Processes and Software Building—Part 17
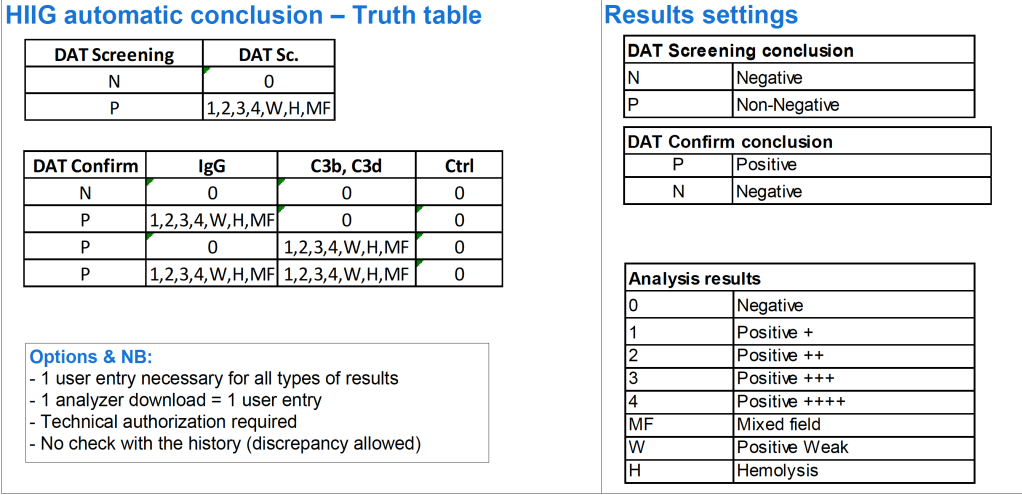
The direct antiglobulin test DAT may be the first or last place that a delayed hemolytic transfusion reaction can be detected. In my practice, I always performed it the first time I encountered a patient with a positive DAT. If the subsequent DAT testing is of the same strength and there is no change in the clinical status of the patient, then I might empirically repeat the elution after 14 days, i.e. just when new antibody emergence may be detected.
In summary, my criteria for elution after a positive DAT are:
- First patient encounter with a positive DAT
- At least 14 days since the previous elution
- DAT strength has increased since the previous exam (at least 1+ increase in strength in either IgG or C3)
- Patient shows evidence of hemolysis
- Suspected cases of drug-related hemolysis
- Transfusion Medicine physician specifically orders it otherwise
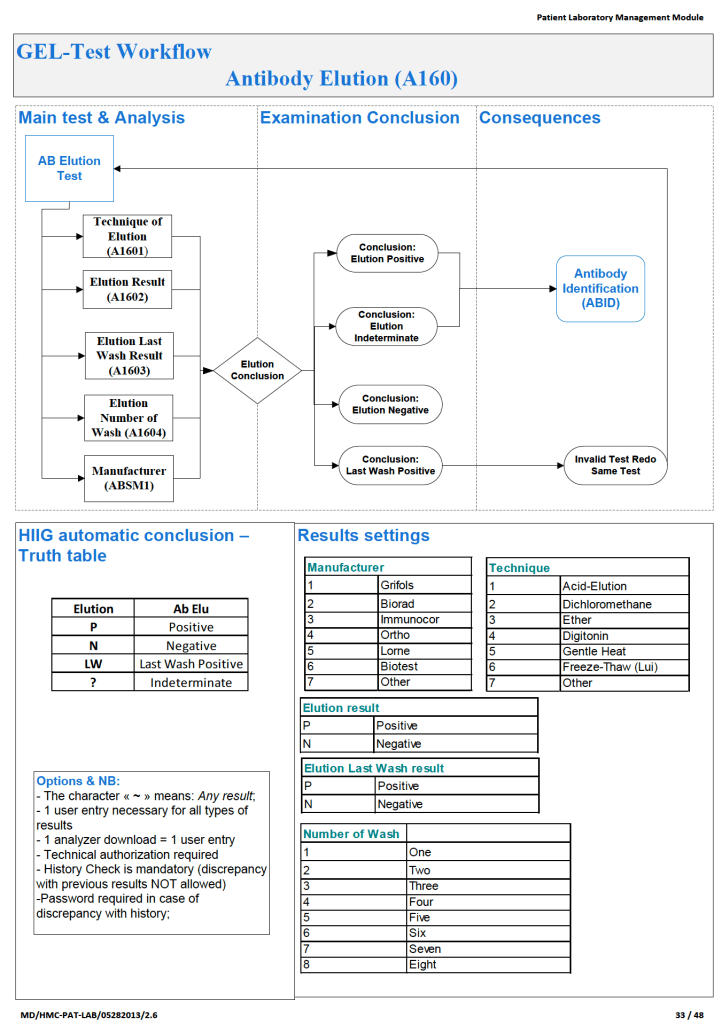
In the software processes, the following parameters were recorded:
- Technique of elution (acid glycine, dichloromethane, digitonin, ether, etc.)
- Number of washes (too many may remove the antibody from the RBCs)
- Last wash result (must be negative to accept conclusion)
- Manufacturer of the elution kit (if any)
- Elution result based on panel testing
Note:
- All indeterminate or positive eluates would trigger an antibody identification.
- All results would be reviewed by me or the covering Transfusion Medicine physician. A comment would be entered into the results that could be viewed by the clinician either directly from Medinfo or through the hospital information system.
If the DAT was only positive for complement, it was up to the Transfusion Medicine Consultant to decide whether to proceed with elution. Personally, I would usually proceed because the eluate is more concentrated and may occasionally detect an antibody that was not noted in the patient’s plasma.
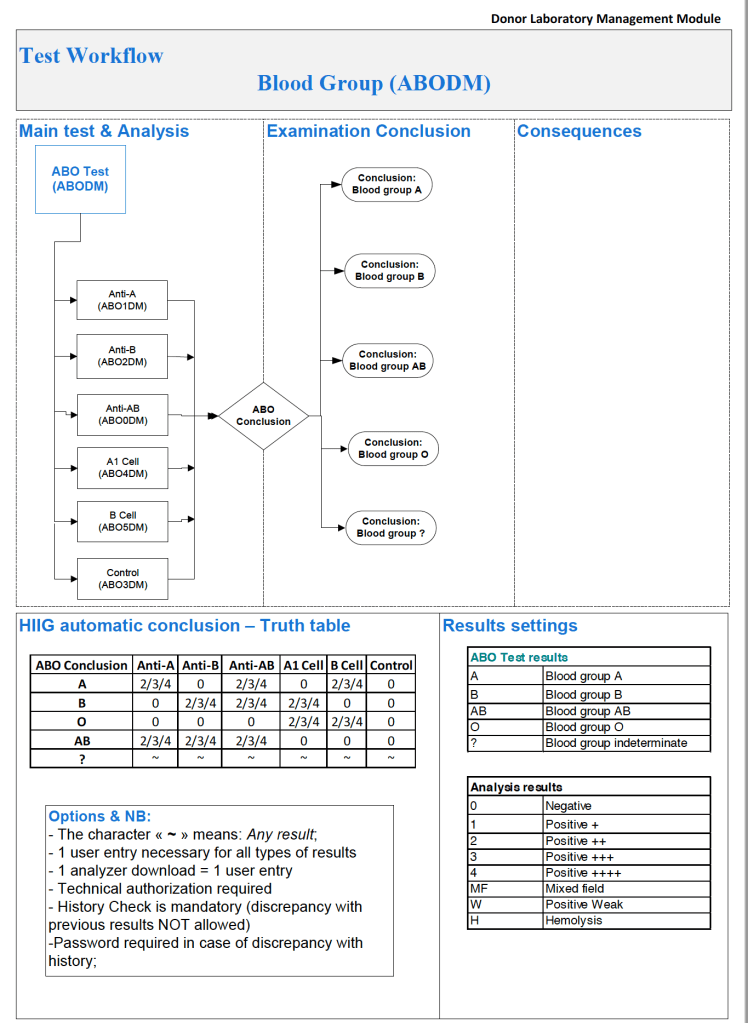
The attached Medinfo workflow shows the process designed by me for use at HMC Doha.