This version updates a previous to include a remote monitoring device GPI Umana T1 to increase detection of these complications.
This version updates a previous to include a remote monitoring device GPI Umana T1 to increase detection of these complications.
Principle:
This is the latest update on donor qualifications during the COVID-19 pandemic and addresses issues about COVID-19 vaccination, COVID convalescent plasma use and donation, return of donors into the donor pool after COVID-19 vaccination. All of this information is subject to change as new regulations are released.
Policy:
References:
This is a teaching document I give to new staff, medical technology students, pathology and residents. Very often I get the question, “Why can’t I just do the antiglobulin phase crossmatch first and then phenotype the RBC unit?” Or: “Why do I have to add reagents in a particular order?”
My practice has always been to select an antigen-negative RBC unit first, then do the antiglobulin-phase AHG crossmatch. This way I know that the unit was definitely phenotyped before release. Likewise, the blood bank computer now only offers antigen-negative units for allocation and then crossmatching if there is a clinically significant antibody.
In a manual setting without a blood bank computer system, performing the AHG crossmatch may yield a negative result, even if the unit is antigen-positive. With storage, some antigenic expression is weakened so it may not be detected at the time of crossmatch. Yet, there may still be enough antigen present to cause hemolysis. Not detected does not necessarily mean not present!!
I expect that many inexperienced staff may be tempted to forego the antigen typing if the AHG crossmatch is negative.
This is an analogous logic to the question, “Do I add the cells or the antiserum/plasma/serum first for the reaction?” If you add the cells first, you may forget to add the patient’s plasma/serum or a typing antiserum and you might not be able to detect the omission by looking at the tube or gel. Actually, I once recommended to one vendor that it color the typing antiserum so it was conspicuously showing on the gel.
I was taught that this is a matter of discipline to ensure that all steps are performed.
However, for every practice, there has to be flexibility. If there is no typing reagent or if it is very expensive or in short supply, one may have no choice but to do the AHG crossmatching first. Often there is still another option: one can often preliminarily screen units first before using a rare reagent—examples:
In an ABO-incompatible stem cell transplant, both donor and recipient RBC types may be present. Likewise, immune effector cells from both the donor and recipient may be present.
Using group O RBCs and AB plasma is an option but there are limited supplies of both. Since we use RBCs in additive solution (SAGM), only minimal residual donor plasma is available and unlikely to be clinically significant.
Here is my approach:
In a massive transfusion setting, the patient’s forward and reverse type will reflect the use of group O RBCs and the patient may even fully type as group O, depending on the number of units transfused. Group O RBCs are very precious and in short supply so we need to switch the patient back to his/her own type as soon as feasible. RBCs in additive solution (e.g. SAGM) have only minimal residual plasma so the load of anti-A,B from the O cells is minimal. In my organization, we did not titer ABO hemolysins in blood donors.
Here is my approach:
Some people would recommend performing a full AHG crossmatch using the patient’s current plasma and RBCs of the original ABO type:
I did NOT do the full AHG crossmatch and had no hemolytic transfusion reactions if the RBCs were compatible with the current reverse type plasma.
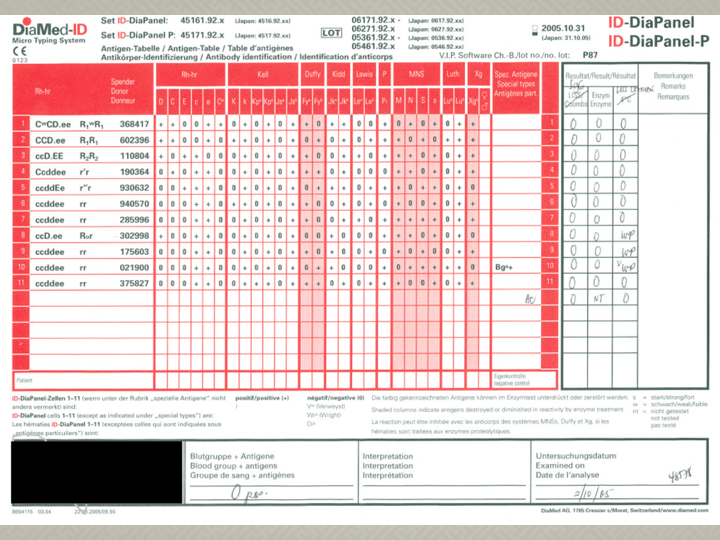
This is an updated version of a lecture I gave in 2010 to a Saudi Ministry of Health blood bank meeting on this topic. It may still be useful as a teaching document.