Donor, patient, interdepot transfer, interfaces
Principle:
As part of good manufacturing process, we must trace everything in Transfusion Medicine, from registration through release of components. The adoption of the Medinfo Hematos IIG computer system allows us to document anyone and everyone who “touches” the blood components and all processes.
Policy:
References:
I designed my blood bank software Medinfo for use by my staff at all levels and positions to adhere to and facilitate compliance to the workflow processes. Blood bank staff were restricted to access only those functions needed for their job duties.
Blood Donation records could not be viewed by outside staff for confidentiality reasons. Blood donor records were not linked to patient records at all.
We did not allow access for Medinfo to non-Transfusion Medicine staff since the screens were designed to maximize efficiency of the work processes, not the viewing by outsiders of results. Outsider access was made through the hospital information system HIS.
The separate hospital information system HIS interfaced to Medinfo for the following functions:
Even within the HIS ordering capabilities, there were additional restrictions:
Results viewing in the HIS were subject to additional conditions as well:
Only certain results, not all results were viewable directed in the patient’s chart since showing all results may be confusing to the outside physicians and nurses. The selected results were sent back into the HIS for viewing. All these non-viewable results were retrievable for blood bank staff in Medinfo.
Another option, one I did not use at either HMC Doha or NGHA in Saudi Arabia, was to order tests and components by physicians directly into Medinfo. Likewise, they could view test results directly in the system. Special screens could be constructed to offer ordering and results retrieval.
This is a sample document for use of expired reagents I wrote for HMC Qatar.
Principle:
Due to logistics issues including the long distance between suppliers in Europe and North America and Qatar and the importation/customs clearance of critical materials, Transfusion Medicine has developed a contingency variance policy to minimize disruption of the essential transfusion medicine testing and component preparation. Approval for use of outdated reagents in special circumstances is not meant to be an excuse for untimely monitoring and improper ordering of supplies.
Definition:
Rare Reagent: Any reagent that is either used uncommonly or is in short supply and difficult to obtain in a timely matter.
Policy:
References:
Sections 1.3.2 and 7.0, Standards for Blood Banks and Transfusion Services, Current Edition, AABB, Bethesda, MD, USA
When I started my COVID-19 convalescent plasma CCP collection in early March, 2020, there were few antibody tests available. However, I anticipated that eventually we would want to include antibody results with the donor record. Antibody results were not used originally at all in the criteria for CCP acceptability for release.
There are many assays by type of antibody (total, IgG, IgA, IgM) and quantitation by titer and/or signal-cutoff ration S/CO. Any of these parameters may be used to define rules for acceptability to complete production and/or allocate to patients. Instrumentation used for titering/quantitation may be interfaced to the blood bank software.
Here is my generic approach to including these results with the donation record. In Medinfo HIIG, it is possible enter test results retrospectively and these can be used set rules for acceptability. Please consult with my detailed post on using rules against parameters.
All of this is easily implemented since all test information will be stored as parameters. From these parameters we can construct rules for:
Also, one can override the rules if the clinician and the transfusion medicine physician agree. For example, there is a severe shortage of group B CCP so use of low-COVID-antibody titer group B CCP could be allowed.
The key is to build whatever test methodology you use and include the manufacturer’s cutoff for low versus high titer interpretation. These results can be printed on the ISBT label as well. One can easily build multiple methodologies and acceptability criteria if different tests are used at different testing sites in your system—just as can be done for other tests (ABO/D, antibody screen, etc.) If one changes methodologies in the future, Medinfo will still use the same rules that applied for the day of production.
Here are some sample test rules:
Example 1: Total COVID antibody > 160 is high titer:
Example 2: IgG antibody with S/CO ratio > 12 is high-titer:
Example 3: IgG and IgM antibodies must have S/CO > 12:
Another option would be just to record the quantitation for each antibody type and list this on the ISBT label and permit its release regardless of the value. One could also permit low-anti-B titer group A plasma with whatever rules you set up.
Medinfo Hematos IIG has an underlying framework of functionality. It is flexible since it acts upon rules based on parameters (e.g. sex, age, diagnosis, test results, etc.) You can change the processes in the system by changing the parameters without upsetting the underlying structure of the software. This means you can make changes very simply and quickly without having to “hard-code.”
Rules are based on parameters which are entered into the system by the user or the results of previous action. I am listing here some examples of parameters used to define processes in my Medinfo installations:
Based on these parameters, the system may require:
Examples:
Overriding rules:
One can also define if the rules can be overridden by someone with appropriate credentials:
On the other hand, rules can be specified to prohibit overriding:
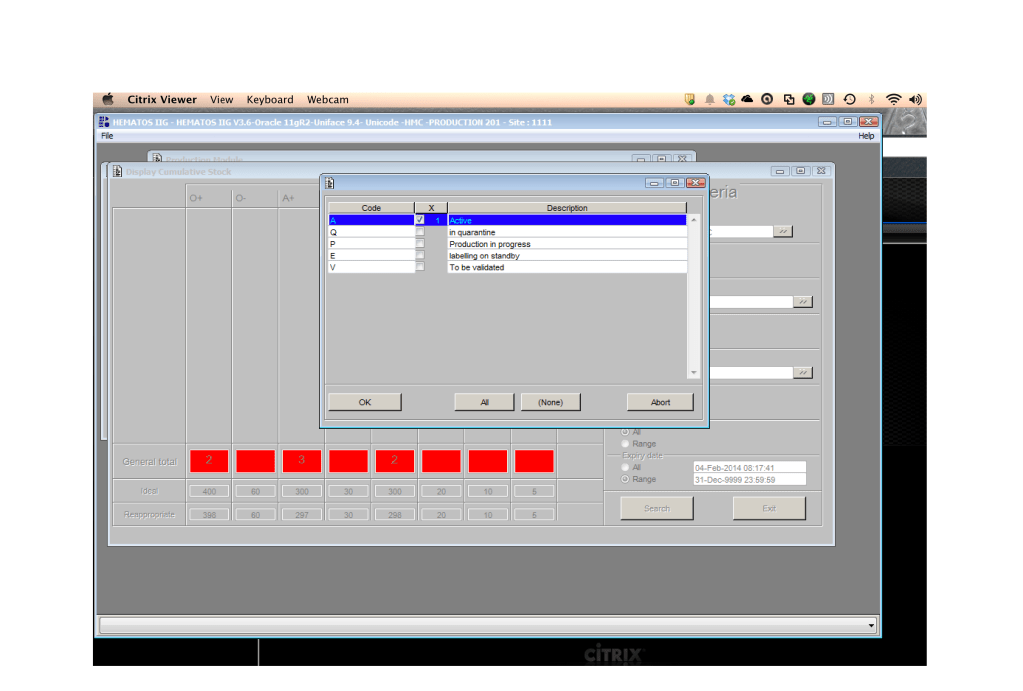
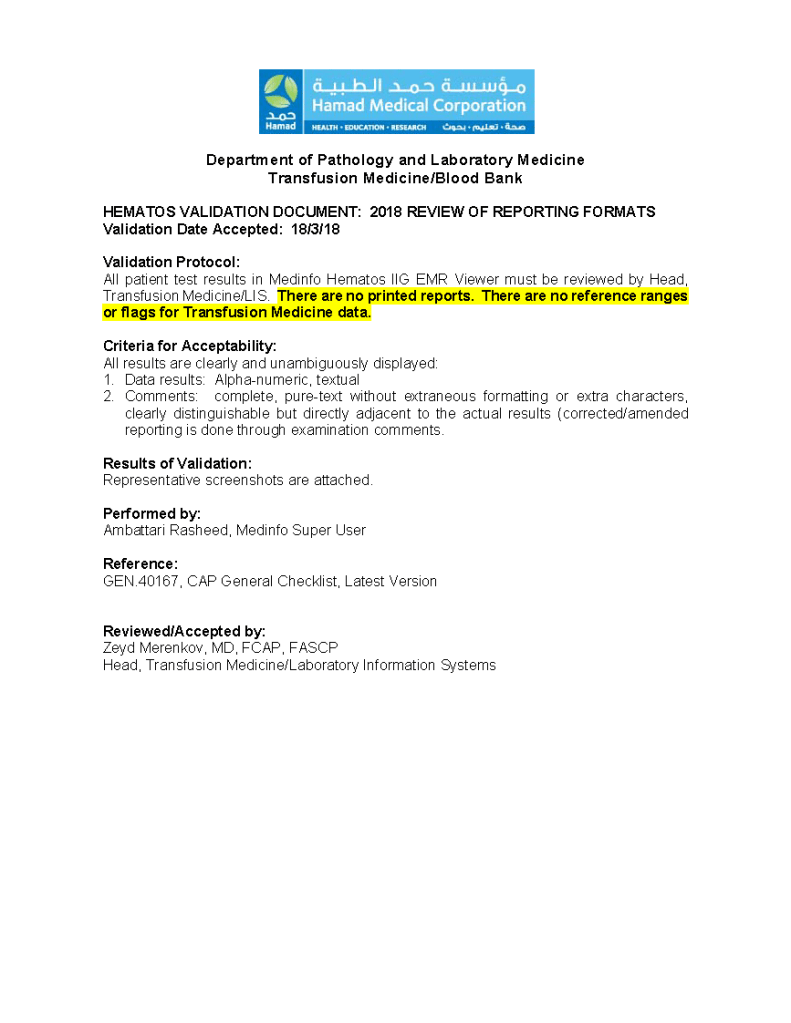
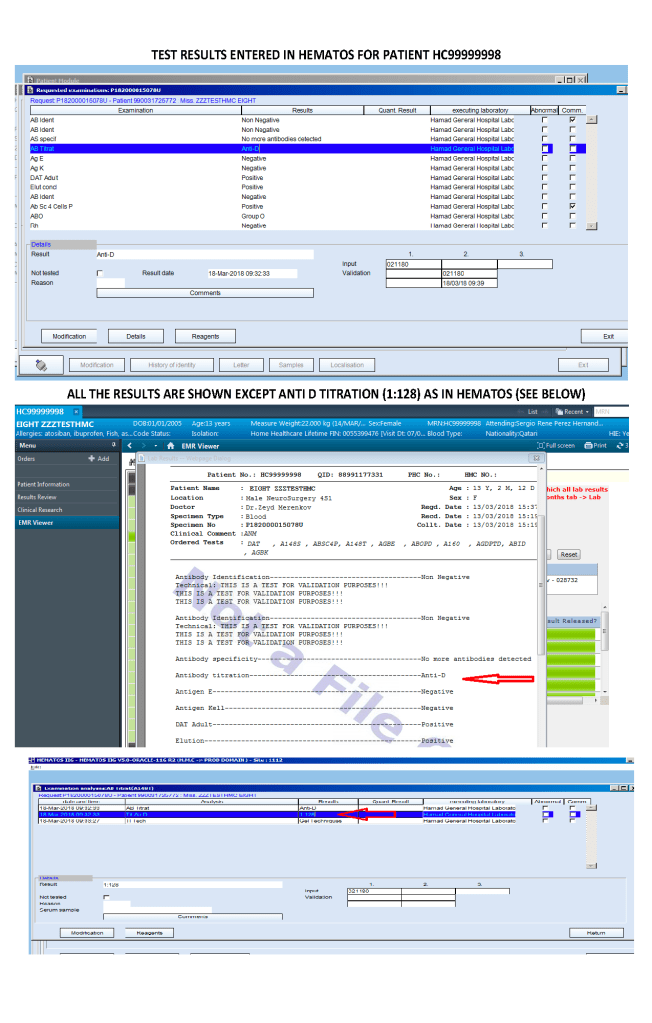
The attached PDF illustrates a sample validation of reporting formats for transfusion service testing. The validation criteria are explicitly stated. The evidence, in forms of screen shots, is attached to the PDF. The data is reviewed and then accepted by me as the Division Head, Laboratory Information Systems.
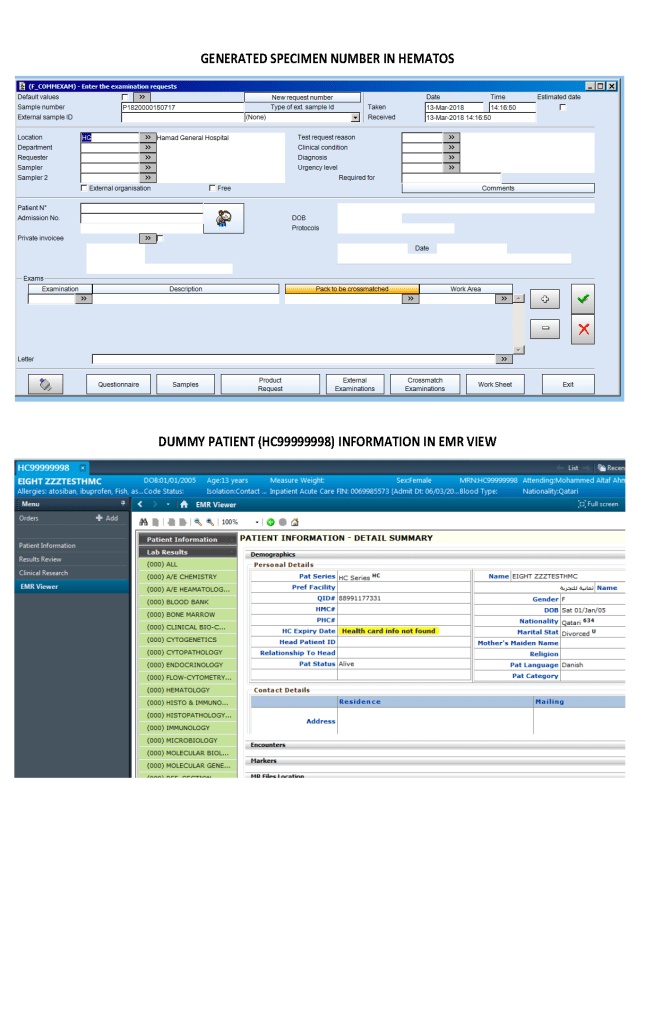
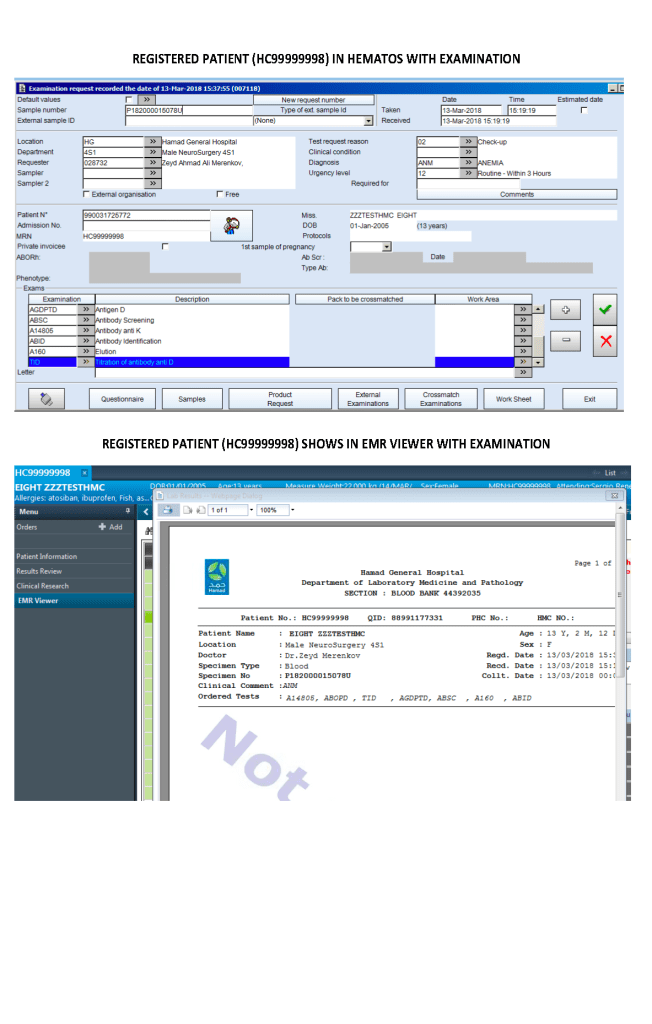
Please note in this sample, no actual patient data was used. All testing was done in a non-production environment.
Here are the embedded screenshots:
In my career, I have worked with many different hospital and laboratory computer systems. One of my greatest frustrations has been providing software permissions to staff at all levels, from clerical, nursing, technical, and medical—inside and outside the blood bank.
The software permissions that I am specifically referring to are those with the blood bank software. These I directly controlled as Division Head of Transfusion Medicine and Laboratory Information Systems. I am not talking about virtual private networks or Citrix or cloud-based software controlled by the hospital IT department.
Here are some examples of inappropriate permissions:
The golden rule is to only give access that is needed for each staff’s job designation. Staff must sign an agreement not to access the system except for work and not release anything to non-designated personnel.
I recommend separating privileges by:
Permissions within a test category may include test ordering, result entry, verification/authorization, and/or purging. In the donor center, it may include registration, donor qualification, collection, donor marker testing, donor immunohematology, component processing, component modification, and/or inter-depot transfer of components. Management tools included in the software may also be restricted to high-level staff.
In this time of COVID and staffing shortages, we may be training new staff to work in the blood bank. During their training, these trainees can be competency assessed and be given access to limited functions. In Medinfo Hematos IIG, you can give staff custom permissions test-by-test so for example, if they are deemed competent for ABO/D typing, you could restrict their access to only those tests as an interim measure.
Having customized access for each employee can be nightmare for the systems administrators so this granular special access must be kept to a minimum. However, it is good to know that you do have this capability if needed.
Principle:
In accordance with AABB Standards, all actions contrary to the standard operating procedures and policies of Transfusion Medicine must be specifically approved by the Head, Transfusion Medicine or designate.
Documentation of variances must be organized in a system for ready retrieval for analysis. They should not be entered into a system that is cumbersome to find the entered variances.
Examples include but are not limited to: Rh(D)-incompatible transfusions, least-incompatible crossmatch, extension of expired rare reagents, etc.
If the same variance is occurring frequently, it should be determined if modifications in the underlying documentation (policies, processes, procedures) should be made.
Policy:
References:
This is the early Qatar experience of treating severe COVID-19 using locally produced Covid convalescent plasma CCP. At that time, the plasma was not tested for SARS-CoV-2 antibody levels.
https://drzeydbloodbank.com/wp-content/uploads/2021/01/jmv.26537.pdf
