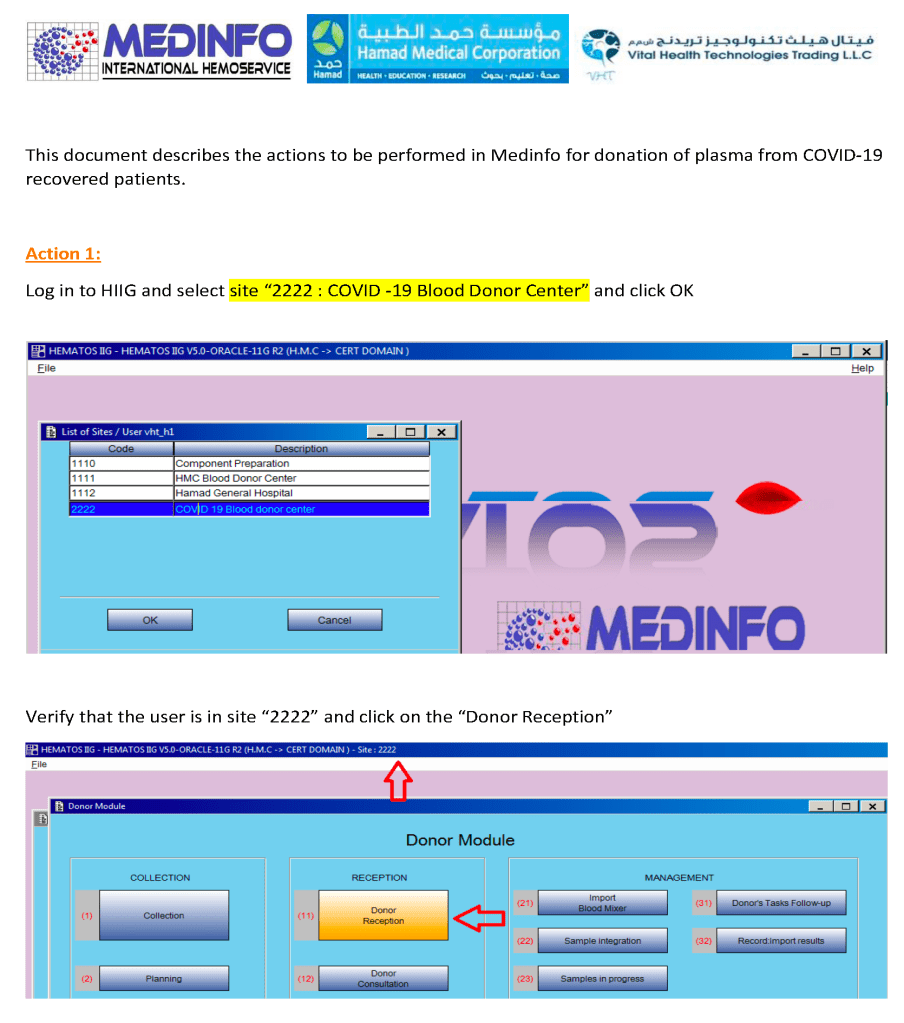
I designed a completely quarantined process for collection, processing, and release of CCP at HMC Doha. This document shows the Medinfo process for site registration as a separate donor center code.
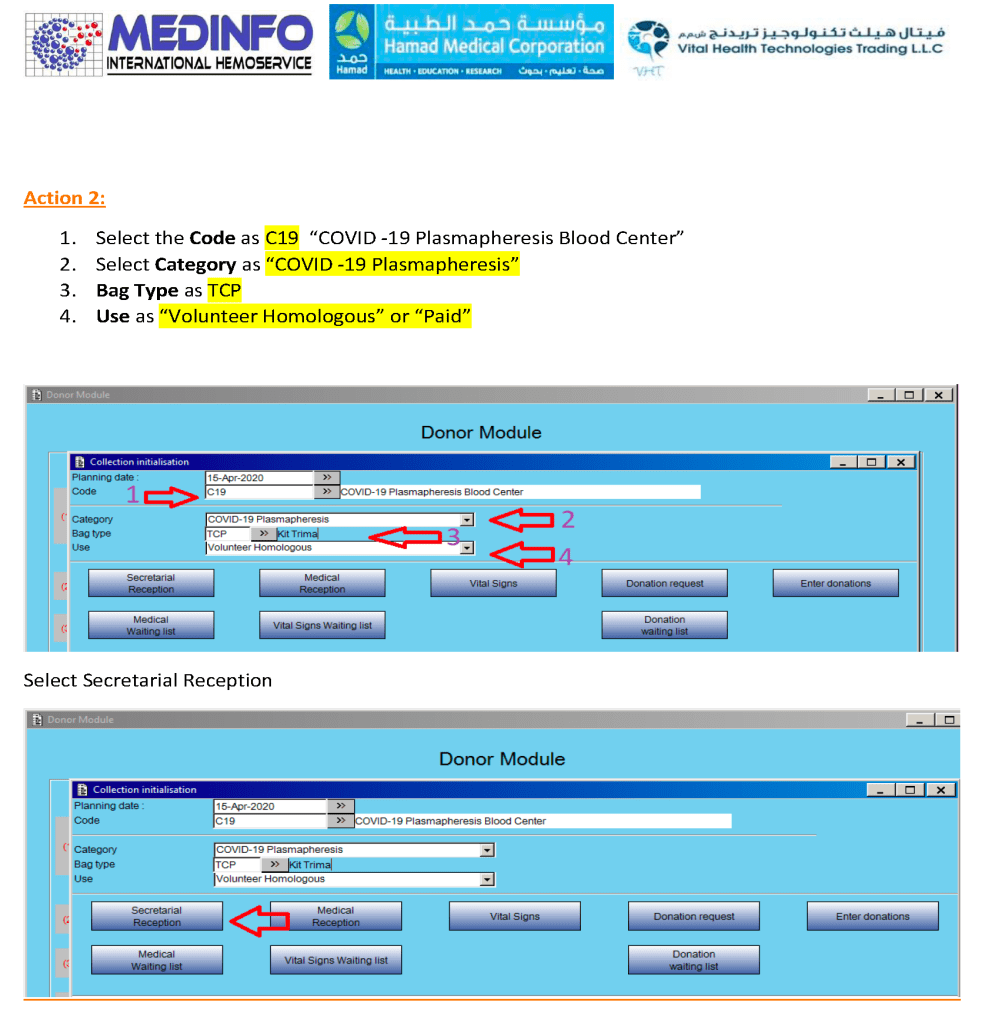
CCP could only be collected at this special site and only the apheresis bag could be used for collection. Regular donation options were not available at this CCP site nor was CCP collection an option at the regular donation sites.
It now has been over eight 8 months since I prepared the CCP workflow in Medinfo. It was built on the framework of the manual CCP process including donor prescreening with an abbreviated donor questionnaire. It was really quite simple and used the donor and patient modules to create quarantine areas for donor screening, collection, processing, and hospital patient blood bank release.
Here are my current comments on the process:
Donor Qualification:
I would still exclude malaria and HTLV from the donor questionnaire and would update to UDQ 2.1. Since these donors have recovered from a potentially life-threatening illness, I would keep the Hgb threshold at 11 g/dl.
Donor Collection:
In the future, I would consider using one of the soon-to-be-released portable devices that continuously monitor vital signs with pO2 and EKG lead to rule out asymptomatic pulmonary or cardiac problems.
I would also consider using low-ABO-titer, group A, universally to meet the demand for group B and AB patients.
Donor Testing:
There is still no need to segregate and separately test CCP donor specimens from regular blood donor specimens. I would perform SARS-CoV-2 antibody testing and set a threshold for qualifying donors—that threshold will be based on the manufacturer’s recommendations. However, if the treating physician wanted to use a low-titer unit, I would permit this.
Donor Processing:
There is no need to change this from the current processes. Keep the CCP processing separate from the regular operations.
CCP Plasma Release:
I would keep the quarantine release and restrict it to the locations used for treating COVID-19 patients
Medinfo Software Modifications:
I would record the IgG and IgM titers for SARS-CoV-2 antibodies in each donation record. This would include testing and entering the results on donations prior to this testing. ISBT labels should include this antibody titer.
Hospital Information Software Modifications:
Set up restricted CCP ordering for the actual treating physicians only. Also provide the ISBT code and shortened descriptors to it if necessary (certain HIS vendors still cannot read ISBT codes natively).
The original CCP workflow is attached for reference.
This process was originally done in the first phase of CCP collection. I have updated it to include SARS-CoV-2 antibody testing.
Principle:
Due to the pandemic, we will initially MANUALLY collect an experimental, investigational-use-only plasma product from apheresis donors and treat it with Mirasol. THIS IS A EMERGENCY INTERIM PROCESS UNTIL THE MEDINFO HEMATOS IIG PROCESSES ARE PREPARED AND VALIDATED.
Policy:
Good Manufacturing Practice applies:
Manufacturers’ recommended processes for equipment and materials usage applies.
All staff engaged in these processes must be competency assessed successfully.
Pre-Screening:
Clinical staff will use the prescreening document to select donors for pre-donation screening.
Quarantine:
All processes (day 0, day 1, day 2, and product modification and release) will be done in quarantine areas SEPARATE and DISTINCT from regular Transfusion Medicine activities. This includes:
Separate space and equipment must be provided.
Equipment for this project may NOT be used for regular, non-quarantine processes
Non-Transfusion Medicine staff will not be permitted in operational areas.
Prospective donors will not be permitted in the processing, testing, storage, or blood bank work areas.
Donation Process:
Day 0: Registration, check donor deferral database, questionnaire, physical exam including arm check, and specimen collection using ISBT specimen labels
Use latest manual donor questionnaire.
Day 1: Donor marker and immunohematology testing, review of results, accept or reject donor for actual plasmapheresis
Day 2: Collect manufacturer’s recommended volume of plasma (500 ml if < 80 kg, 600 ml if >= 80 kg), aliquot, pathogen-inactivate (Mirasol), freeze at minus 80C
Testing:
Testing will be performed with regular blood donor specimens using ISBT specimen labels
Testing must be done by donor-specific processes (not those for clinical patients)
Exclude malaria and HTLV testing.
Testing must be directly interfaced to Medinfo Hematos IIG donor module
CCP COVID antibody testing:
SARS-CoV-2 antibody testing to be performed to determine cut-off for donor eligibility for CCP collection.
Use of donors with antibody levels below threshold is at the discretion of the treating clinician.
Processing:
Aliquoting, pathogen-inactivation, and labelling may proceed if the pre-donation screening results are acceptable.
Storage:
Long-term in minus 80C quarantine freezer
Short-term at 1-6 C just after thawing in quarantine refrigerator
Standard temperature monitoring and alarms apply
Labelling:
The backup manual labelling process applies
The ISBT specimen label will the donor unit number
Outdate will be 6 years if the product is stored at -65C, 1 year if stored at -18C
Product Release:
Orders must be on the PAPER requisition (old Blood Bank Order Form) with a patient prescription and signed by a physician designated to treat COVID patients.
No orders in Cerner
Thawing plasma at 37C upon receipt of order by Transfusion Medicine staff
Signing out component to clinical unit by Transfusion Medicine Staff to locations treating COVID-19 patients.
Information Technology: Medinfo Hematos IIG customized software to be implemented as soon as possible for all processes
Not covered: Transfusion Medicine is NOT responsible for:
Triage of request for convalescent plasma
Pickup and transport of components
References:
Level 1-4 documents for donation, testing, processing, and release of blood components
All blood components are considered medications and are subject to Good Manufacturing Practices as mandated by international accreditation standards. The whole process must be done reproducibly and precisely by specific personnel trained and documented to be competent. This includes collection of convalescent COVID-19 plasma.
Transfusion Medicine will provide staff who are deemed competent for the entire process of the collection, manufacture, and release of this unlicensed, emergency-contingency component.
It will help greatly if all candidates are prescreened to exclude the following candidates:
Administrative:
Donors must come with a valid Qatari identity card: no ID means no screening
Sex:
Males only to minimize the risk for transfusion-associated lung injury TRALI
Donor Feeling:
If the donor does not feel well, he should not come for screening/collection.
Food/Drink:
Donor must have eaten/drunk fluids within 4 hours of arrival for screening/collection.
Medication exclusions:
Antibiotics within the past 14 days
ACE inhibitors in the past 48 hours
Beta blockers
Anticoagulants
Anti-anxiety or other psychotropic medications
Other medications on the attached list
Medical exclusions:
Stable vital signs
History of seizures
History of dementia or other chronic neurologic disorder
Family history of dementia or other chronic neurologic disorder
Significant cardiac arrhythmias
History of hepatitis B, hepatitis C, HIV, brucellosis, Ebola
Travel history:
5 years cumulative residence in Europe including Ireland and France 1980-2001
3 months cumulative residence in the UK (and/or all its territories) 1980-1996
Any visit(s) to West Africa
This is NOT a complete list of criteria. Transfusion Medicine personnel will screen according to the full donor criteria. Thus, donors passing the pre-screening may still be otherwise disqualified based on the detailed process.
I will be posting a detailed series about the manual and software-enhanced COVID-19 processes that I set up in Qatar at HMC Doha in March-April 2020.
In this series I will provide you with screen shots of my Medinfo Hematos IIG software design for each step in the process: collection, processing, testing, inter-depot transfer, and hospital transfusion service/blood bank release.
This GMP-compliant software-enhanced system is based on the manual system I set up in early March 2020 at HMC.
I want to thank Medinfo Hematos IIG for their rapid response to building this parallel system based on my standard processes in so short a time (two weeks) and my special thanks to the software engineering team at Vital Health Technologies, the agent for Medinfo in Qatar.
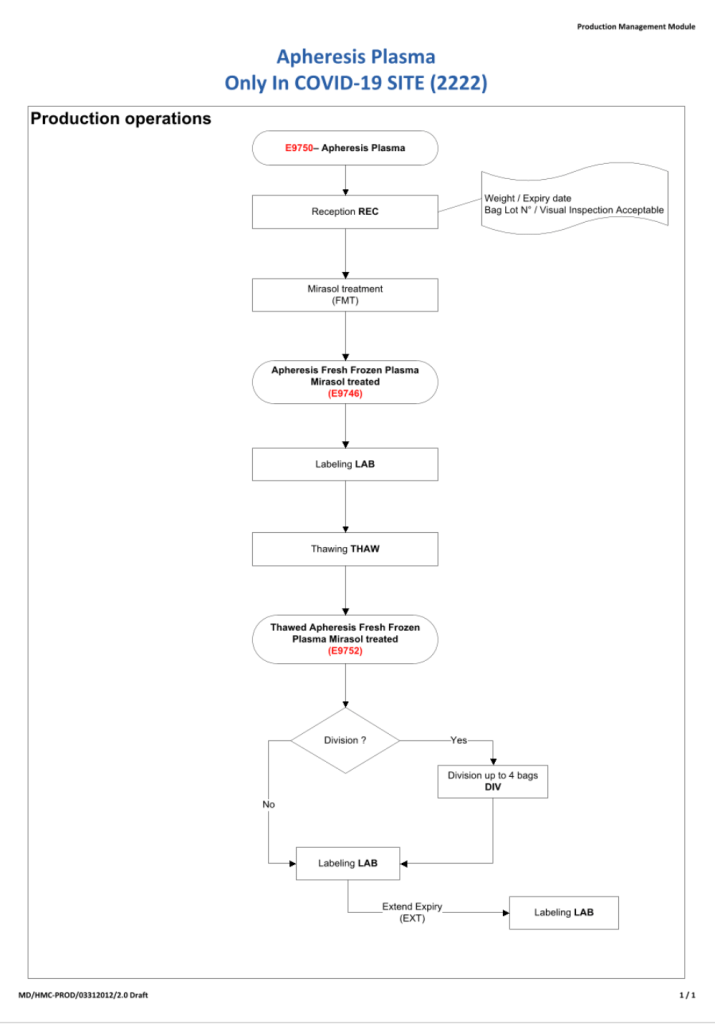
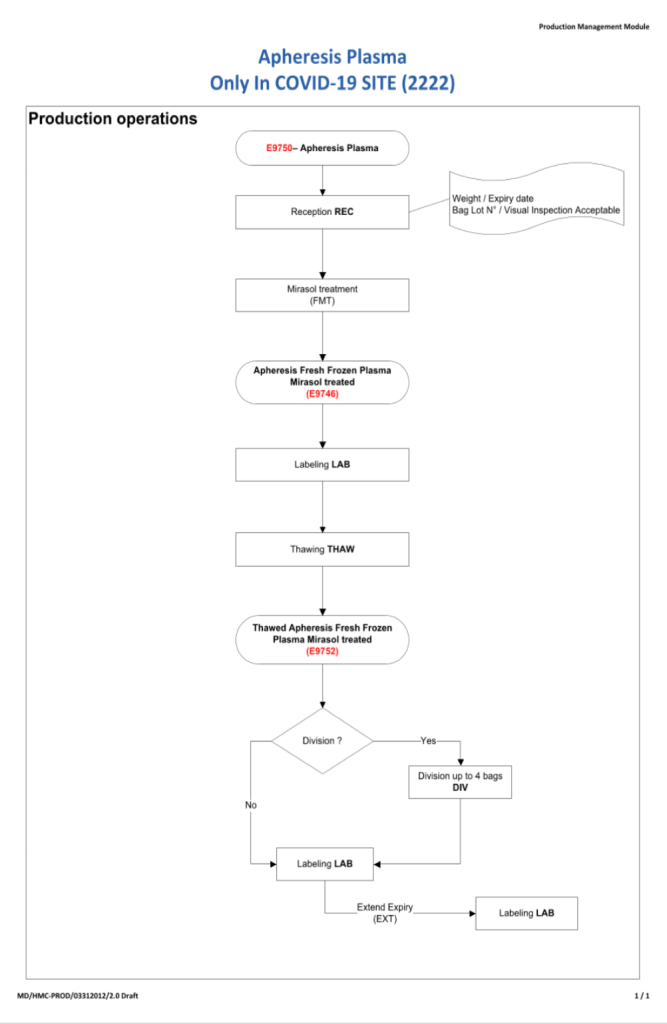
To start the series, I am providing the basic workflow for the system. As is normal in Medinfo software design, a full mapping of the processes are made. This workflow shows the new CCP ISBT codes and the quarantine collection and processing steps. The donor testing (marker and immunohematology) processes are similar to those for regular donor units.
This is basically the same process both manually and in the software. I always say:
A good software process is based on a good manual process!!
Please note the following workflow for our initial discussion.
Since group AB plasma is in short supply, use of group A plasma with low anti-B titers may be substituted based on inventory levels.
Policy:
If the AB inventory is low, we will test group A donors at the time of collection for anti-B titers.
The numbers to be tested will depend on the level of the shortage and the availability of equipment to perform titration.
Use the automated analyzer to perform saline anti-B.
If the saline titer is less than or equal to 1:64, the plasma may be used for recipients of any ABO blood group and will be labelled as group AU—A Universal.
Process the unit routinely and perform pathogen-inactivation.
Medinfo Hematos IIG will only label for universal use if the titer is below the cutoff.
The ISBT label must explicitly show group AU plasma and the actual anti-B titer.
Allocation rules for low-titer group A plasma will be identical to group AB except:
For neonates, preferentially use group AB.
For children < 20 kg, use ABO-compatible plasma (non-group AB) before selecting group AB or if not available, low-titer A in that order.
Donors must have a new anti-B titer performed each donor encounter.
References:
Technical Manual, Current Edition, Bethesda, MD, USA
Standards for Blood Banks and Transfusion Services Current Edition, AABB, Bethesda, MD, USA
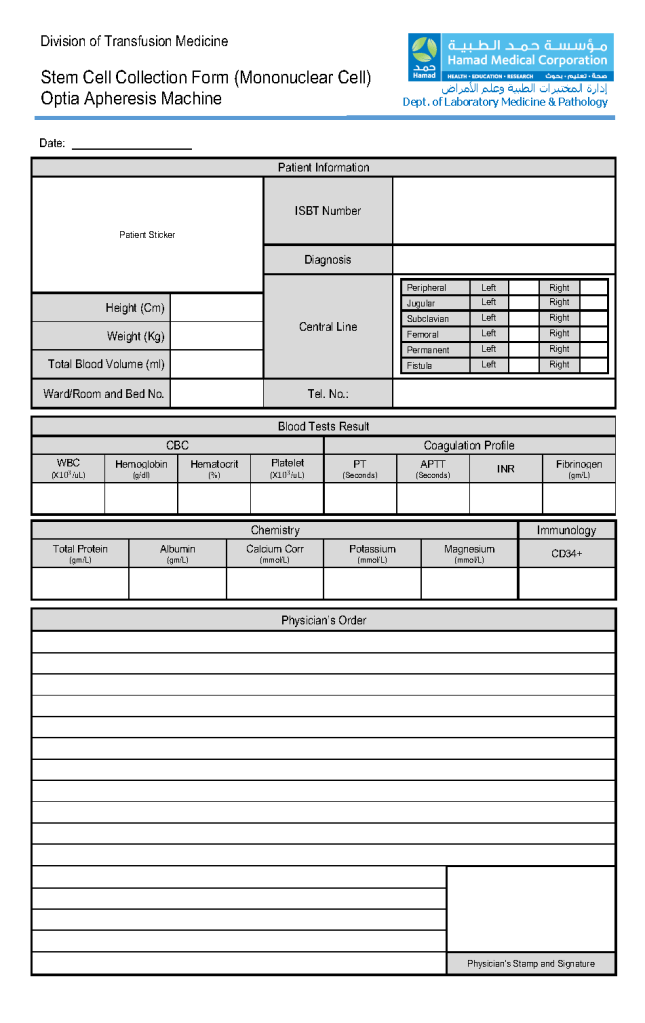
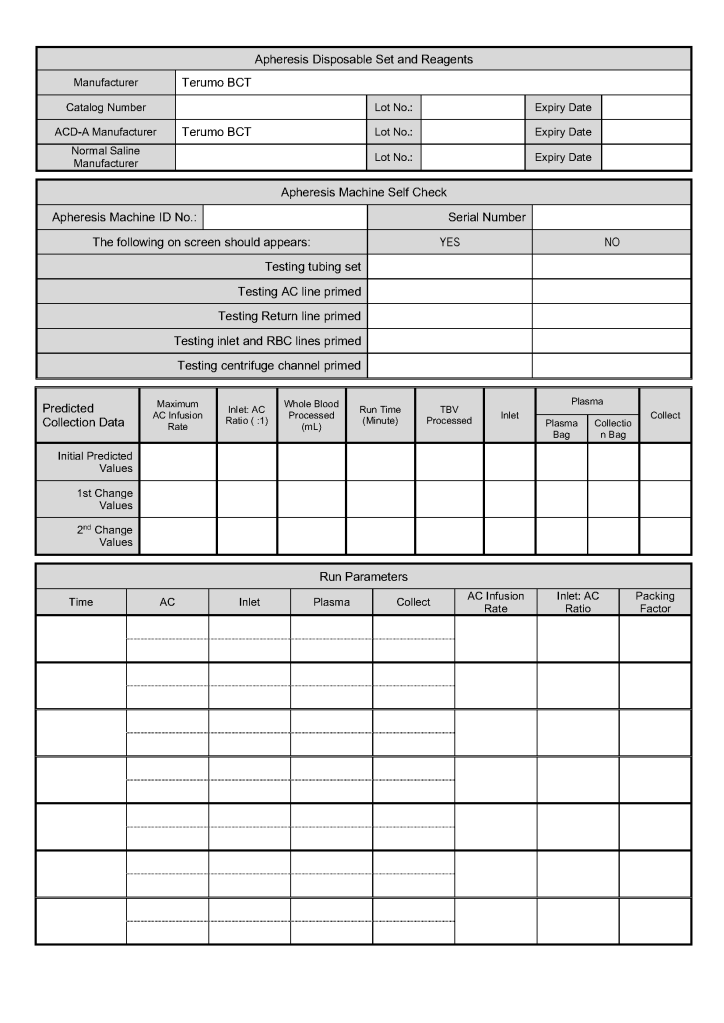
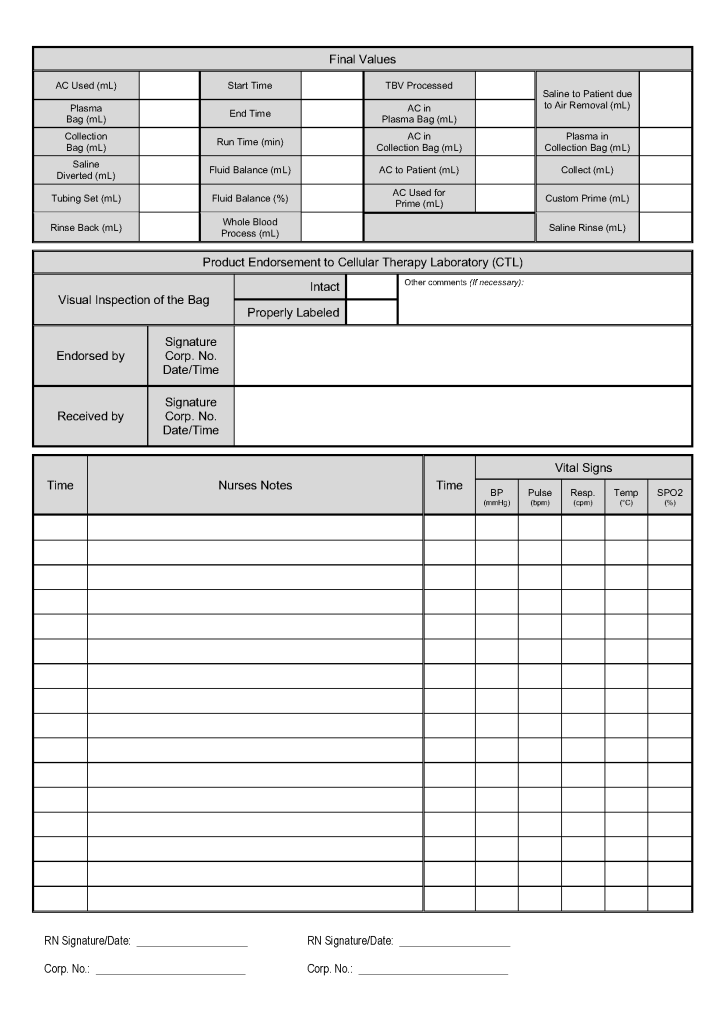
This is a sample of the stem cell therapeutic apheresis form that my apheresis team and I developed. It can be readily made into an electronic form. I want to thank Dr. Saloua Al Hmissi, Apheresis Consultant, and Ms. Mini Paul, Head Apheresis Nurse, for their efforts in making this form a success.
New rules have been approved by US FDA CBER for body fluid exposure, tattooing, body fluid exposure, and body-piercing. By similar logic we will extend this also to HIJAMA. We will not make any changes to our sexual history/practices or history of sexually transmitted disease treatment or clotting factor deferrals (except fibrinogen.)
Policy:
Effective immediately, we will accept donors AFTER THREE MONTHS from the following activities:
HIJAMA (ritual blood-letting)
Tattooing
Body piercing (e.g. piercing for ear-rings)
Contact with blood of another individual through percutaneous inoculation such as a needle stick or through contact with a donor’s open wound or mucous membranes
A TWELVE-MONTH DEFERRAL still applies after receiving a blood component or blood derivative except clotting factors (excluding fibrinogen concentrate.)
Transfusion of clotting factors remains a permanent/indefinite deferral.
Reference:
Revised Recommendations for Reducing the Risk of Human Immunodeficiency Virus Transmission by Blood and Blood Products, Guidance for Industry, U.S. Department of Health and Human Services, Food and Drug Administration, Center for Biologics Evaluation and Research, April 2020
Maintaining an adequate blood supply and expedited compatibility testing are critical in disaster planning. Medinfo Hematos IIG allows us to get dynamic updates of our blood supply and dynamically reallocate blood components as needed.
Policy:
Determinate total available blood supply across all locations by using the Cumulative Stock Display program in Medinfo Hematos IIG.
Recheck stock at least every hour during the disaster.
At each transfusion service site, in conjunction with a Transfusion Medicine Consultant:
Cancel reservations for elective surgical and non-emergency medical cases of affected ABO/D types.
Retain reservations for antigen-matched, oncology, NICU, and high-risk obstetrical cases.
Inform Donor Recruitment/Logistics to send SMS, radio, and television messages for blood donors—all types.
Contact ALL staff and have them report to duty.
At the Blood Donor Center, the Head Nurse, Recruitment, Supervisor, Component Processing, and Supervisor, Marker Testing will contact staff.
At hospital transfusion services, the site supervisor will contact all staff.
Process blood components using automated component technology (Reveos).
Perform all donor marker testing including single-well NAT.
Abbreviation of donor marker testing is only at the discretion of the Division Head, Transfusion Medicine.
Transfusion Services:
Release blood component according to the various protocols as needed:
Massive Transfusion Protocols
Emergency release
STAT
Priority
Routine
Compatibility testing will be electronic, immediate-spin, or full AHG as per our protocols.
References:
Standards for Blood Banks and Transfusion Services, Current Edition, AABB, Bethesda, MD, USA
Guidelines to the Preparation, Use, and Quality Assurance of Blood Components, European Committee (Partial Agreement) on Blood Transfusion (CD-P-TS), Current Edition
All donor unit mislabeling is potentially life-threatening and must be stringently investigated as soon as possible after the discrepancy is detected. Most importantly, if there is one error, there may be possibly ADDITIONAL donor unit errors (e.g. switch of donor tubes or units, etc.). All donor units processed in the same batch must be also quarantined until the discrepancies are resolved.
The blood bank computer system will detect many errors; however, if the donor unit or its samples are mislabeled in the beginning, these may not be detected. Medinfo enforces checks on the final ISBT label and will compare current results to the historical record and will alert to any errors. Additionally, the use of ISBT specimen labels will obviate the risk of barcode reading errors.
Definitions:
Responsible blood bank physician: specialist or consultant physician on-call at the time the discrepancy is detected
Policy Details:
The following steps MUST be performed as soon as possible:
The Component Processing Supervisor or Senior Technologist must be IMMEDIATELY notified of any discrepancy.
The Blood Bank Supervisor will inform the Division Head, Transfusion Medicine. If the Head is not available, notify the Transfusion Medicine on-call.
Quarantine ALL donor units collected and processed in the same batch.
Obtain copies of all testing including photos of the gel/glass bead cards documenting the discrepancy.
Obtain copies of all worksheets used in donor processing for the affected batch.
Perform repeat ABO/D typing of ALL DONOR UNITS in the affected batch. Any further discrepancies must be investigated and resolved.
Identify all staff who were involved in handling the donor unit (phlebotomist, blood bank technicians processing and labelling the unit). Identify those associated directly with the error.
Submit all documents and photos to the Blood Bank Supervisor or designate.
Prepare an occurrence/variance OVA report documenting all the data, findings, and interpretations.
All investigations must be reviewed by the Supervisor, responsible blood bank physician, and one of the senior consultants.
All such investigations must then be finally reviewed and approved by the Division Head, Transfusion Medicine or his designate. Only when the issue(s) are completely resolved and investigation is approved may the donor unit be properly relabeled and released into available stock. Also, only at that time may the other units in the affected batch be released into available stock!!
Photograph the correctly relabeled unit and attach it to the other documentation of the incident.
If the discrepancy cannot be resolved, ALL units in the affected batch must be discarded.
The implicated staff’s personnel record should be reviewed for previous errors. Appropriate disciplinary action should be taken and documented in the personnel record. If a verbal warning is given, it should still be documented in the written record.
If there is a systemic cause for the error, appropriate measures should be taken to minimize reoccurrence.
All actions must be in accordance with the institution’s policies and regulations.