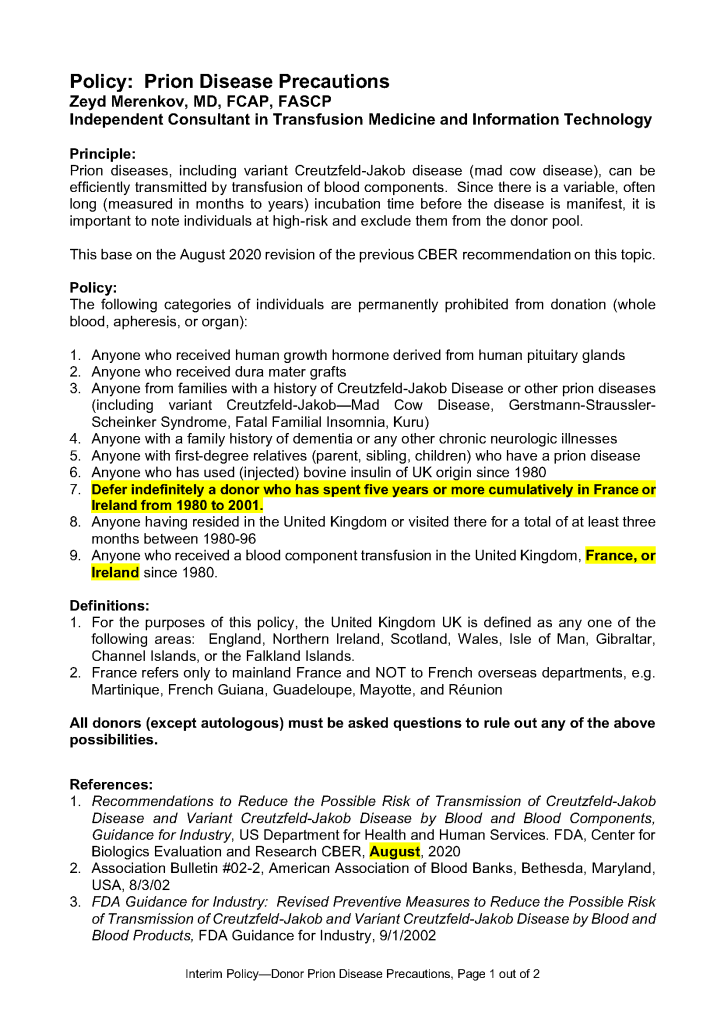
Policy: Prion Disease Precautions 27th Sep 202119th Jul 2021 drzeyd This is a revision to a previous post. All these criteria are built into the Hematos Medinfo IIG dedicated blood bank computer system.