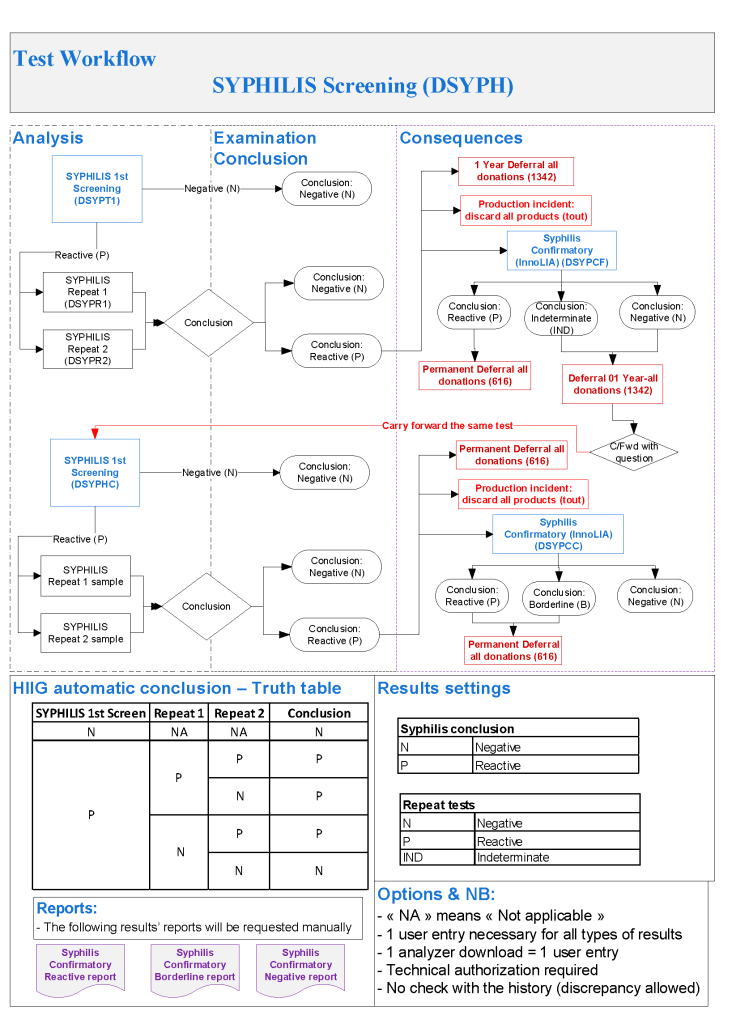
Syphilis testing uses a screening test (we used an EIA methodology to detect cardiolipin) and a confirmatory test a syphilis linear immunoblot assay LIA.
I emphasize that any test methodologies and testing algorithms can be designed in Medinfo. This is what I selected during the time I was HMC Doha.
My algorithm specification was:
Syphilis Testing:
Syphilis Ab test positive or indeterminate: do InnoLIA-Syphilis test
InnoLIA-Syphilis test positive: permanent deferral, refer to Infectious Disease clinic
InnoLIA-Syphilis test borderline or negative: defer for 1 year, then repeat all syphilis testing.
Repeat Syphilis Testing after 1 Year:
Syphilis antibody testing negative, reenter into donor pool
Syphilis antibody positive or borderline: do InnoLIA-Syphilis test
InnoLIA-Syphilis test positive: permanent deferral, refer to Infectious Disease clinic
If InnoLIA-Syphilis borderline or negative: permanent deferral, syphilis not confirmed
This was translated into Medinfo processes as follows:
As a transfusion medicine physician, I must know if I can trust my staff’s interpretation of immunohematology testing. I may be called at night and they will provide me with results and I must use these to make a medical judgment. If their interpretation is flawed, I might make a decision that harms the patient.
I really don’t like multiple-choice questions, but nowadays this is often the norm. For my staff, especially senior staff and those who want to be promoted to senior staff, I have developed a series of projective exercises to help me understand their thought processes.
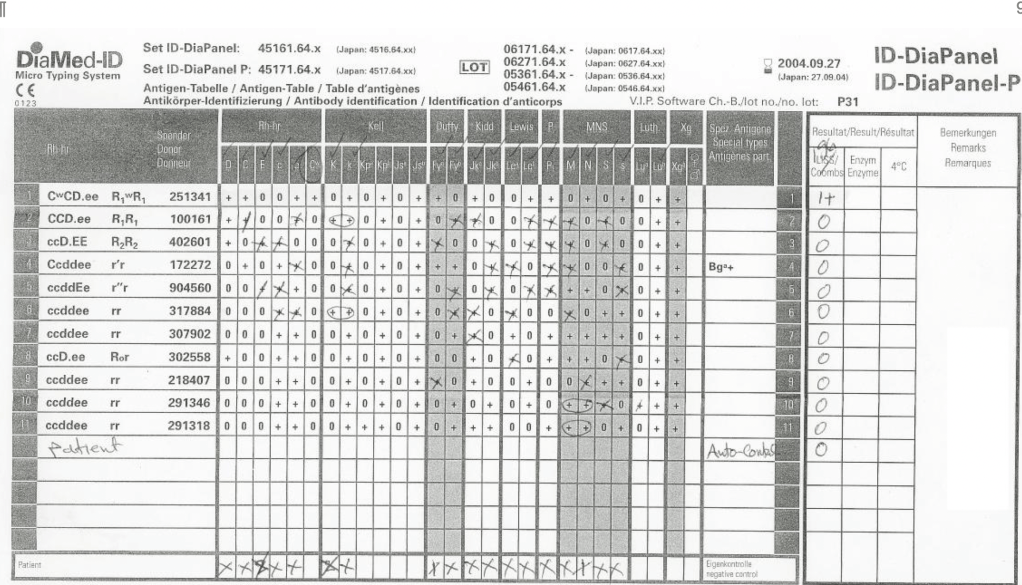
Here is a sample exercise. I have the staff review this panel and tell me to interpret it:
Most of them answer that this is an anti-Cw without hesitation. However, they are basing that on only one Cw-positive cell.
More astute ones indicate it might be anti-Cw but ask to test additional Cw-positive cells and perform an enzyme panel. These are the ones that I will consider for promotion now.
This is an updated job description of what I used at NGHA Riyadh for a Systems Administrator for laboratory software. Such a person will have software privileges as agreed by the hospital information systems department. In our system there, there was a separate laboratory information systems section LIS:
Basic Function:
To analyze laboratory databases and prepare reports to optimize laboratory utilization and management
Principal Duties:
Maintains and secures the laboratory information server (to be distinguished from the LIS hardware) and its associated databases
Uses downloaded database files from laboratory computer system to prepare reports as deemed necessary by and as prioritized by the Pathology Chairman, Laboratory Operations Administrator, and/or Portfolio Head, LIS, which may include but is not limited to:
Cost containment (implementation of CEO directives)
Internal laboratory and external hospital committees (as requested by them)
OVA statistical analysis
Specimen referrals to outside laboratories
Specimen referrals from other hospitals or hospital systems
ER Stat Laboratory utilization reports
Laboratory Utilization Committee, including STAT turn-around-time and critical values
Quality Improvement-Accreditation Portfolio
Test utilization metrics
Any other reports requested/approved by the Portfolio, LIS, Laboratory Operations Administrator, and/or Chairman
Assists in the management of the document control program for the laboratory
Assists in the management of the intellectual property control program for the laboratory
Performs any other assignments as directed by the Pathology Chairman, Laboratory Operation Administrator, and/or Portfolio Head, LIS
Essential & Preferred Education & Experience:
B.S. degree or higher in computer science including coursework in networking, database structure, and management
Experience (at least two years) in operating enterprise-level (e.g. Oracle, IBM DB2), business-level (Postgresql, MySQL, Microsoft SQL Server) databases as well as Microsoft Access® desirable
Fluency in English (high-level) essential, fluency in Arabic desirable
Experience (at least one year) in working with databases in a variety of operating systems (Win32/64, Linux, UNIX) desirable
Experience (at least one year) in working in a hospital laboratory environment desirable, not necessarily as a laboratory technologistLa
Must be self-reliant and disciplined to operate independently and have excellent organizational and interpersonal skills to relate to a wide variety of laboratory and hospital personnel
Degree of Responsibility:
This is a middle-level management position within the Department of Pathology and Laboratory Medicine. The analyst must be self-reliant and disciplined to operate independently, have excellent organizational and interpersonal skills to relate to a wide variety of laboratory and hospital personnel.
In my long career, there have been cycles in transfusion practice. Today’s dogma becomes yesterday’s heresy and then later again the dogma. Just consider the selection of blood components before the introduction of cyclosporine for intended renal transplant recipients.
In training, I was told NEVER, NEVER use the intended donor’s blood for the renal recipient. This would immunize him against the donor tissue antigens and cause the transplant to fail.
Several years later after cyclosporine, we were doing a booming business of directed RBC transfusions from the donor to his/her recipient.
Just a few years ago, I used blood component therapy for all, especially trauma patients. Give the victim what he lacks: for oxygen-carrying capacity, RBCs; for volume crystalloid; for low protein albumin; for coagulopathy FFP, factor concentrates, cryoprecipitate; for thrombocytopenia, platelets.
Most recent studies now mention the danger of giving too much crystalloid, etc. It talks about using fresh whole blood to provide all of the above in less volume. Results from trauma and military studies are encouraging and may be better than individual component therapy.
There are special considerations for whole blood:
21-day outdate for the RBCs
Platelet functionality limited after 7 days
Use of group O, low-ABO-titer
Pathogen-inactivation of whole blood is CE-approved by riboflavin (Mirasol). Terumo BCT is developing an exciting technology to first use Mirasol and then make components using the Reveos automated component system—RBCs, plasma, and platelets. This is an ongoing project so for now the only CE-approved project is use as whole blood. Such Mirasol-treated whole blood has been shown to prevent malaria transmission in Ghana.
From my review of the literature, these are my specifications as of this date 18/8/20:
Use/ordering restricted to trauma and selected ICU/surgery suites
Only male donors
7 day outdate
Group O, Anti-A and anti-B IgM titers, both <= 1/256
Leukodepleted < 1E6 residual WBCs
What level of anti-A and anti-B titers is acceptable? The titer was set as low as 1:32 but at recent THOR meeting 1:256 has been used. In Qatar in a pilot study, I found that about 50% of our donors had titers < 1:256. The issue is that each time the donor presents himself/herself, we must repeat the titer—it is not stable.
Of course, performing even just a saline-titer is time consuming. The only practical way for us in Doha would have been to use an automated titration option on an immunohematology analyzer—in our case, the Ortho Vision MAX, which could perform 1 titration run in about 30 minutes, and the instrument cannot be used for any other testing during the process.
I personally would perform leukodepletion to conform to CE, but you need a special whole blood filter that removes WBCs butspares the platelets. Terumo BCT has such a filter that achieves <1E6 residual WBCs. Never use a standard RBC leukodepletion filter since it will remove BOTH platelets and WBCs—this would defeat the purpose of using whole blood.
At HMC Doha, female donors were only used for packed RBC production—all plasma and platelets were discarded. Some centers do HLA antibody screens and allow negative females to donate.
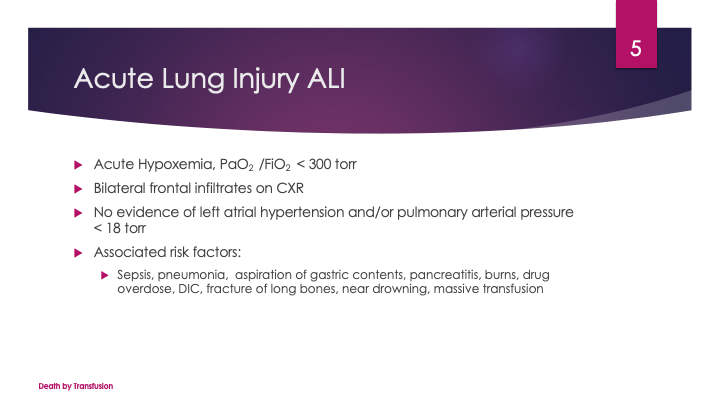
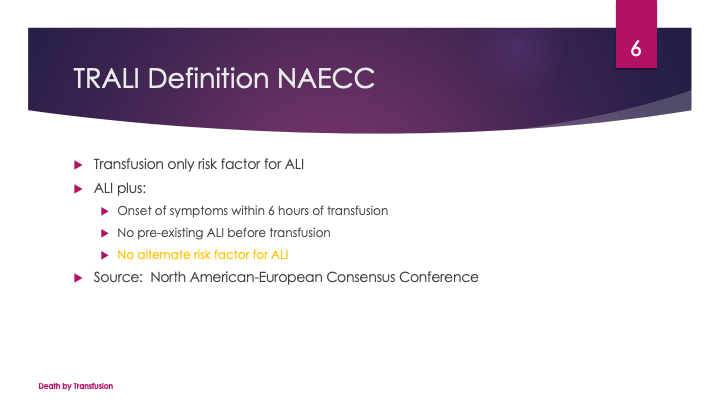
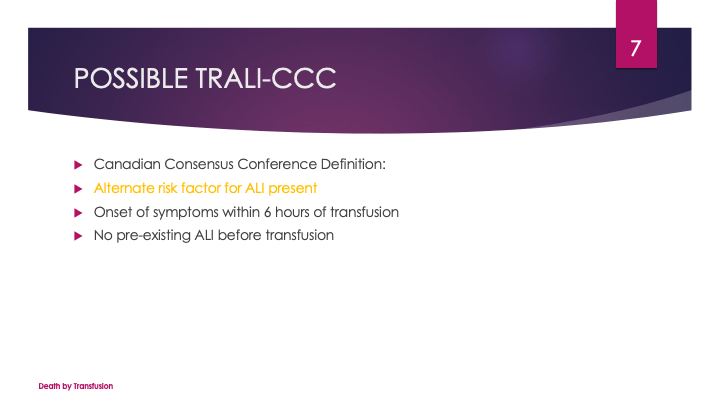
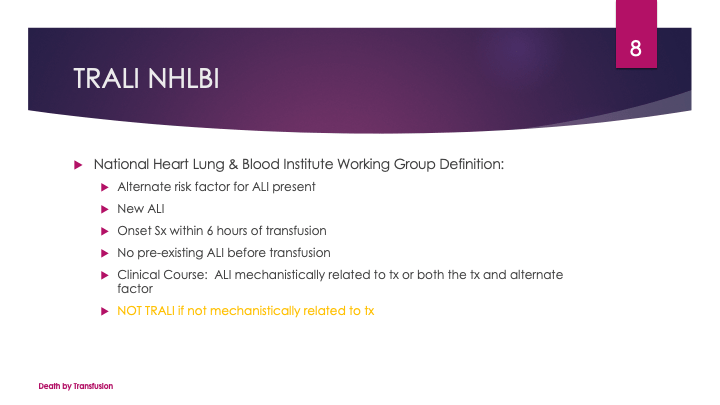
Finally, many groups do not leukodeplete at all. I am concerned about the risk of adverse reactions and TRALI so I would conform to CE and do it.
Whichever conditions you stipulate, it is easy to create the process in Medinfo. The most important thing is to know what you want to specify.
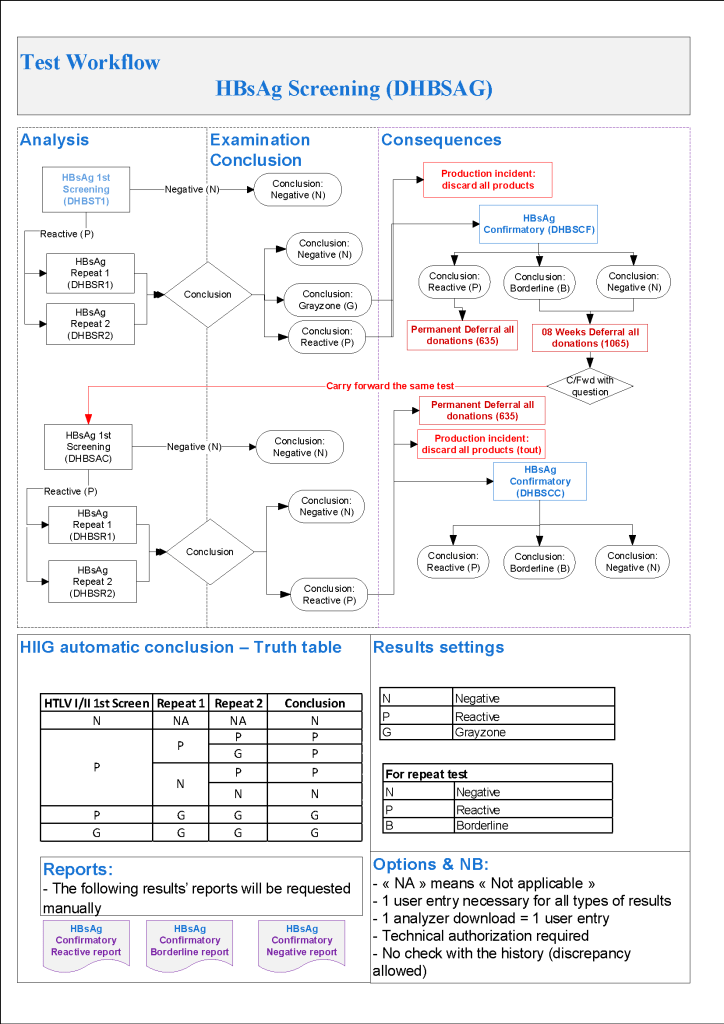
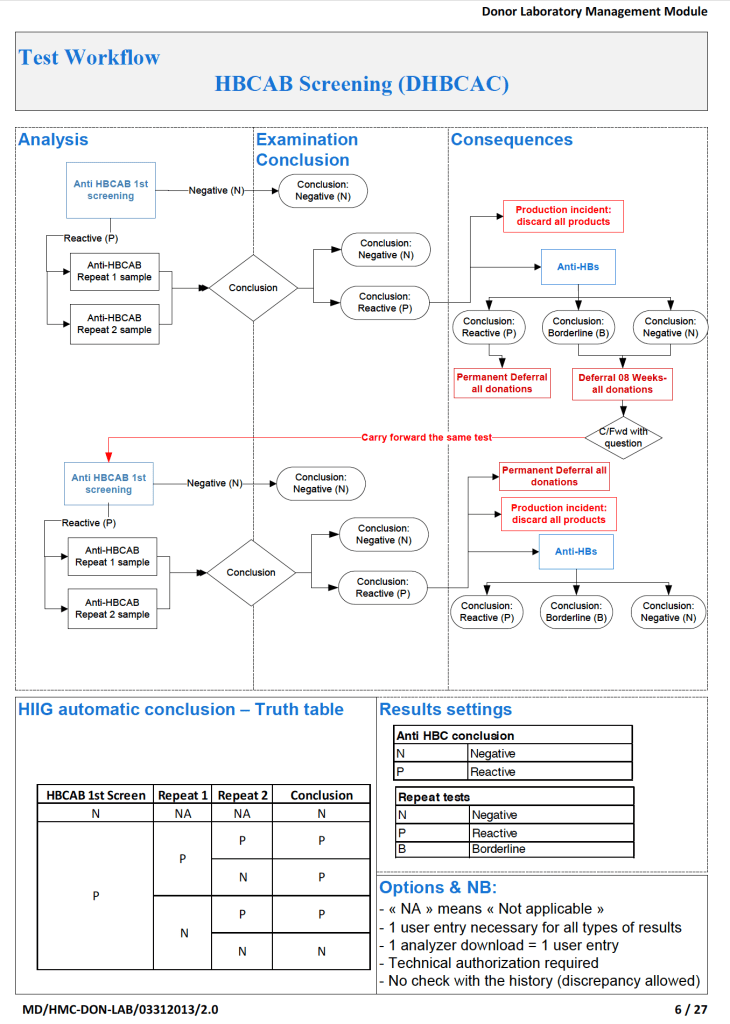
Hepatitis B donor screening consists of HBsAg and HBcAb for all donors, the latter to detect the window period. In the USA, a non-negative HBcAb result will trigger a deferral. In the Gulf area/KSA, there HBV was positive higher than in the West so there was a high rate of HBcAb positivity often from recovered HBV infection.
Here was my last algorithm before I left HMC Doha, which allowed use of donors with protective titers of HBsAb. Note that the WHO cut-off for this is 10 IU/L whereas we used 100 IU/L as our threshold:
Hepatitis B:
HBsAg non-negative, then:
HBsAg positive with HBsAg confirmatory positive, regardless of other results: permanent deferral, refer to Infectious Disease clinic
HBsAg positive with HBsAg confirmatory borderline or negative, repeat all HBV testing after 8 weeks
HBsAg borderline: repeat all HBV testing after 8 weeks
HBV-DNA positive confirmed, regardless of other results: permanent deferral, refer to Infectious Disease clinic
If HBcAb positive, repeat after 8 weeks
Repeat Hepatitis B Testing After 8 weeks:
HBsAg positive with HBsAg confirmatory positive: permanent deferral, refer to Infectious Disease clinic
HBsAg positive with HBsAg confirmatory borderline or negative: permanent deferral, refer to Infectious Disease clinic
HBsAg borderline, permanent deferral, refer to Infectious Disease clinic
HBV-DNA positive confirmed: permanent deferral, refer to Infectious Disease clinic
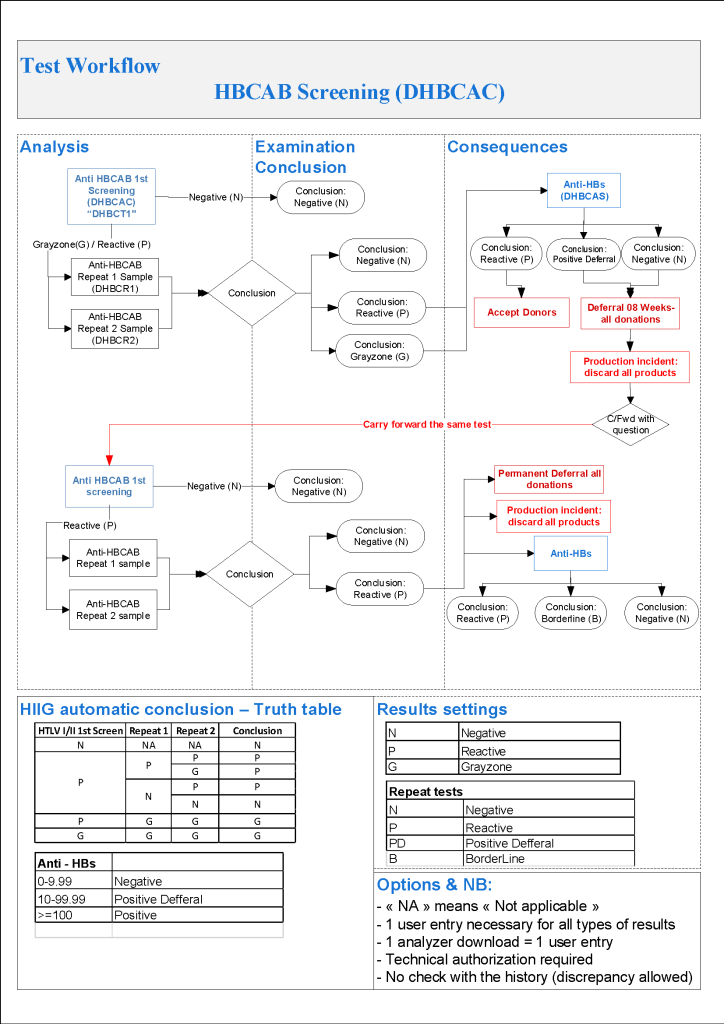
HBcAb positive or borderline with negative HBsAg and negative HBV-DNA: review HBsAb level:
If HBsAb level >= 100 mIU/mL (100 IU/L), donor may be reentered
If HBsAb level < 100, then recommend to donor to receive booster HBV vaccine
After HBV vaccine administration, retest after 30 days:
If HBsAb level >= 100, donor may be reentered
If HBsAb level < 100, donor is indefinitely deferred
HBsAg, HBcAb, HBsAb all negative: reenter into donor pool
Here is the HBcAb and HBsAb part of the algorithm:
Previously, we had we had disqualified any donor with a nonnegative HBcAb:
This is an updated version of a presentation given to the Saudi MOH several years ago. I have included statements about pathogen inactivation and platelet additive solution which were not used on the original date.
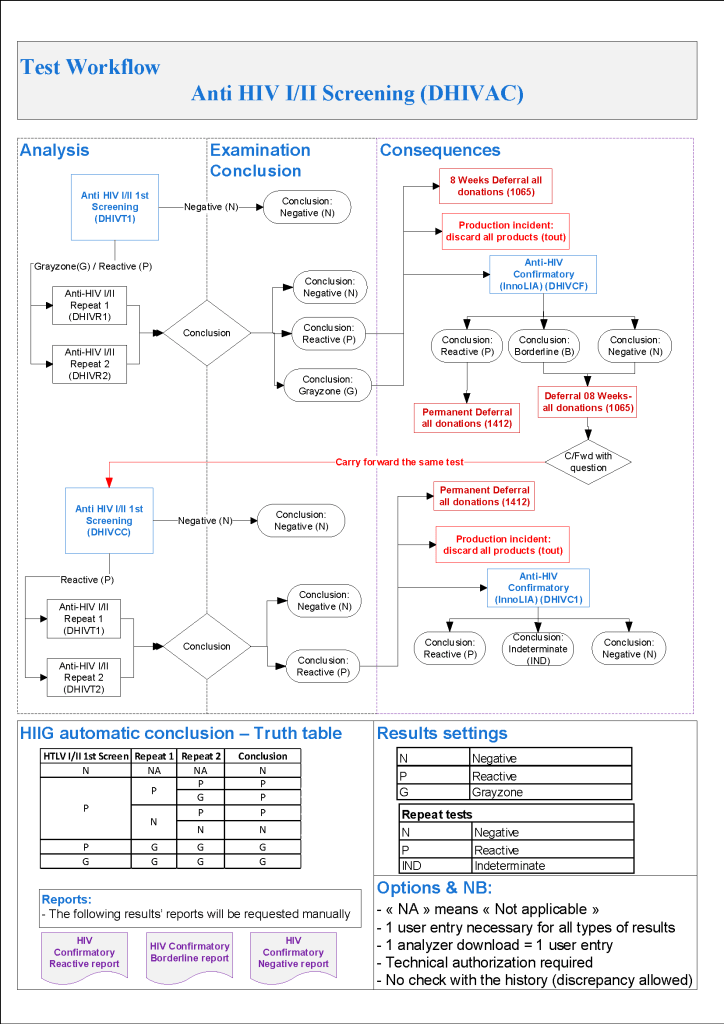
As I designed this in Medinfo, this is algorithm uses an HIV- /HIV-2 antibody EIA screening test, HIV p24 antigen test, and a confirmatory linear immunoblot assay LIA that can discriminate between type HIV-1 and type HIV-2. If there is an indeterminate result, a repeat test is ordered after 8 weeks. A reentry protocol is also included (1.6.3 below).
HIV Testing:
HIV-RNA positive confirmed, regardless of other HIV results: permanent deferral and do HIV-InnoLIA, refer to Infectious Disease clinic
HIV-RNA borderline: do HIV-InnoLIA
HIV-InnoLIA positive, regardless of other HIV results: permanent deferral and refer to Infectious Disease clinic
HIV-InnoLIA indeterminate: repeat all HIV testing after 8 weeks
HIV Ab positive with negative HIV-RNA and/or borderline/negative HIV-InnoLIA: repeat testing after 8 weeks
Repeat HIV Testing After 8 Weeks:
HIV RNA positive and/or HIV-InnoLIA positive, regardless of other HIV results: refer to Infectious Disease clinic
HIV-InnoLIA and/or HIV antibodies indeterminate: permanent deferral, HIV infection not confirmed
HIV Ab negative and HIV-RNA negative and HIV-InnoLIA negative: reenter into donor pool
This algorithm is represented in Medinfo as follows:
HMC Doha 2011-2020: Set-up of both donor and patient modules including inter-depot transfer:
Donor:
Implemented COVID-19 convalescent plasma CCP production at HMC Doha over two-week period, February-March, 2020 including full integration with software
Donor collection, donor marker testing, donor immunohematology testing, inter-depot transfer between production site and hospitals and hospital-hospital transfers, ISBT labelling and specimen
Collection Interface (read-only) with Qatar Ministry of Interior to obtain both English and Arabic demographic information from donors
Establishing world’s first interfaces (bidirectional as required) with Terumo BCT Atreus and Reveos automated blood processing equipment, Mirasol pathogen-inactivation/platelet additive solution, Terumo Trima Accel donor apheresis machine, Terumo mixer-shaker donor collection device
Patient:
Implemented a CCP quarantine patient blood bank separate from regular hospital blood banks) for thawing and releasing of CCP plasma
Patient module including all compatibility testing, ABO/D typing, extended antigen typings, direct and indirect antiglobulin testing (antibody screens), antibody identifications, eluate, component modifications (thawing, pooling, aliquoting), interfacing of Diamed automated gel testing
Establishing algorithms for emergency release, electronic crossmatching, automated patient specimen titration with Ortho Vision MAX, prophylactic antigen matching, ensuring irradiation of blood components or use of pathogen-inactivation as required, allocation rules by algorithm, required and optional antigen matching in presence of antibodies
Development of bidirectional interface between Medinfo patient module and Cerner Millennium laboratory module (permitting order of transfusion tests and blood component orders in Cerner, transmission to Medinfo patient module for testing and allocation of components, and then sending test results and component status back to Cerner)
Common:
Developing current and future states to develop the workflows to prepare software processes
NGHA Riyadh 2009-2010: Set up of both donor and patient modules including inter-depot transfer:
Donor:
Collection, marker testing, immunohematology testing, component production, inter-depot transfer between production site and hospitals and hospital-hospital transfers, ISBT labelling and specimens
Patient:
Patient module including all compatibility testing, ABO/D typing, extended antigen typings, direct and indirect antiglobulin testing (antibody screens), antibody identifications, eluate, component modifications (thawing, pooling, aliquoting), interfacing of Diamed automated gel testing
Please refer to my website https://drzeydbloodbank.com for specific posts on Medinfo software process building. On the right hand side from the bottom TAGS menu, pick Medinfo Hematos IIG to see those articles.
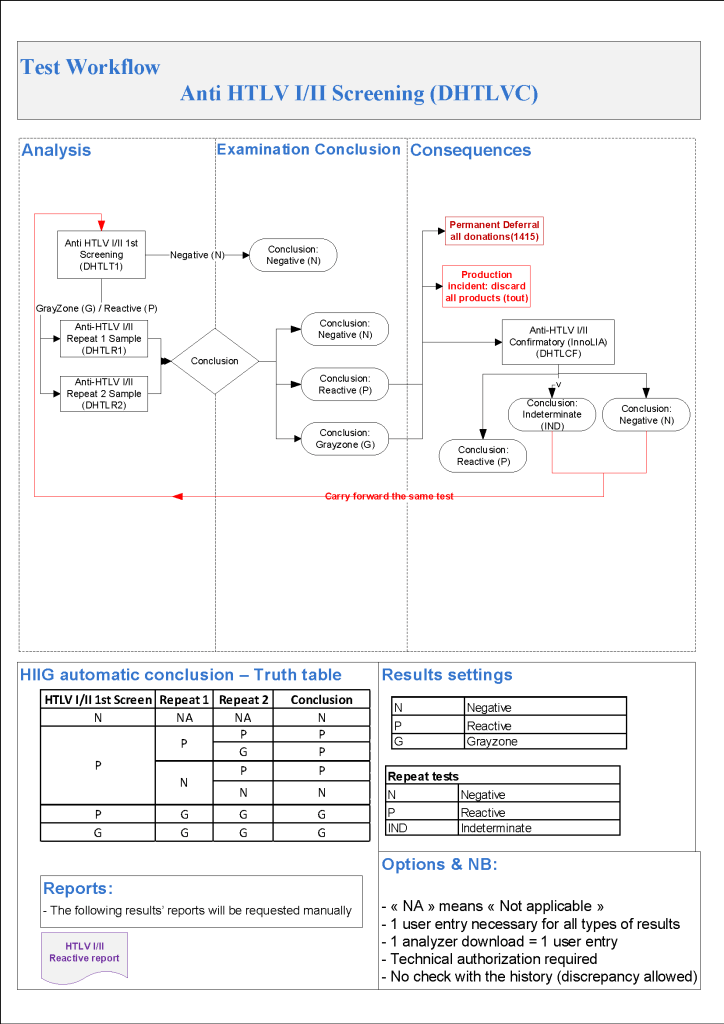
As I designed in Medinfo, this is a much simpler algorithm than HCV and uses an HTLV-1/HTLV-2 screening test and a confirmatory linear immunoblot assay LIA that can discriminate between type 1 and type 2. If there is an indeterminate result, a repeat test is ordered after 6 months:
HTLV 1/2 Testing:
HTLV Antibodies positive, then do HTLV-InnoLIA:
HTLV InnoLIA positive for HTLV-1 and/or HTLV-2: refer to Infectious Disease clinic
HTLV InnoLIA indeterminate or negative, repeat HTLV Ab and HTLV InnoLIA testing after 6 months
Repeat HTLV Testing After 6 Months:
HTLV 1/2 antibodies positive, permanent deferral and do HTLV InnoLIA
HTLV 1/2 antibodies indeterminate, permanent deferral and do HTLV InnoLIA
HTLV InnoLIA positive for HTLV-1 or HTLV-2: refer to Infectious Disease clinic