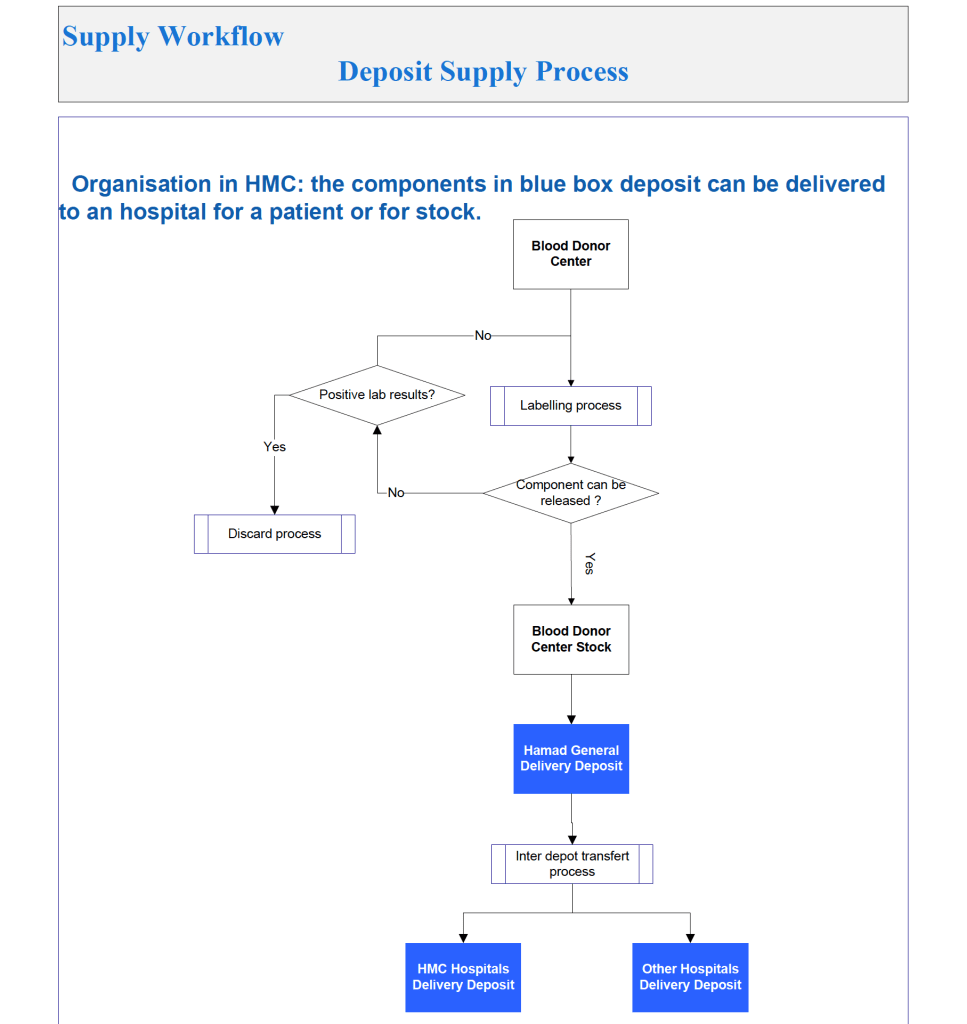
This is the start of a series of posts on how Medinfo blood bank software was designed for product delivery in the HMC system in Doha.
The overall process was:
Transfer blood components (all types) from the Blood Donor using the Interdepot Transfer process (see that post for details) to the Hamad General Hospital HGH General Delivery Deposit.
Release components to individual HMC system hospitals and client blood banks from the HGH General Delivery Deposit,.
It was also possible to release blood components directly from the Blood Donor Center to HMC hospital blood banks as a contingency. Client hospitals outside the HMC system still had to obtain their components from HGH General Delivery Deposit.
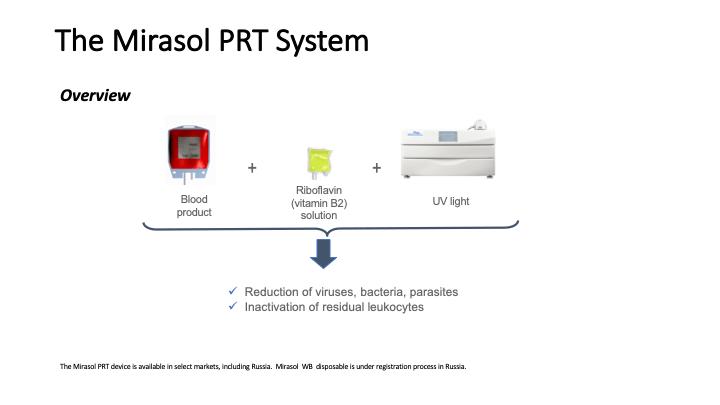
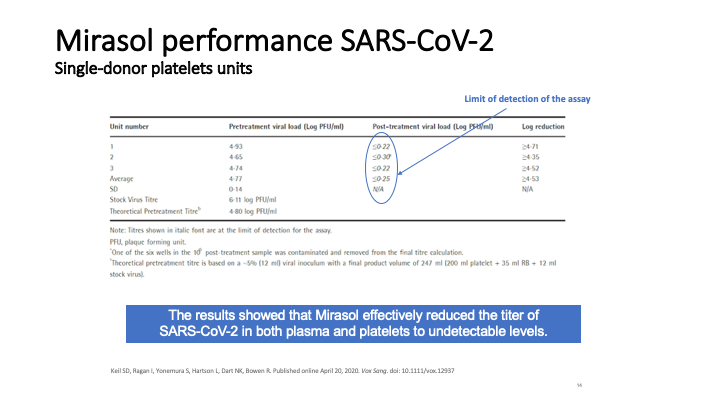
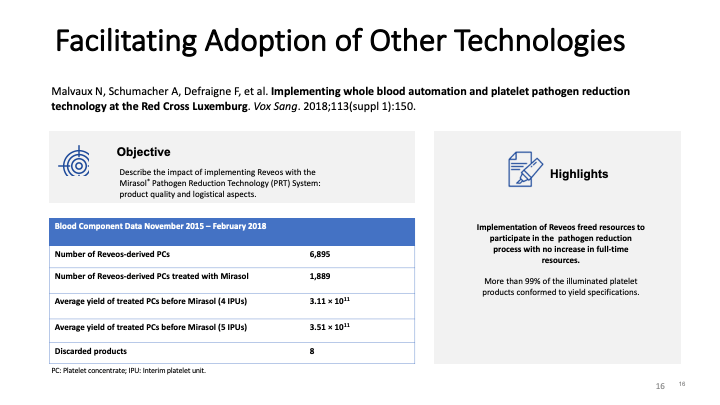
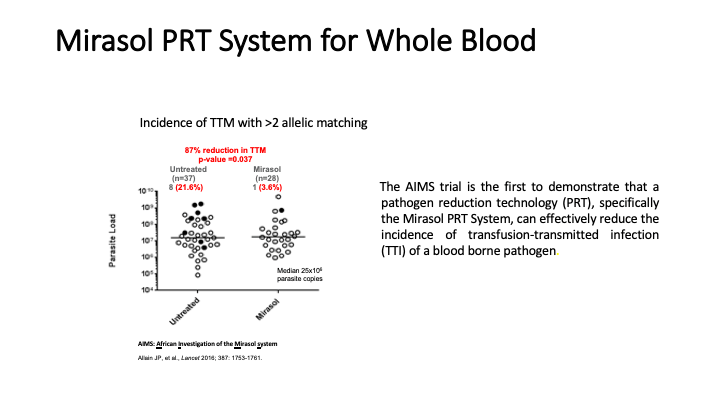
This is the virtual talk I gave at the Russian Transfusion Congress in Moscow on 13 May. It gives a brief description of automated component processing and riboflavin-based pathogen inactivation and then discusses the use of these technologies together to free up labor and enhance the quality of products, i.e. improved GMP, especially if a dedicated blood bank computer system is used to enforce production rules.
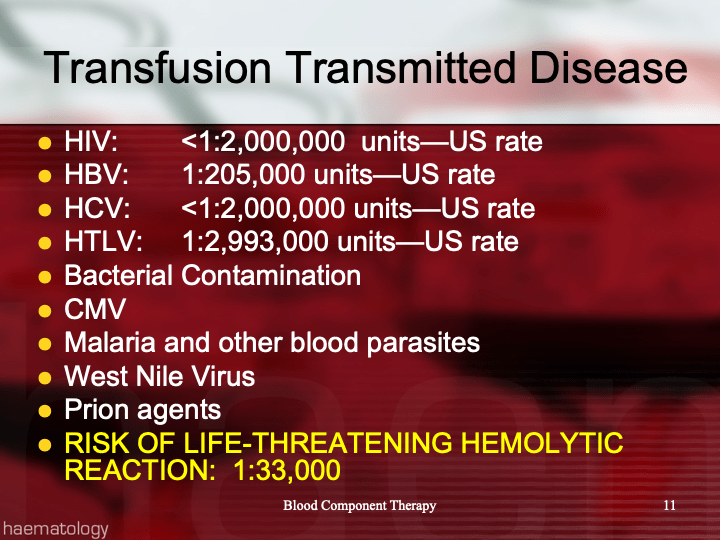
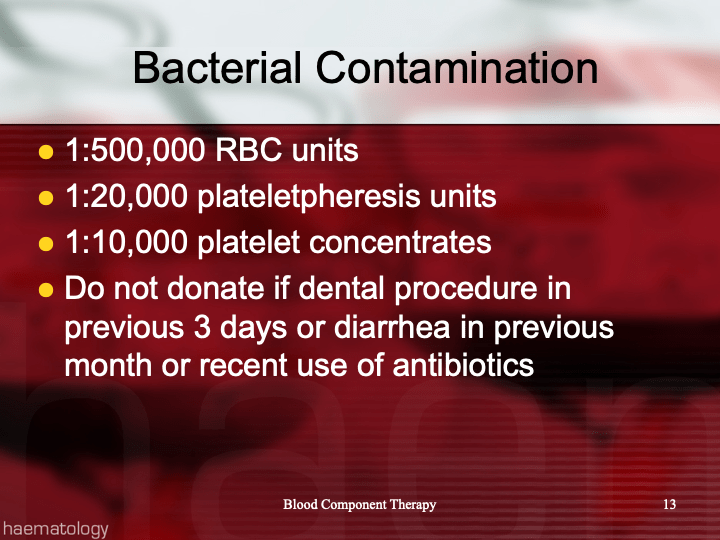
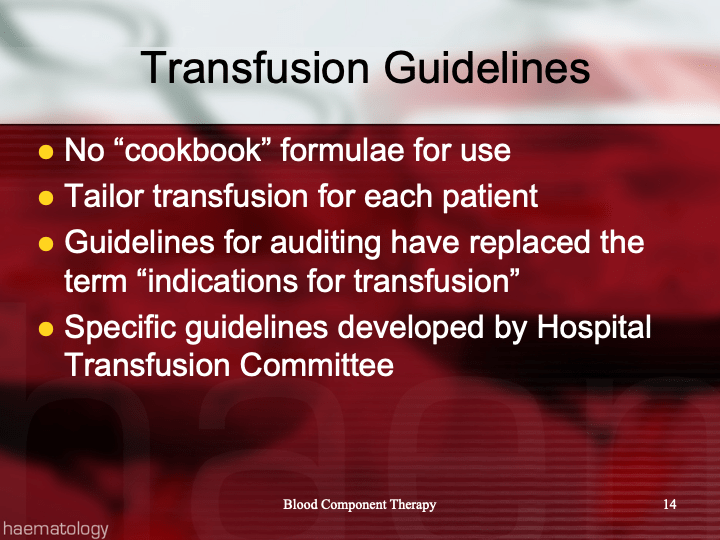
This is the final section of this base medical student lecture originally given at NGHA Riyadh. It has been updated to current technologies and current types of blood components.
This presentation was originally given to third-year medical students at NGHA-Riyadh as their first lecture, Introduction to Transfusion Medicine. It has been updated for new component types and will be presented in multiple parts.
All donor unit mislabeling is potentially life-threatening and must be stringently investigated as soon as possible after the discrepancy is detected. Most importantly, if there is one error, there may be possibly ADDITIONAL donor unit errors (e.g. switch of donor tubes or units, etc.). All donor units processed in the same batch must be also quarantined until the discrepancies are resolved.
Definitions:
Responsible blood bank physician: specialist or consultant physician on-call at the time the discrepancy is detected
Policy Details:
The following steps MUST be performed as soon as possible:
The Component Processing Supervisor or Senior Technologist must be IMMEDIATELY notified of any discrepancy.
The Blood Bank Supervisor will inform the Division Head, Transfusion Medicine. If the Head is not available, notify the Transfusion Medicine on-call.
Quarantine ALL donor units collected and processed in the same batch.
Obtain copies of all testing including photos of the gel/glass bead cards documenting the discrepancy.
Obtain copies of all worksheets used in donor processing for the affected batch.
Perform repeat ABO/D typing of ALL DONOR UNITS in the affected batch. Any further discrepancies must be investigated and resolved.
Identify all staff who were involved in handling the donor unit (phlebotomist, blood bank technicians processing and labelling the unit). Identify those associated directly with the error.
Submit all documents and photos to the Blood Bank Supervisor or designate.
Prepare an occurrence/variation OVA report documenting all the data, findings, and interpretations.
All investigations must be reviewed by the Supervisor, responsible blood bank physician, and one of the senior consultants.
All such investigations must then be finally reviewed and approved by Head, Transfusion Medicine or his designate. Only when the issue(s) are completely resolved and investigation is approved may the donor unit be properly relabeled and released into available stock. Also, only at that time may the other units in the affected batch be released into available stock!!
Photograph the correctly relabeled unit and attach it to the other documentation of the incident.
If the discrepancy cannot be resolved, ALL units in the affected batch must be discarded.
The implicated staff’s personnel record should be reviewed for previous errors. Appropriate disciplinary action should be taken and documented in the personnel record. If a verbal warning is given, it should still be documented in the written record.
If there is a systemic cause for the error, appropriate measures should be taken to minimize reoccurrence.
All actions must be in accordance with the applicable regulations.
The Medinfo HIIG interface to the Reveos is a bidirectional interface, which was first developed by the Medinfo team for HMC in Qatar. It is similar to the Atreus interface but there are 4 units processed simultaneously in each cycle of operation whereas the Atreus only processed 1 unit each cycle. In Qatar it was used in conjunction with Mirasol riboflavin-based pathogen inactivation.
The process is:
Medinfo controls registration, donor screening, and donor collection of whole blood and apheresis-derived (Trima) components.
Medinfo will assign ISBT specimen labels for the whole blood collected with the Reveos blood kit.
Medinfo will not allow processing of whole blood units not meeting donor criteria (donor screening, volumes, collection time, donor deferral database, etc.)
Reveos will read ISBT specimen labels generated by Medinfo.
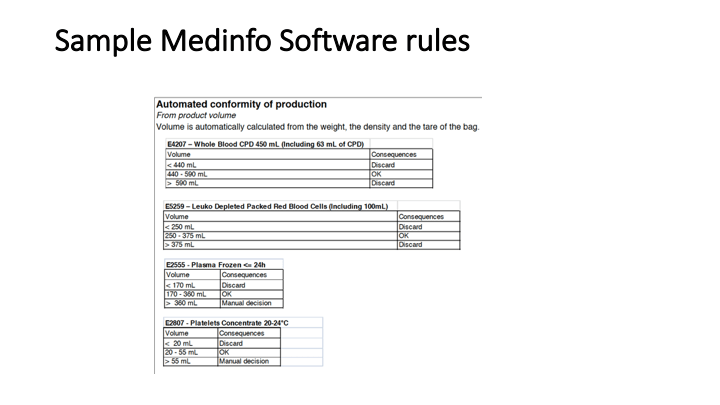
Upon processing, Medinfo will receive from the Reveos machine the packed red blood cell, plasma, platelet, and buffy coat volumes for each bucket in the Reveos machine.
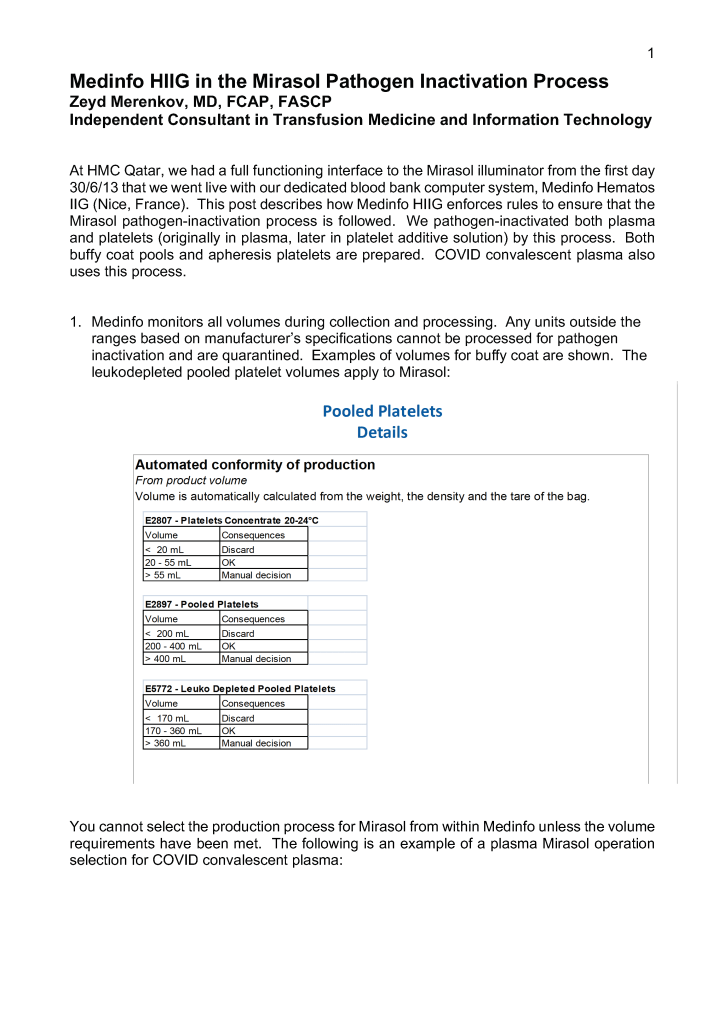
If the volumes are within the specified ranges, platelet pooling and Mirasol pathogen inactivation of platelets and plasma may proceed.
For each component, the following information will be collected:
All timestamps in the process
Which Reveos machine used
Which bucket in each machine used
Volumes collected (packed RBCs, buffy coat platelet, plasma volume)
Reveos collection set details
Processing technologist ID
The key point is the complete TRACEABILITY of each component throughout its production. Should there be a failure in production, we can trace exactly where the problem is and then quarantine this and any other affected units simply in the system. Additionally, this information is part of the permanent record of the unit so it can retrieved subsequently at any time.
This post is about my over 10 years of experience with automated component processing using Terumo equipment, first Atreus and then Reveos at HMC Qatar. The Reveos system is still in use at that institution. There is also a previous post about Mirasol riboflavin-based pathogen inactivation.
We were the first place in the world to combine the automated component production Atreus with the Mirasol pathogen inactivation. Their synergism was very important in the rapid throughput of component production for Qatar.
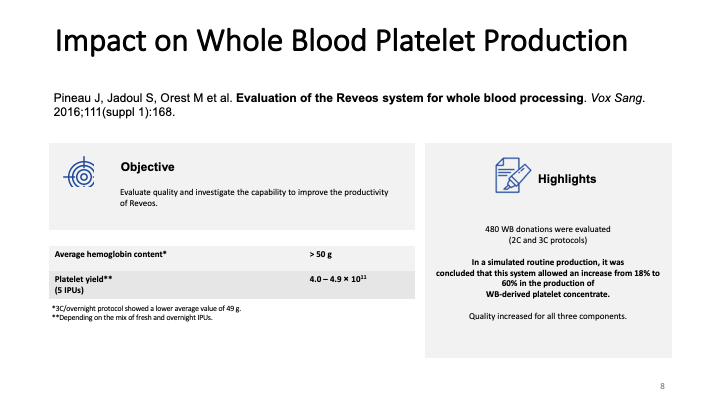
Terumo has two programs, 2C (C for components) to yield plasma and RBCs and 3C for yielding RBCs, plasma, and platelets. The 2C program is faster but no platelets are separated.
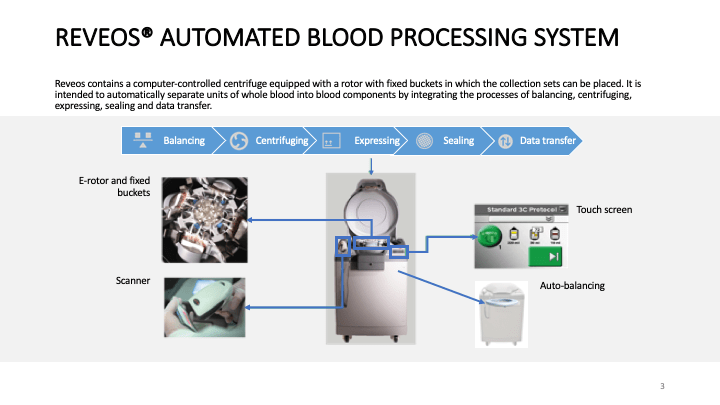
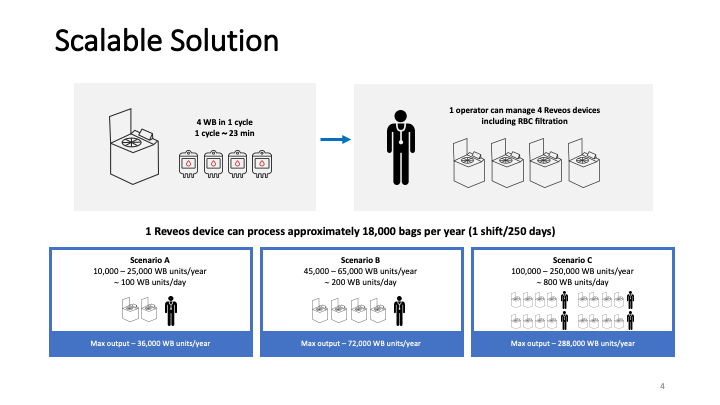
We used the Atreus since 2010 and later replaced it with the Reveos in 2016. Both systems use a special blood bag set that collects the whole blood in European CPD. The kit is carefully placed in the machine. Atreus machines accepted one blood bag set, the Reveos can accept up to 4 sets. In both cases, the whole blood is processed to yield packed RBCs, leukoreduced plasma (<1E6 residual WBCs), platelets, and a special WBC bag (i.e. the residual buffy coat, which is not for clinical use.
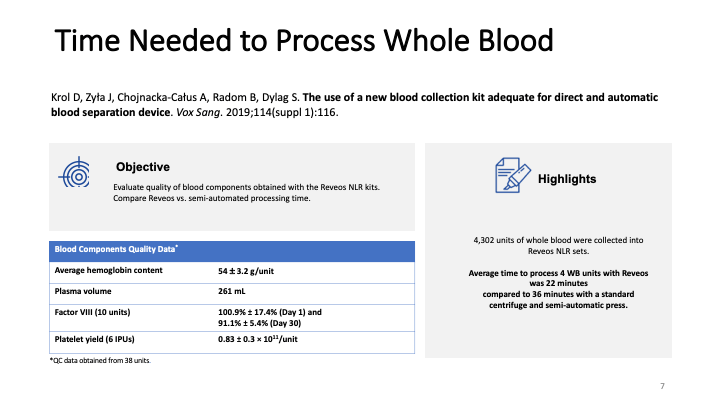
The Atreus took about 10 minutes to process the one bag set whereas the Reveos processes 4 bag sets in slightly more than 20 minutes. Thus, the throughput from the Reveos is twice that of Atreus.
We had 4 Atreus and later 4 Reveos machines and these were handled by up to 4 technologists, depending on the number of the units. While the machines were running, the staff were filtering the RBCs and platelet pools, pooling the platelets, and performing the PAS-Mirasol pathogen inactivation. The workflow was not hectic and staff were not stressed out by the multiple tasks. Normally 1 staff member ran the Reveos or Atreus machines at any one time.
When the processing was complete, the RBC bags were filtered with an integral leukodepletion filter designed to leave a residual of <1E6 WBCs in accordance with the CE Standard. The platelets were combined to give a target yield of >= 2.4E11 absolute number of platelets. Then the pool was leukodepleted by filtration to a residual of <1E6 WBCs.
Both Reveos and Atreus measured the RBC, platelet, and plasma volume yields. Additionally, for platelets a Platelet Yield Index PYI was calculated as a relative measure of the platelet yield. To reach a goal of 2.4E11 platelets, the PYI indices for the individual platelet bags were added so that the total exceeded 240.
When combined with the Mirasol system, the component volumes for the plasma and platelets needed to be within specified ranges. Both systems could easily meet these requirements.
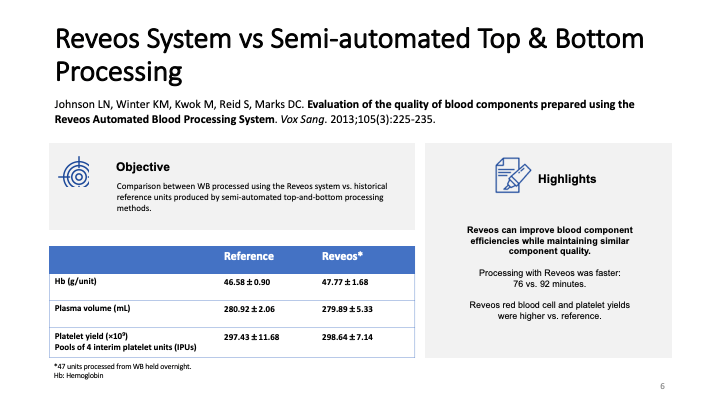
When we switched from Atreus to Reveos, our platelet yields increased. The transition period was only two weeks. When we adopted platelet additive solution PAS at the same time, the Reveos had a special program to make “dry” platelets with less volume so that the PAS could be added and still stay within the acceptable range for pathogen-inactivation.
Throughout these years, Terumo sent us special engineers to handle the Atreus then Reveos, Mirasol, and PAS processing. All staff were trained by Terumo initially before we finalized their competency assessments.
We had excellent local service: we never had downtimes due to equipment failures. During the COVID pandemic, all materials (kits, filters, Mirasol solution, and PAS) have been provided without interruption.
We went live with Medinfo Hematos IIG software for the entire blood donor center and hospital blood banks in 2013. From the first day 30/6/13 we had bidirectional interfaces first to the Atreus and later to the Reveos—the world’s first. Likewise, the Mirasol and PAS processing were fully integrated with Medinfo when they were activated.
The residual buffy coat was not used for patient care. However, it has proven invaluable as a quality control material for the stem cell laboratory. In addition, many researchers have used it to establish cell lines for investigational use.
Proper handling the collected whole blood units is critical to success:
Maintain the temperature below 25C.
Carefully stack the whole blood units in the blood containers—do not play “ring toss” and just throw them into the container.
In summary, I am very pleased with using this system for over 10 years. In a few weeks, the production laboratory was fully GMP compliant using a diverse group of staff with varying technical backgrounds.
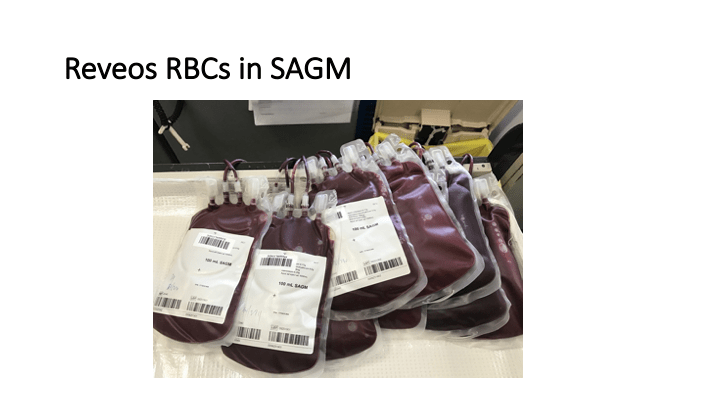
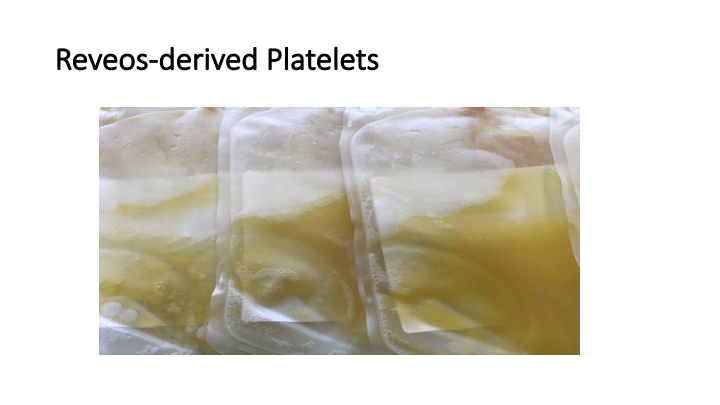
The following are some pictures of the Reveos and its prepared blood components.
Reveos Machine has 4 chambers to process the 4 whole blood units.Reveos takes up little space: this crowded corner processed all whole blood for Qatar.Buffy-coat platelets processed by the ReveosClose-up of Reveos buffy coat platelets: notice there are NO streaks of RBCs.
This is a teaching document of a process to irradiate RBC components when our irradiators are not functioning. In our system, we used Mirasol pathogen-inactivation so our RBC units were affected. The number of units for advance irradiation was based on our historical usage of irradiated units across our system. The workweek is Sunday-Thursday so on Thursday special effort was made to have the minimum number of irradiated units available.
We used irradiated units for compatibility testing to avoid the possibility that the unit would be released without irradiation.
Emergency Interim Procedure:
Verify the patient’s diagnosis/location: All Hematology-Oncology patients should receive irradiated blood. Refer to the list of diagnoses for which irradiation is indicated (attached).
Only PRBCs need to be irradiated. Mirasol-treated (pathogen-inactivated) platelets can be used directly without irradiation in accordance to Council of Europe CE regulations.
Attach radiation indicator labels to the selected units as per the irradiation procedure.
Send the units for irradiation to the Radiation Oncology department.
Verify that the proper dose of irradiation was received while in the Radiation-Oncology department.
Keep a minimum stock of 20 group O-positive units irradiated at the start of each day AND before the start of the weekend on Thursday afternoon. Irradiate that number of group O-positive units plus any other specific requests for blood.
You should use the irradiated units for crossmatching. DO NOT CROSSMATCH FIRST BEFORE IRRADIATING!! If the antibody screen is positive, refer the specimen to the Transfusion Service for further processing and selection of units.
Note: If a special antigen typing is needed, we may have to irradiate after selecting the antigen-matched unit if it is not found in the group of irradiated units.
If a unit is required for a child < 20 kg, it must be washed before release if the unit was irradiated more than 24 hours previously according to our irradiation policy.