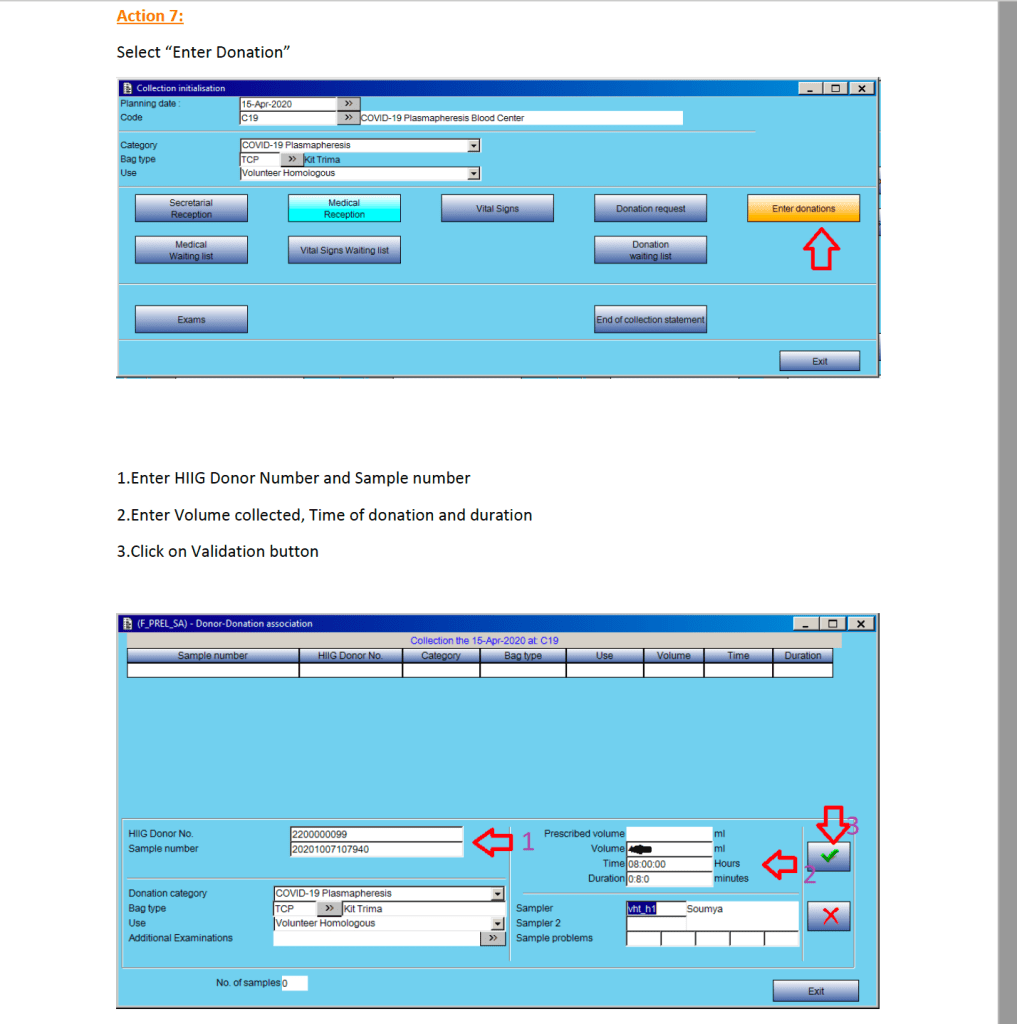
The actual donation process is the same as for plasmapheresis donors: