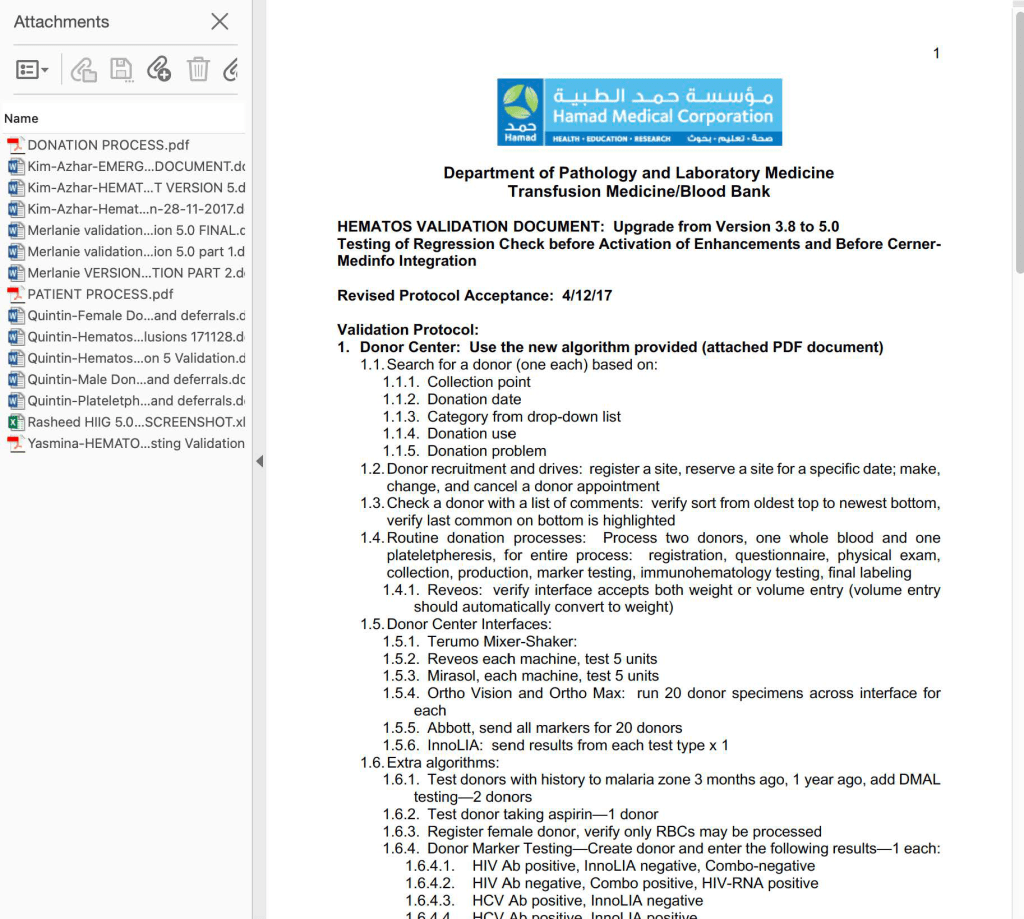
I designed a completely quarantined process for collection, processing, and release of CCP at HMC Doha. This document shows the Medinfo process for donor registration as a separate donor center code.
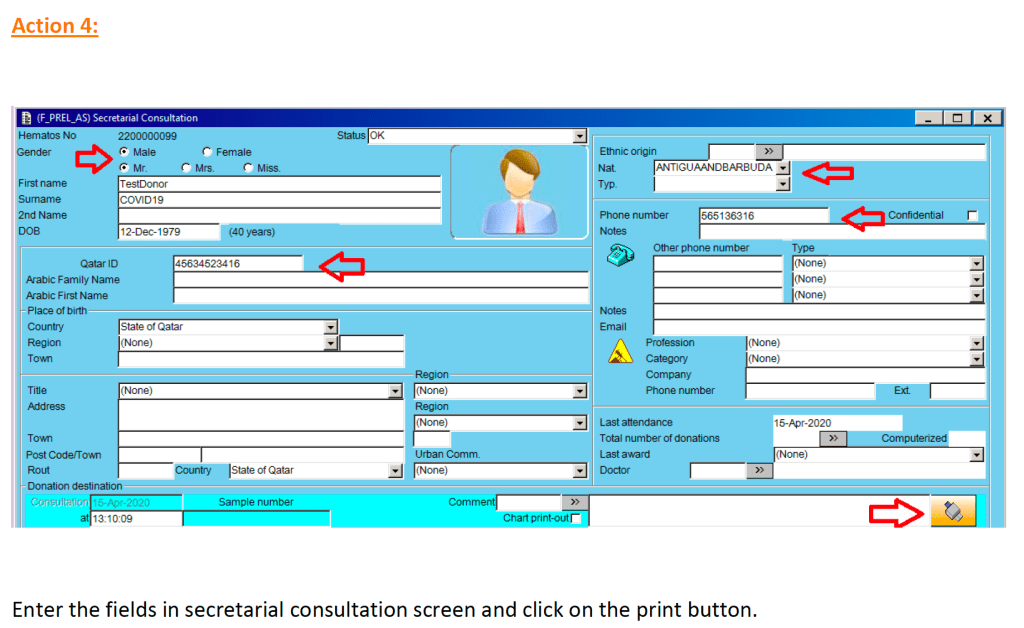
Check donor history and donor deferral database. If there is no previous encounter, generate a new donor file:
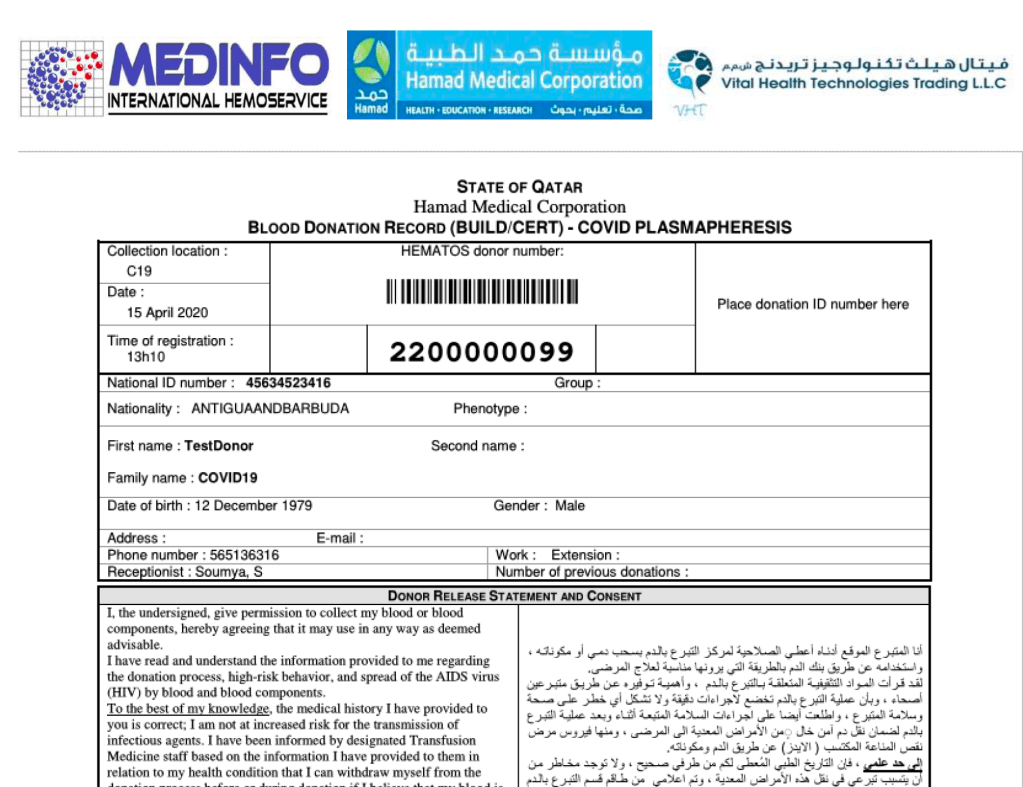
At the completion of this action, the Blood Donation Record with the donor unit number (in this example 2200000099) and consent form in English and Arabic is generated.
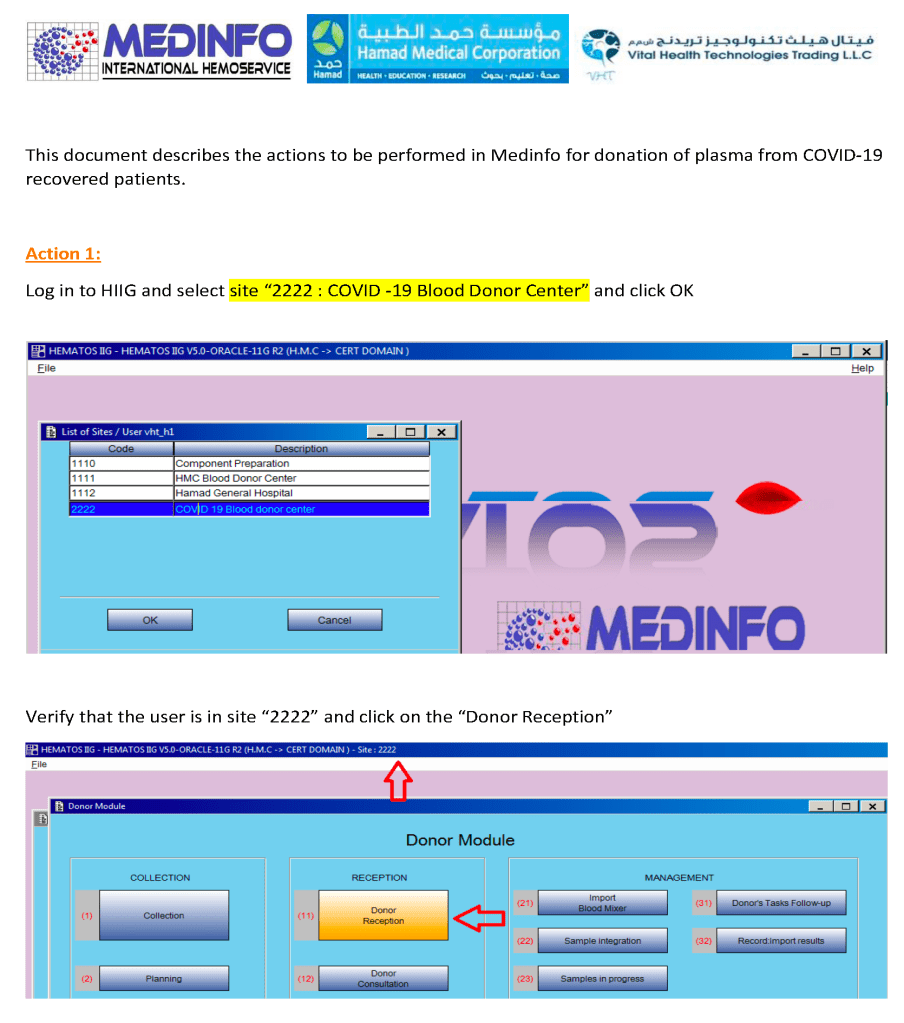
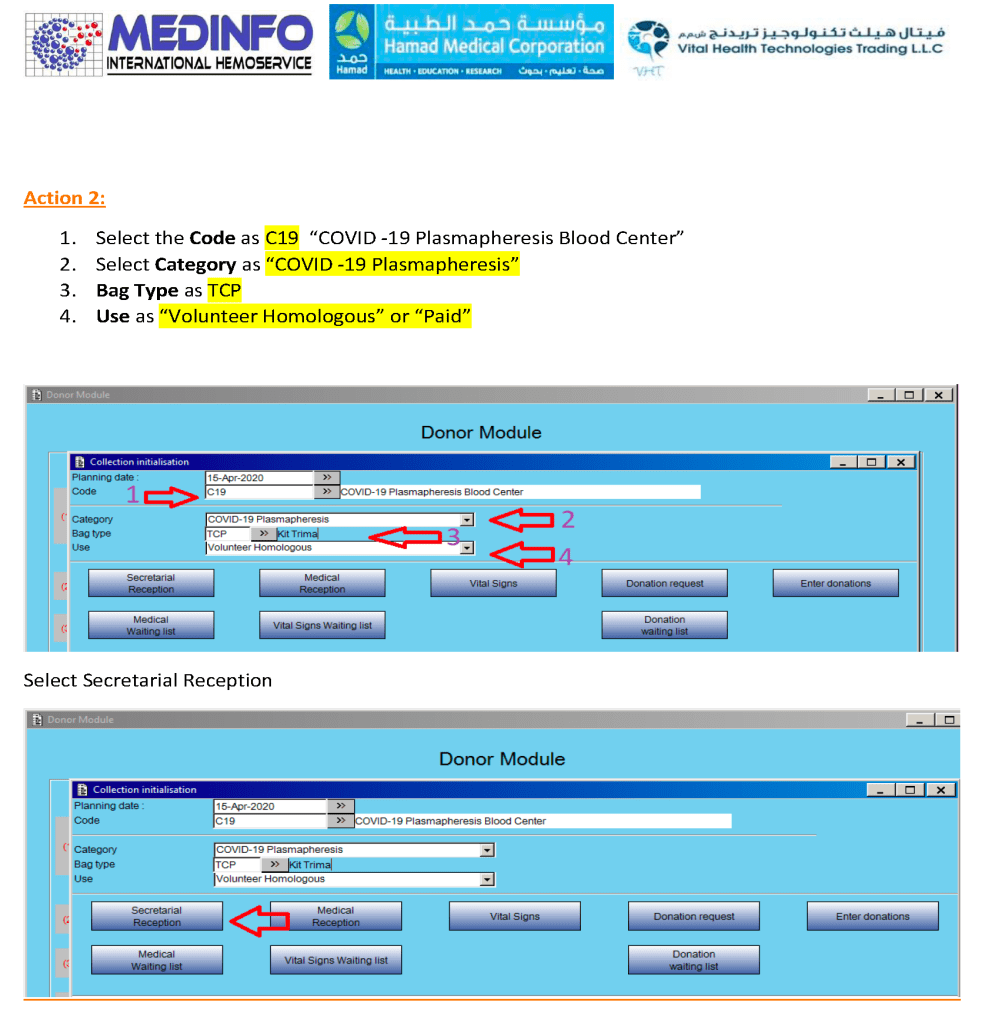
CCP could only be collected at this special site and only the apheresis bag could be used for collection. Regular donation options were not available at this CCP site nor was CCP collection an option at the regular donation sites.
Collection/registration/screening must be in a separate area from regular blood and apheresis donations.
Donors must provide consent.
ISBT specimen labels must be used on each tube collected.
We need a minimum of two apheresis nurses, one for the registration/screening/post-donation observation and one for the actual apheresis procedure.
If there will be multiple serial donors, then we need a waiting area (each donor at least 2 meters apart).
Donor screening must be in sound-proof area so that other waiting donors cannot hear the interview/questionnaire process.
Amount that can be collected depends on body weight: 500 ml for <80 kg and 600 ml for >= 80 kg, collection may occur twice per week
Collection time includes 15 minutes for registration/interview/physical examination, 60-75 minutes and 15 minutes for cleanup/disinfection before the next case, approximately 2 hours per donation.
A post-donation observation area (minimum 15 minutes after collection) with apheresis nurse nearby in case of reactions is needed if there will be multiple donors.
Specimens will
Module 2:
Donor testing and donor immunohematology will be done with other donor specimens in our regular location
Module 3:
Apheresis collection must be processed and stored separately from regular blood/apheresis donations.
Processing will occur only after the results are shown to meet all criteria.
Pre-collection testing (test-only donation) would permit processing without waiting for results.
Storage at minus 80C may be for a minimum of six (6) years but this may be extended if needed.
All acceptable components will have a final ISBT label—no products without the ISBT label will be transfused. The ISBT label indicates that the unit meets all donor criteria for convalescent plasma.
Module 4:
Product modification (thawing) and release (sign out from blood bank) must be in a separate area(s) from the regular hospital blood bank.
Release of convalescent plasma follows the same process as regular component release
Transfusion of convalescent plasma at the patient’s bedside follows same process as regular component transfusion
Nursing and other staff performing the transfusion must pass competency assessment.
Plasma will be transfused as ABO-identical or compatible unless low ABO-titer group A is used.
Plasma must be free of clinically significant antibodies
Workflow Considerations:
Donors must be restricted to the waiting, collection, or post-donation observation areas.
Donors must NOT pass through production, testing, or component release areas (just as they are currently restricted in the Blood Donor Center and HMC hospital blood banks/transfusion services).
Logistics:
Throughput is a maximum of 4 donors (2000 to 2400 ml plasma) per eight-hour shift with one apheresis nurse and one donor apheresis (Trima) machine.
The processes are scalable with additional staff and machines (e.g. with 3 machines and nurses, then 12 donors and 6000 to 7200 ml of plasma collected).
Thawing of 1-2 units of plasma takes up to one hour. Contact the quarantine blood bank at least one hour before the desired pick-up time.
The four modules above can be in separate areas not adjacent to one another. Modules 1, 3, and 4 must be quarantine areas where access is limited. Module 2 can be performed with regular donor specimens using standard precautions.
We can provide training for transfusion of blood components and competency assessment to any location transfusing this product.
Information Technology:
All modules will be connected to the Medinfo Hematos IIG dedicated blood bank computer system.
All records of collection/production/testing/storage/modification/release will be stored therein.
All ordering of convalescent plasma components will be through Medinfo.
External test results (e.g. future antibody titering) can be added to the component information.
Links to the Hospital Information System (Cerner) may be considered after the Medinfo processes are fully functional.
I designed a completely quarantined process for collection, processing, and release of CCP at HMC Doha. This document shows the Medinfo process for site registration as a separate donor center code.
CCP could only be collected at this special site and only the apheresis bag could be used for collection. Regular donation options were not available at this CCP site nor was CCP collection an option at the regular donation sites.
This has been revised to recommend the use of a continuously recording portable vital signs device such as Umana’s UT1M (GPI, Italia) which includes PAO2 and heart rhythm measurements.
Principle:
All therapeutic apheresis procedures are potentially life-threatening and must only occur by an order from a transfusion medicine physician with experience/competence in such procedures.
Definitions:
Referring Physician is the clinical physician requesting a therapeutic apheresis procedure.
Transfusion Medicine Physician is a physician in the Transfusion Medicine Section with medical privileges for therapeutic apheresis procedures. This includes the Head, Transfusion Medicine, consultants in Transfusion Medicine, and designated specialist physicians in Transfusion Medicine. The final decision to accept/reject the patient is made by the transfusion medicine physician.
Covering Physician is the clinical physician designated by the referring physician to be physically present and covering the patient in case of any adverse reactions during a therapeutic apheresis procedure.
Apheresis Nurses are nurses in Transfusion Medicine who are designated by this section for performing therapeutic apheresis procedures.
Medical Privileges are determined by Transfusion Medicine in conjunction with the medical privileging by the Medical Director.
Policy:
The referral physician will discuss the request for a therapeutic apheresis with the designated transfusion medicine physician. The referral physician must certify that the patient can tolerate the procedure based on his medical condition.
The transfusion medicine physician will review the patient’s clinical and laboratory data, with special note of the history of allergies, medications, previous transfusion reactions, and current vital signs.
Vascular access will be initially assessed by the apheresis nurse. Any questionable situations will be reviewed by the transfusion medicine physician.
The following laboratory values (less than 24 hours old) must be available before the procedure may begin:
CBC including platelet count
PT and APTT
Fibrinogen
Serum calcium
Serum protein and albumin
LDH for TTP cases
A valid type and screen must have been done within the previous three days of the procedure.
Upon review of # 2 through 5, the transfusion medicine physician will determine if the procedure is indicated and will communicate this to the referral physician, who will sign written order in the patient chart. Appropriate replacement fluids will also be mutually agreed upon in advance of the procedure and ordered by the transfusion medicine physician. The order specification must include:
Name of procedure and specification (e.g. therapeutic plasma exchange, isovolemic)
Replacement fluid type and volume (e.g. 3 liters 5% albumin, 2 liters, FFP, cryoprecipitate, normal saline)
Blood component orders if indicated (e.g. RBC exchange) and timing (before, during, and/or after the procedure)
Calcium replacement (e.g. 2 grams calcium gluconate IV in 100 ml normal saline to run during the procedure)
Any special laboratory testing post-procedure
The apheresis nurse will follow the orders of the necessary prescribed replacement fluids (FFP, albumin, PPF) in the quantities necessary for the exchange.
The referring physician will obtain the signed, informed consent from the patient.
If vascular access is unsatisfactory, the referring physician will obtain the proper access (central line, AV shunt, etc.).
The referring physician will arrange for a physician member of his team to be present at the actual therapeutic procedure. This physician designate will be responsible to treat any complications arising from the procedure.
Vital signs and weight will be obtained before starting the procedure.
If the procedure is outside an intensive care unit and the patient is critically ill, consider the use of a portable attached monitoring patch (such as the Umana UT1M device). The device will give alarm if any measurement is outside the defined ranges.
If any blood components are administered, keep the patch attached to detect TRALI/TACO and other adverse transfusion reactions.
When approved by the Blood Bank Director or designate with proper venous access and informed consent, the apheresis may start the procedure in the presence of the patient’s covering physician. The procedure will be performed in a designated hospital area.
The procedure must be documented on the appropriate therapeutic apheresis order and procedure worksheets.
References:
Standards for Blood Banks and Transfusion Services Current Edition, AABB, Bethesda, MD, USA
CAP Standard TRM.42245 regarding therapeutic apheresis procedures
It now has been over eight 8 months since I prepared the CCP workflow in Medinfo. It was built on the framework of the manual CCP process including donor prescreening with an abbreviated donor questionnaire. It was really quite simple and used the donor and patient modules to create quarantine areas for donor screening, collection, processing, and hospital patient blood bank release.
Here are my current comments on the process:
Donor Qualification:
I would still exclude malaria and HTLV from the donor questionnaire and would update to UDQ 2.1. Since these donors have recovered from a potentially life-threatening illness, I would keep the Hgb threshold at 11 g/dl.
Donor Collection:
In the future, I would consider using one of the soon-to-be-released portable devices that continuously monitor vital signs with pO2 and EKG lead to rule out asymptomatic pulmonary or cardiac problems.
I would also consider using low-ABO-titer, group A, universally to meet the demand for group B and AB patients.
Donor Testing:
There is still no need to segregate and separately test CCP donor specimens from regular blood donor specimens. I would perform SARS-CoV-2 antibody testing and set a threshold for qualifying donors—that threshold will be based on the manufacturer’s recommendations. However, if the treating physician wanted to use a low-titer unit, I would permit this.
Donor Processing:
There is no need to change this from the current processes. Keep the CCP processing separate from the regular operations.
CCP Plasma Release:
I would keep the quarantine release and restrict it to the locations used for treating COVID-19 patients
Medinfo Software Modifications:
I would record the IgG and IgM titers for SARS-CoV-2 antibodies in each donation record. This would include testing and entering the results on donations prior to this testing. ISBT labels should include this antibody titer.
Hospital Information Software Modifications:
Set up restricted CCP ordering for the actual treating physicians only. Also provide the ISBT code and shortened descriptors to it if necessary (certain HIS vendors still cannot read ISBT codes natively).
The original CCP workflow is attached for reference.
All blood components are considered medications and are subject to Good Manufacturing Practices as mandated by international accreditation standards. The whole process must be done reproducibly and precisely by specific personnel trained and documented to be competent. This includes collection of convalescent COVID-19 plasma.
Transfusion Medicine will provide staff who are deemed competent for the entire process of the collection, manufacture, and release of this unlicensed, emergency-contingency component.
It will help greatly if all candidates are prescreened to exclude the following candidates:
Administrative:
Donors must come with a valid Qatari identity card: no ID means no screening
Sex:
Males only to minimize the risk for transfusion-associated lung injury TRALI
Donor Feeling:
If the donor does not feel well, he should not come for screening/collection.
Food/Drink:
Donor must have eaten/drunk fluids within 4 hours of arrival for screening/collection.
Medication exclusions:
Antibiotics within the past 14 days
ACE inhibitors in the past 48 hours
Beta blockers
Anticoagulants
Anti-anxiety or other psychotropic medications
Other medications on the attached list
Medical exclusions:
Stable vital signs
History of seizures
History of dementia or other chronic neurologic disorder
Family history of dementia or other chronic neurologic disorder
Significant cardiac arrhythmias
History of hepatitis B, hepatitis C, HIV, brucellosis, Ebola
Travel history:
5 years cumulative residence in Europe including Ireland and France 1980-2001
3 months cumulative residence in the UK (and/or all its territories) 1980-1996
Any visit(s) to West Africa
This is NOT a complete list of criteria. Transfusion Medicine personnel will screen according to the full donor criteria. Thus, donors passing the pre-screening may still be otherwise disqualified based on the detailed process.
Setting up ABO-incompatible renal transplants is a major undertaking and requires close coordination between Transfusion Medicine and the clinical team. This post addresses my experience in setting up this program in 2019 at HMC in Qatar.
Like any process involving titration, it is best to automate it to minimize inter-technologist variability. Unfortunately, doing both IgG and IgM titers takes up to 1 hour per machine and totally monopolizes the machine during that interval. I did not have sufficient staff to even consider doing the titrations manually. Performing automated titers disrupted my workflow so I encouraged the clinicians to send the specimens for off-peak processing.
Titration:
Obtain the full clinical protocol and especially note the thresholds for transplantation.
Determine the methodologies used at the reference site. Can you do this at your local site or do you have to use an alternative method?
Do you have equipment to automatically titer? Doing both IgG and IgM may monopolize an immunohematology analyzer for one hour? How will this affect your other testing?
Regardless if it is the same method, you must still correlate your titers with the protocol site, both IgG and IgM.
If you are using multiple analyzers for titration, you must do a comparison study between them. How much does the titer vary?
Columns:
Determine column inventory and order the A, B, and AB columns. You must order enough to finish the course of treatment. It may take weeks to get additional columns, depending on your supply chain. Each column costs thousands of euros.
Where are you going to store the columns? Ours needed 2-8C storage. Can you keep them away from quarantined products and patient specimens?
Are your columns single-use?
If multi-use, who is going to restore them after use? How do you ensure that it is dedicated for the right patient?
Apheresis Equipment:
How are you going to attach the column to the apheresis equipment?
Will you use your therapeutic apheresis equipment like Terumo Optia directly or will you use a second machine (e.g. Medicap)?
Do you have all the clamps, tubing, and holder for the column?
Staffing:
Do you have sufficient apheresis nurses to perform the procedures? You may be running the apheresis for up to 8 hours. How does this impact your other procedures or donor center operations? Our pool of apheresis nurses was very limited. They also covered routine blood donation. How will doing this process impact your regular donation and other apheresis operations—donor and therapeutic?
Do you have sufficient supplies of ACD-A anticoagulant and calcium gluconate?
Specimen Collection:
Perform titrations expeditiously: Can you finish titration testing before the next scheduled procedure? In our institution, we collected specimens at 0400 and had them directly brought to the blood bank for testing. Results were ready at 0600 so the clinicians could decide early if another procedure was needed.
Table of Permissible ABO Types:
Define acceptable blood products by blood type—take into consideration pathogen inactivation and platelet additive solution if used. At our institution, all RBCs were in additive solution and all platelets were pathogen-inactivated in platelet additive solution PAS so residual ABO antibodies were minimal in the final components. Since the platelets contain only minimal plasma, we did not concern ourselves with matching their ABO type with the donor kidney. Otherwise, platelet types with plasma compatible to the donor kidney must be selected.
Software:
Prepare a truth table for acceptable ABO component types based on #16 above.
Include the titer cutoff for IgG and IgM antibodies in the organ transplant module.
Selection of blood component for ABO-incompatible renal transplantation is discussed in a separate post that will follow.
I am attaching the US Center for Biologics Evaluation and Research CBER Guidance for Industry revision dated December 2020 to replace the one issued in September 2019.
This is a very detailed document that will require US blood centers to comply with newer more stringent safeguards to minimize the risk of bacterial contamination of platelet components.
The easiest way to comply is to universally pathogen-inactivate all platelet components: then the rest of the algorithm does not apply. I am happy that for over 10 years I have used pathogen-inactivation (riboflavin-based Mirasol, Terumo BCT) and not experienced any bacterial sepsis from platelet or plasma components.
For those of us practicing outside the USA, please note:
The US still does not permit pooled, buffy coat platelets to have either a 5 or 7 day outdate. For pooled components stored at 20-24 C, the FDA only allows a four-hour outdate, regardless what the rest of the world permits. Thus, the USA mainly uses apheresis platelets.
If you have pathogen-inactivated platelets, you are so fortunate that you don’t have to follow these other recommendations to have a low risk of bacterial contamination.
Reference:
Bacterial Risk Control Strategies for Blood Collection Establishments and Transfusion Services to Enhance the Safety and Availability of Platelets for Transfusion, Guidance for Industry, U.S. Department of Health and Human Services, Food and Drug Administration, Center for Biologics Evaluation and Research, September 2019 updated December 2020
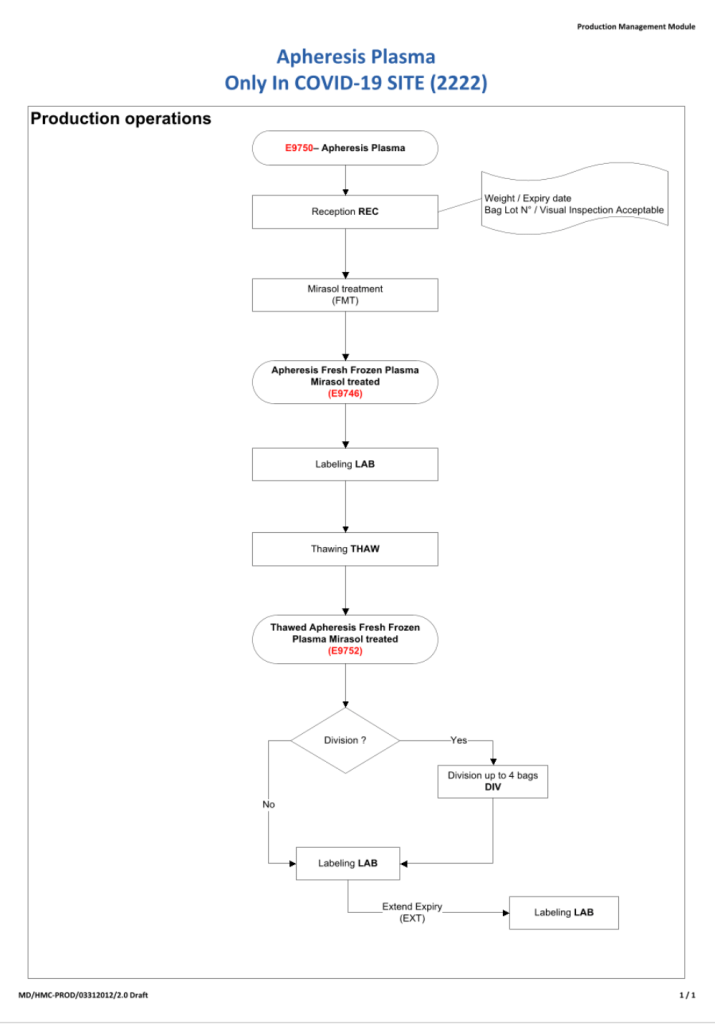
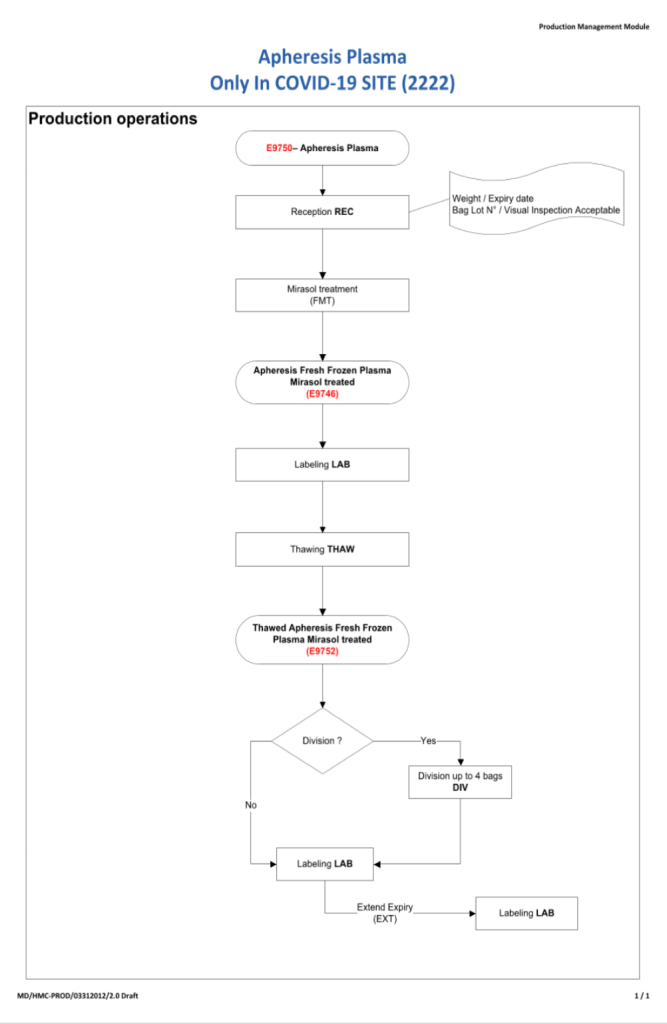
I will be posting a detailed series about the manual and software-enhanced COVID-19 processes that I set up in Qatar at HMC Doha in March-April 2020.
In this series I will provide you with screen shots of my Medinfo Hematos IIG software design for each step in the process: collection, processing, testing, inter-depot transfer, and hospital transfusion service/blood bank release.
This GMP-compliant software-enhanced system is based on the manual system I set up in early March 2020 at HMC.
I want to thank Medinfo Hematos IIG for their rapid response to building this parallel system based on my standard processes in so short a time (two weeks) and my special thanks to the software engineering team at Vital Health Technologies, the agent for Medinfo in Qatar.
To start the series, I am providing the basic workflow for the system. As is normal in Medinfo software design, a full mapping of the processes are made. This workflow shows the new CCP ISBT codes and the quarantine collection and processing steps. The donor testing (marker and immunohematology) processes are similar to those for regular donor units.
This is basically the same process both manually and in the software. I always say:
A good software process is based on a good manual process!!
Please note the following workflow for our initial discussion.