The Division Head, Transfusion Medicine and Blood Banks, is responsible for all aspects of transfusion medicine at HMC for the State of Qatar. The following policy documents some of those roles.
Policy:
The Division Head, Transfusion Medicine HTM, serves as a member of the Corporate Transfusion Committee
The HTM through the CTC establishes criteria for transfusion of blood components and passes these through the HMC corporate process for establishing official guidelines.
The HTM reviews blood component requests, especially in times of shortage to triage in conjunction with the Medical Director and Chairperson, DPLM
The HTM establishes transfusion practices through the interim policies, which are in turn used to prepare processes and procedures through corporate transfusion medicine.
The HTM serves as Project Manager for the Medinfo Hematos IIG computer system and prepares policies, processes, and procedures for Transfusion Laboratory Information Systems.
References:
Standards for Blood Banks and Transfusion Services, Current Edition AABB, Bethesda, MD, USA
I have had many medical students, residents, and fellows rotate through my Transfusion Medicine section. Hardly anyone has any interest in making my discipline his/her career. It is a required rotation or an “easy” rotation during which the trainee may take his vacation. The trainee will cram for the examination and then promptly forget it.
I left practice in the USA in 1990, in what I consider the golden age of laboratory medicine. We had supervisors for each laboratory section. In the blood bank, we had many staff with SBBs or who were SBB students. We were very self-sufficient in handling immunohematology problems except for rare blood types or antibodies to high incidence/prevalence antigens.
When I returned to visit my old laboratory, I sensed a deprofessionalization of the laboratory and blood bank in particular. Blood Bank now is a cost center, not an area of revenue. Why hire experienced blood bankers for most hospitals? Send the antibody workups to the Blood Center. There are limited jobs for transfusion medicine consultants. Minimize testing, don’t do extended antigen typings, etc.
Nowadays, I feel like one of the dinosaurs marching into oblivion like in Walt Disney’s Fantasia film, the section called The Rite of Spring. Who will replace those retiring? Have you ever noted the average age of attendees at the AABB annual convention? I feel young when I go there (and don’t worry about the gray hair!)
I want to attract new doctors and scientists to Transfusion Medicine. I really try, but most have no interest and look on their rotations as a necessary evil.
I have lowered my expectations for most medical trainees in Transfusion Medicine. They don’t like it, they just want to pass it, and move on. What must I impress them with for their future careers?What is essential for them to remember?
I have had both pathology and non-pathology trainees. Surgical and ob/gyn doctors used to spend one month whereas the hematology and pathology residents/fellows spent on average three months. The few interested in the field might do multiple rotations.
I still gave them lectures on a variety of topics, especially how to transfuse blood components, basic ABO/Rh antigens, compatibility testing, and direct antiglobulin testing. They would forget most of this, but I wanted them to remember TURN-AROUND-TIMES:
Examples:
HOW LONG DOES IT TAKE TO PERFORM THE TEST? TO FIND COMPATIBLE BLOOD? TO THAW THE PLASMA? RELEASE AN MTP SHIPMENT? TO PERFORM A TRANSFUSION REACTION WORKUP BEFORE RELEASING MORE BLOOD?
I am not discouraging people from entering the field, but I am a realist to know that few will share my passion for serology or want to take call on difficult immunohematology cases. At least if they understand the pressure the technical staff are in and these turn-around-times this will make both their work as clinicians and mine as transfusion medicine more congenial.
Sometimes, you may not have adequate resources for a project so you will consider hiring an outside consultant. During my career, I have used several outside consultants for projects ranging from installing a new general laboratory computer system to assisting in getting international accreditations.
Regrettably, my experience with software consultants has been mixed. I have used them for general laboratory software installation and settings. Very few have any experience with dedicated blood bank software or setting up hospital blood bank modules. They are often former employees of the software vendor you are using. There is always a potential for conflict of interest.
The software consultant must work for you, NOT for the vendor you are using. He/she must maintain his independence from the vendor and only represent your interests. I have had many problems with this. Here are some of my unpleasant experiences:
Current and Future States:
One set of consultants gave essentially the following current state mapping for almost every test in our menu:
Order this.
Collect this.
Receive this.
Perform this.
Release this.
They did not know our current state so they were unable to help us build a proper future state.
Mapping Errors:
The consultants were in charge of exporting results from a previous system into the new one, this included mapping the results into the appropriate test fields. They assumed it would map properly, I insisted on testing a two-week sample of laboratory results and discovered major errors that could adversely affect patient care—it was a major disaster and almost held up implementing a hospital go-live on-time.
Benefits of New Software:
The consultants were obsessed with calculating benefits of the conversion to the new software vendor and making fancy PowerPoint presentations to assure officials that they were gaining benefits. There were many issues to resolve that were critical to the functionality that I felt the time would have been better spent in fixing the software issues than calculating alleged benefits.
The Need for Speed:
There were some consultants without any experience in blood bank who insisted that this had no bearing in making software settings. One bragged to me that he could install a blood bank system in a few days.
Default Settings:
Some outside consultants kept pushing using the default settings. There is no “one size fits all” solution for a large healthcare organization. There is need for customization. I wondered why we needed the consultants to set up default settings which is what the vendor wanted us to do anyway.
Sometimes, you may not have adequate resources for a project so you will consider hiring an outside consultant. During my career, I have used several outside consultants for projects ranging from installing a new general laboratory computer system to assisting in getting international accreditations.
For a complex accreditation process such as AABB, I have used such consultants to audit operations in the donor center including processing and testing, hospital blood banks, and stem cell laboratory. They are high-level technical specialists with highest blood bank qualifications (e.g. SBB(ASCP) or equivalent) and have considerable experience in practice of blood banking and quality systems. They have been AABB Assessors so they can give you a dry-run accreditation assessment.
Depending on the project, you may need one or a group of consultants. I have worked with both individual consultants and groups. A group can complete the tasks quicker but this is not always necessary. Organizations such as AABB have many different consultants with different types of expertise so you can select the most appropriate individuals to form a team for your needs.
These specialists can audit your operations and propose a model and if you want, actually help you to implement the processes. They can help you with the accreditation formalities, especially if you do not have any staff with experience in the process. It all depends how much you can spend.
In the Middle East, to bring in such consultants may mean expensive air fares, hotels, meals, plus the actual costs of doing the consulting. This is a major investment for your organization but it is well worth it to expedite the process. There are local consultants available as well and using them may greatly help with the expenses.
Although it is expensive upfront, it can be cheaper in the long run by establishing the appropriate framework in the first place. You can engage the consultants to actually do much of the work themselves, but it is better for them to offer a train thetrainerexperience, i.e. engage your own technical staff to learn new skills and then have them cross-train the rest of the staff.
Based on the findings, your local staff can implement the changes. You can then consider rehiring the consultants to verify that the work has been done properly.
I have used both individual consultants and groups through AABB Consulting. My staff and I have learned much from such interactions, and I highly recommend their use when local expertise is not available.
Super-Users: Engaging Laboratory Staff in Computer Operations
This is an update of a previous post.
It is critical to engage the technical, medical , and (blood bank) nursing staff in this process, That is why it is so important to identify a core of computer-literate users to help with the building and testing/validation.
I don’t mean finding staff who can already program or code. Rather, I mean staff that are astute with knowing their work processes and who had good skills with Microsoft Office and Windows or equivalent. I did not expect them to understand database structure or use structured query language. They were chosen for their ability to learn quickly and their meticulousness.
For our blood bank system, I chose computer-literate technical staff to be involved in the build from the very beginning. They learned how to test each module and to some degree support it. These became my Super-Users and to this day support the system for many tasks. These staff served as the system administrators and worked directly with me as the Division Head for Laboratory Information Systems. They were not full-time and still had their other clinical/technical duties. They liaised with the software vendors engineers.
Our blood bank system was NOT a turnkey system. It was custom designed according to our workflows. There were NO default settings!! We had to be remember, ‘Be careful what you ask for, you might get it!’ In some countries, approved systems are turnkey and may allow only few changes to the core structure and thus may not be this optimized for the needed workflow; often only cosmetic changes are permitted.
When we built our first dedicated blood bank computer system, the company would take a module and completely map out the current processes collaboratively with me. After this, I analyzed the critical control points and started to map out the improved computer processes that would take over. After that we would build that those processes in the software and test it. If it failed, we would correct it and test again…and again if necessary. Fortunately, the blood bank vendor did not charge us when we made mistakes.
Sadly, another vendor (non-blood bank), only gave limited opportunities to make settings. If wrong, there might be additional charges to make corrections. This other vendor really pushed the client to accept the default settings regardless whether or not they actually fit. End-users were selected to make and approve the settings, but they were only minimally trained on how to make the settings. It was a journey of the end-users being led to the slaughter—and being blamed for their settings when they accepted the vendor’s recommendations—they usually selected the defaults. There wasn’t enough time for trial and error and correction.
The blood bank system Super Users were an important part of our process. They were an integral part of the implement team and could propose workflows, changes, etc.—subject to my approval. They learned the system from the start and developed invaluable skills that allowed them to support the system after the build. Also, they could serve to validate the system according to the protocols I prepared. Moreover, I took responsibilities for their activities and they were not left out to hang.
Every hospital blood bank location and the blood donor center had Super-Users. These included:
Blood Donor Center:
Administrative Clerk for donor registration, consent, ISBT specimen labels, creation of new donors and patients for validation purposes
Apheresis/Donor Nurse for donor questionnaire, donor physical examination, and donor collection
Medical technologist for donor marker testing
Medical technologists for blood component production including Reveos, Mirasol, platelet additive solution, pooling, and leukodepletion
Medical technologist for donor immunohematology testing
Medical technologist for inter-depot transfer of blood components
Hospital Blood Banks and Transfusion Centers:
At least one technologist at each site for inter-depot transfer, component medication (washing, irradiating, aliquoting, reconstituted whole blood), immunohematology testing, component allocation and release
The cost of using these staff? They were paid overtime and were relieved of other duties when working on Super User duties. This was much cheaper than hiring outside consultants who may or may not know our system well enough to perform these tasks.
By having a Super User at each site, I in effect had an immediate local contact person for troubleshooting problems who could work with the technical/nursing staff. We did not rely on the corporate IT department for support and worked directly with the software vendor. Response time was excellent this way.
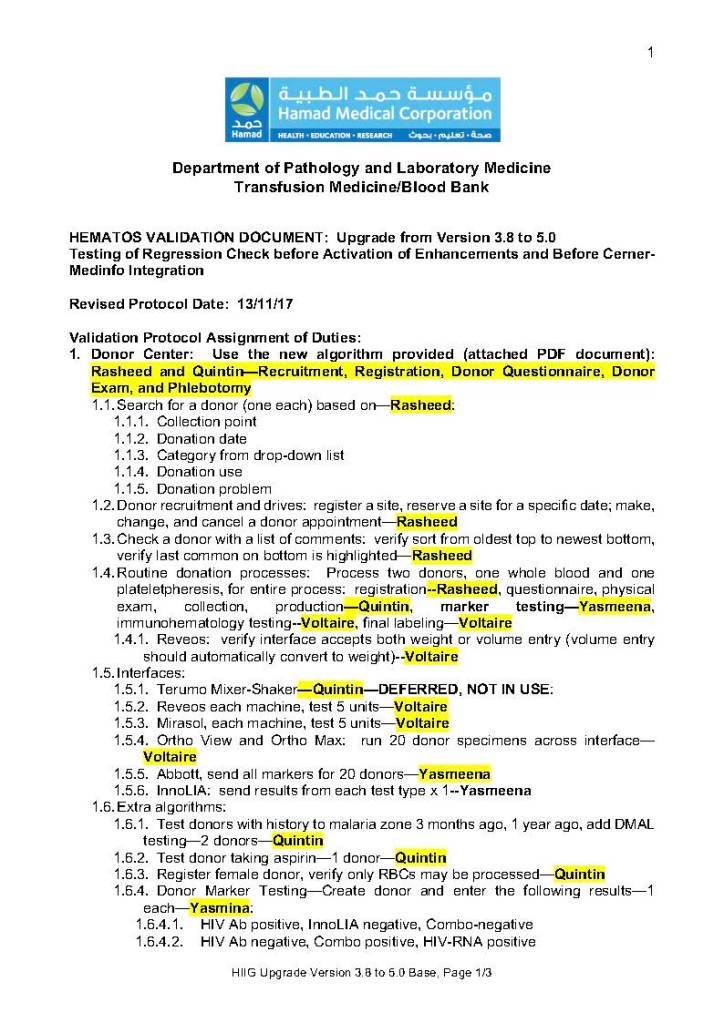
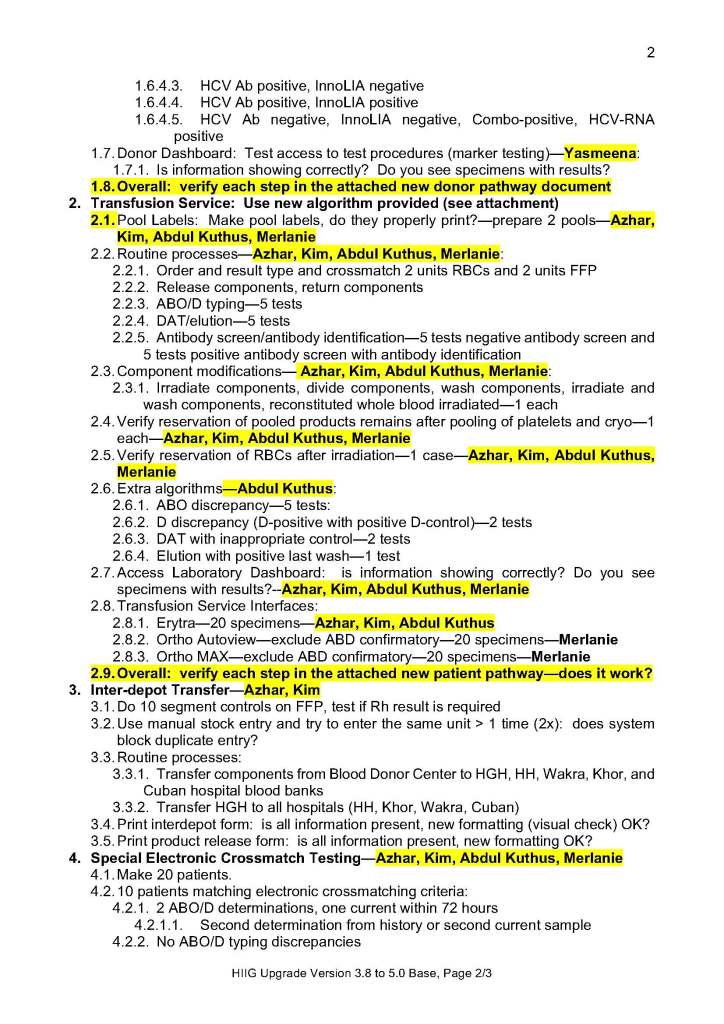
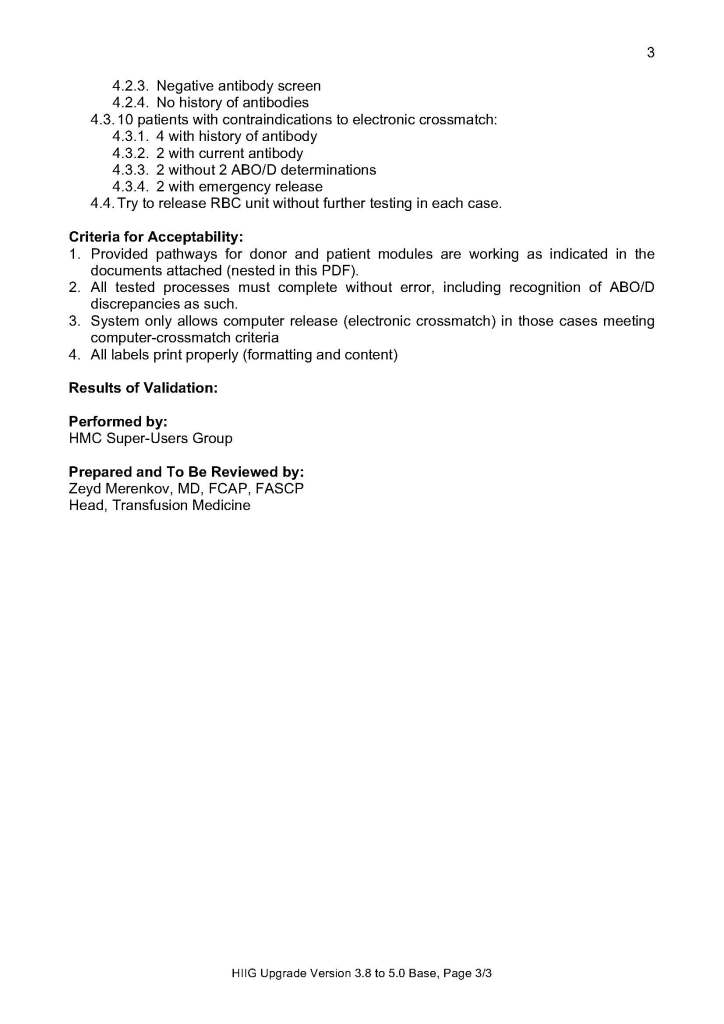
The following document is a sample document of the assigned Super User duties during a validation.
All policies, processes, and procedures must comply with local, national, and applicable international accreditation standards (i.e. AABB, CAP, ISO, and JCI).
All recruitment information must be entered into Hematos IIG.
The Coordinator, Donor Affairs, is responsible for all recruitment activities.
Donor recruitment staff will visit scheduled donation sites in advance and assess their suitability and prepare them for use before the start of each campaign.
Donor recruitment materials and announcements will be left at each location during the inspection visit.
Collected blood will be stored at room temperature during the collection on-site and transported back to the Donor Center in suitable validated containers to maintain storage at desirable temperature.
The processes and procedures for normal donation, e.g. registration, donor questionnaire, physical examination, and collection apply.
References:
HMC 1001 Setting Specification, Version 1.5, Hematos IIG, Medinfo
Standards for Blood Banks and Transfusion Services, Current Edition, AABB, Bethesda, Maryland, USA