COVID-19 convalescent plasma
Principle:
This policy is based on the 19/1/21 CBER document Updated Information for Blood Establishments Regarding COVID-19 Pandemic and Blood Donation.
Policy:
Note that these rules do not address the special case of COVID-19 convalescent plasma donors.
References:
Updated Information for Blood Establishments Regarding the COVID-19 Pandemic and Blood Transfusion, CBER, US FDA, 19/1/21
When I started my COVID-19 convalescent plasma CCP collection in early March, 2020, there were few antibody tests available. However, I anticipated that eventually we would want to include antibody results with the donor record. Antibody results were not used originally at all in the criteria for CCP acceptability for release.
There are many assays by type of antibody (total, IgG, IgA, IgM) and quantitation by titer and/or signal-cutoff ration S/CO. Any of these parameters may be used to define rules for acceptability to complete production and/or allocate to patients. Instrumentation used for titering/quantitation may be interfaced to the blood bank software.
Here is my generic approach to including these results with the donation record. In Medinfo HIIG, it is possible enter test results retrospectively and these can be used set rules for acceptability. Please consult with my detailed post on using rules against parameters.
All of this is easily implemented since all test information will be stored as parameters. From these parameters we can construct rules for:
Also, one can override the rules if the clinician and the transfusion medicine physician agree. For example, there is a severe shortage of group B CCP so use of low-COVID-antibody titer group B CCP could be allowed.
The key is to build whatever test methodology you use and include the manufacturer’s cutoff for low versus high titer interpretation. These results can be printed on the ISBT label as well. One can easily build multiple methodologies and acceptability criteria if different tests are used at different testing sites in your system—just as can be done for other tests (ABO/D, antibody screen, etc.) If one changes methodologies in the future, Medinfo will still use the same rules that applied for the day of production.
Here are some sample test rules:
Example 1: Total COVID antibody > 160 is high titer:
Example 2: IgG antibody with S/CO ratio > 12 is high-titer:
Example 3: IgG and IgM antibodies must have S/CO > 12:
Another option would be just to record the quantitation for each antibody type and list this on the ISBT label and permit its release regardless of the value. One could also permit low-anti-B titer group A plasma with whatever rules you set up.
This is the early Qatar experience of treating severe COVID-19 using locally produced Covid convalescent plasma CCP. At that time, the plasma was not tested for SARS-CoV-2 antibody levels.
https://drzeydbloodbank.com/wp-content/uploads/2021/01/jmv.26537.pdf
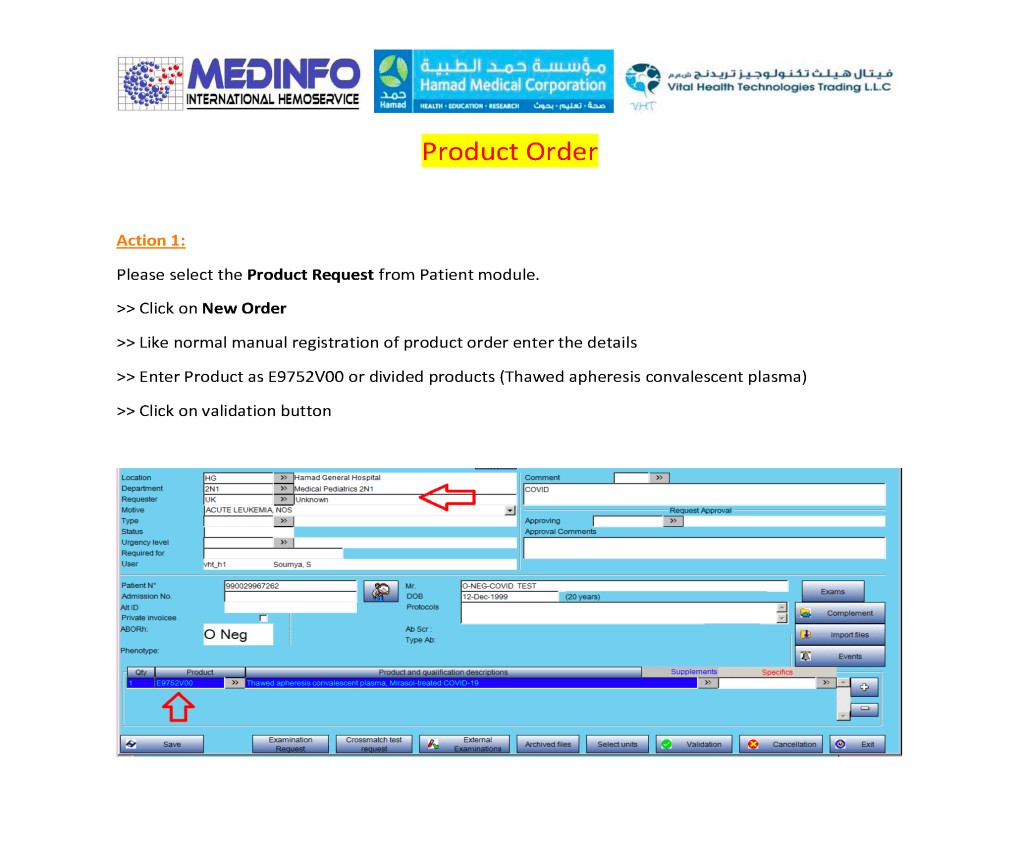
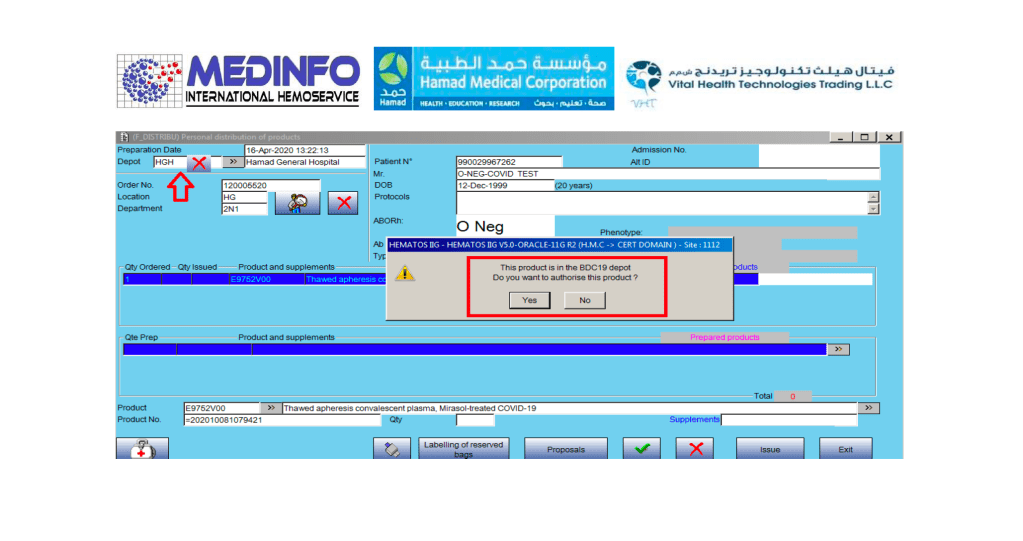
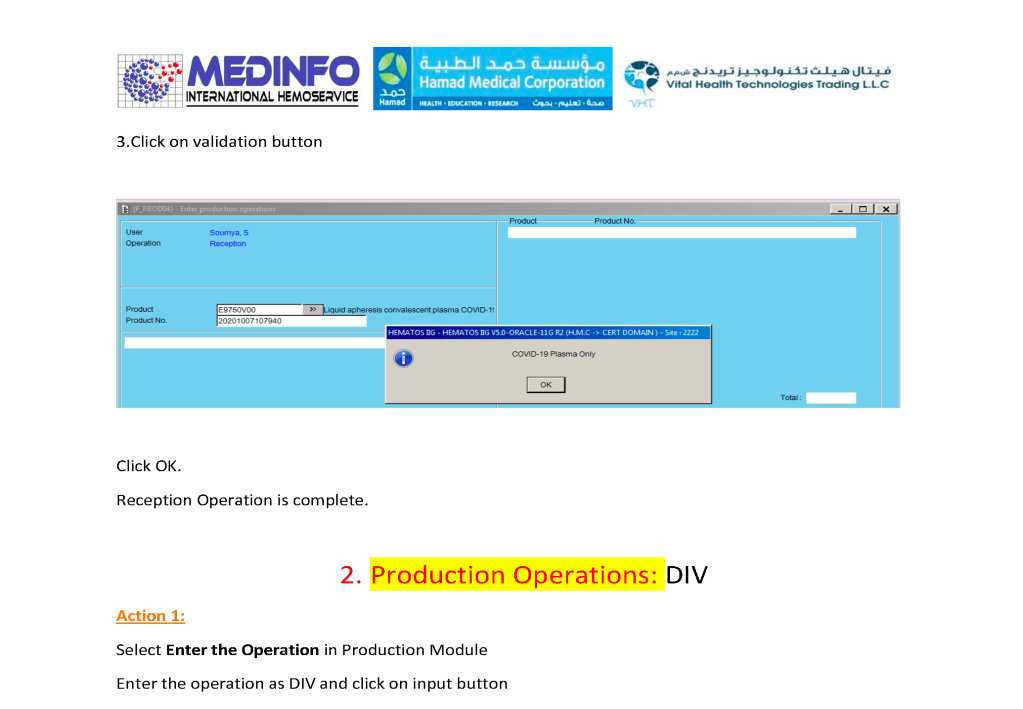
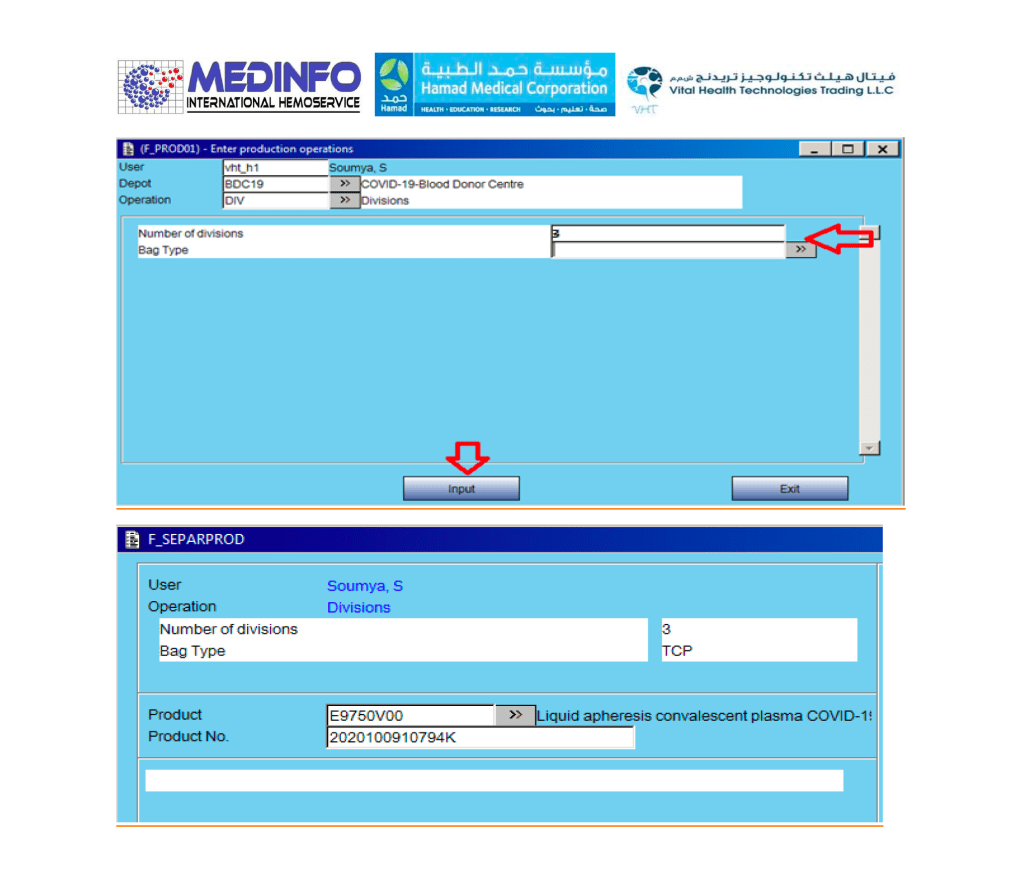
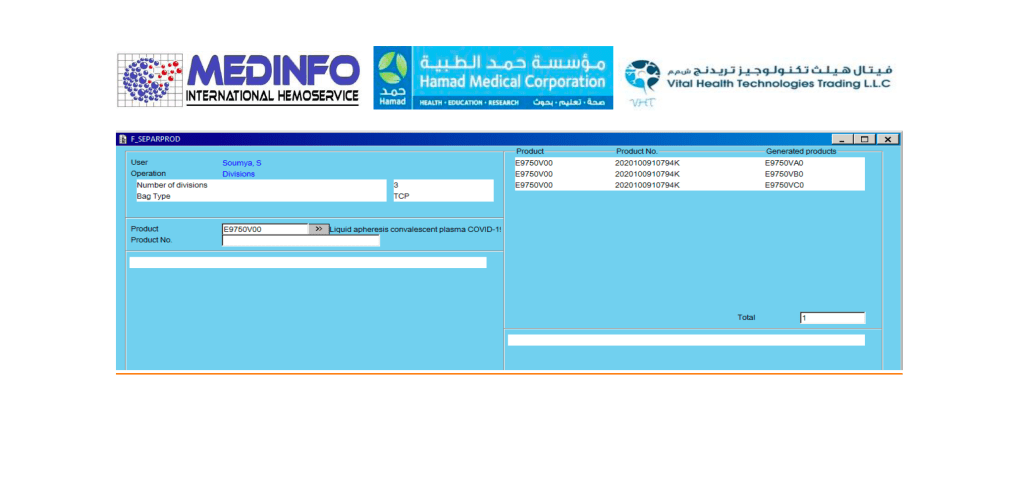
This is the conclusion of a continuing series of posts on the actual Medinfo design of the CCP donation and release processes and covers the transfer of completed units to the hospital blood banks. It highlights specific changes made for the parallel CCP system I developed at HMC Doha.
A blood component is either located at a production site, a destination hospital blood bank site, or in transit. Here a quarantine production site is specified. The actual release process is documented in this post.
In summary, with the exception of the donor marker testing and immunohematology testing, all other CCP processes are handled by special quarantine processes. There are abbreviated marker testing specific for plasma and a special Predonation screening to minimize wastage of the expensive apheresis kits.
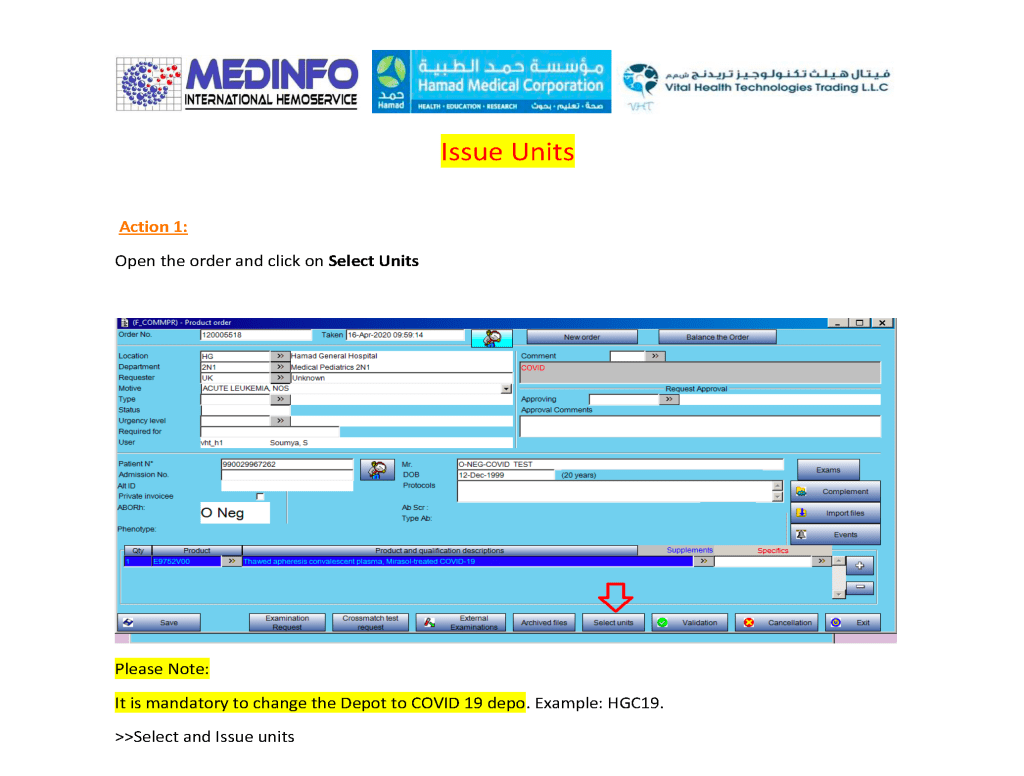
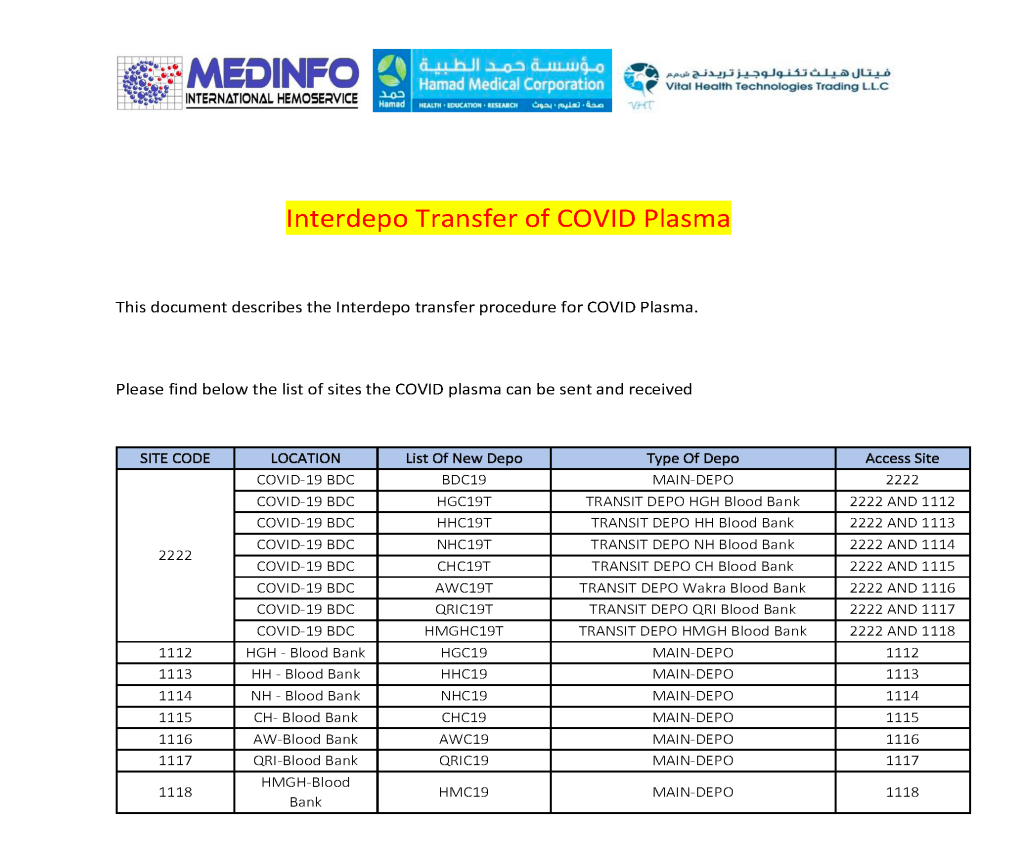
This is a part of a continuing series of posts on the actual Medinfo design of the CCP donation and release processes and covers the transfer of completed units to the hospital blood banks. It highlights specific changes made for the parallel CCP system I developed at HMC Doha.
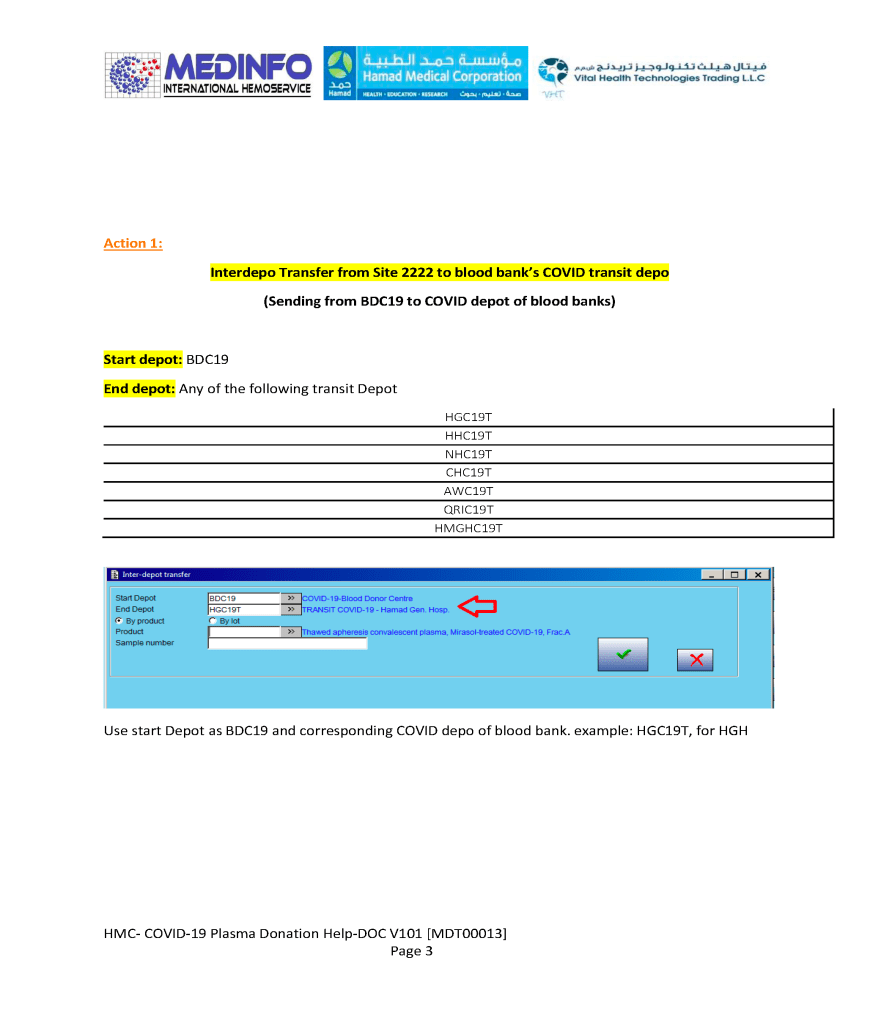
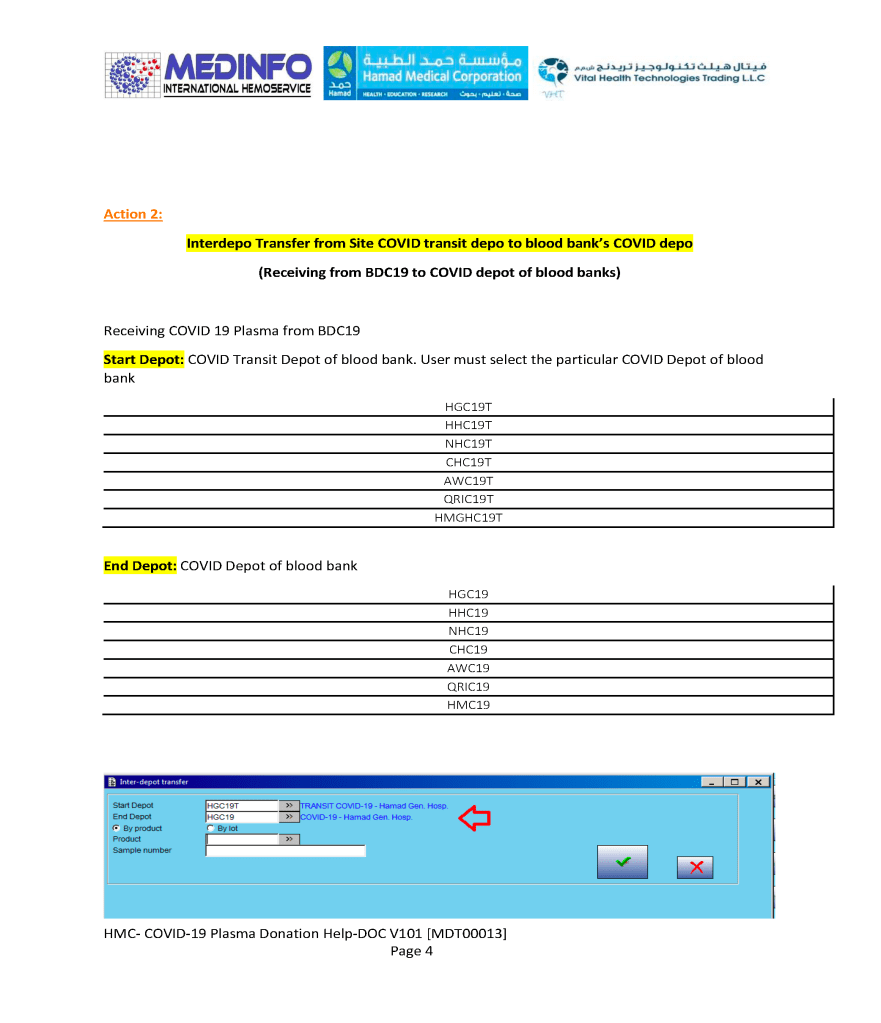
A blood component is either located at a production site, a destination hospital blood bank site, or in transit. Here a quarantine production site is specified. The actual transfer protocols and allowable destination sites are listed for this product.
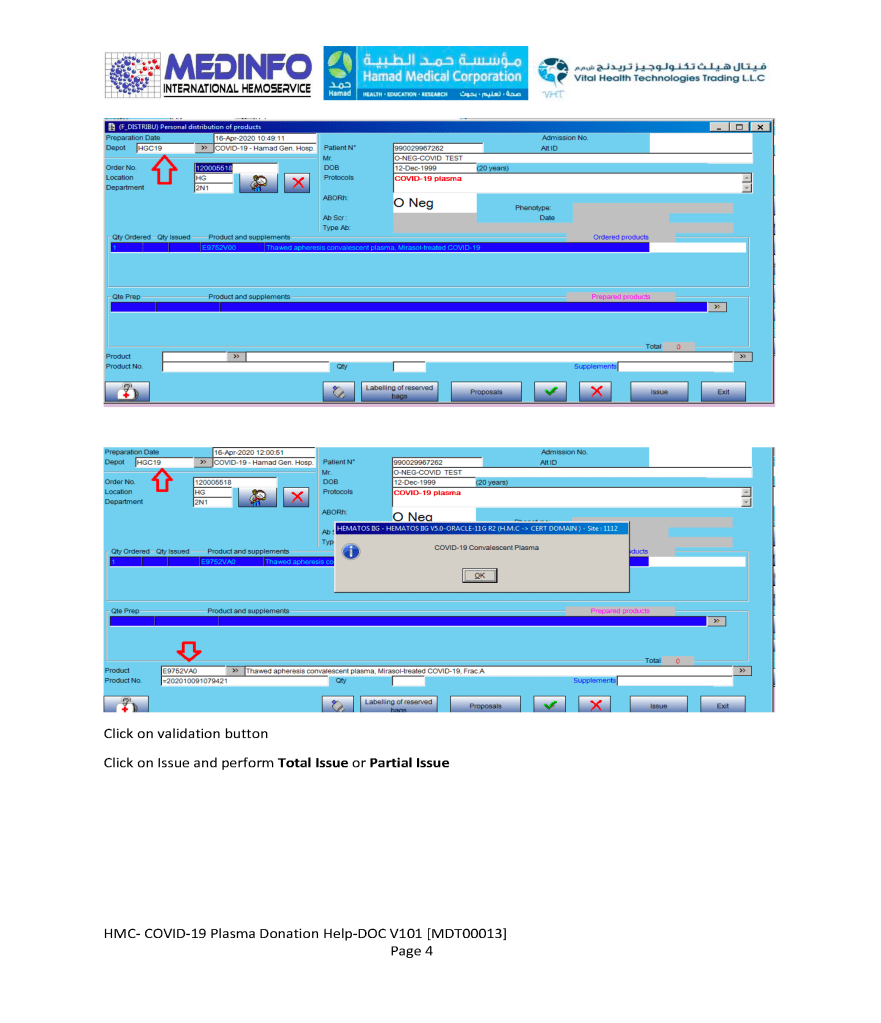
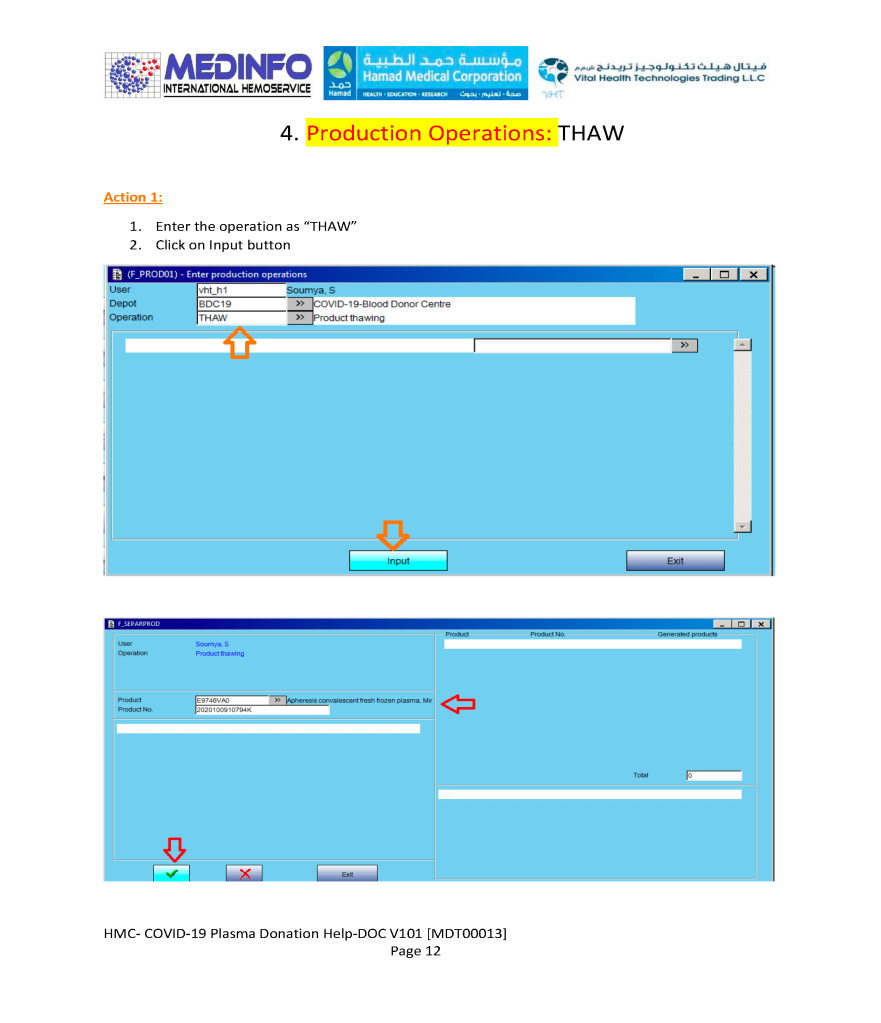
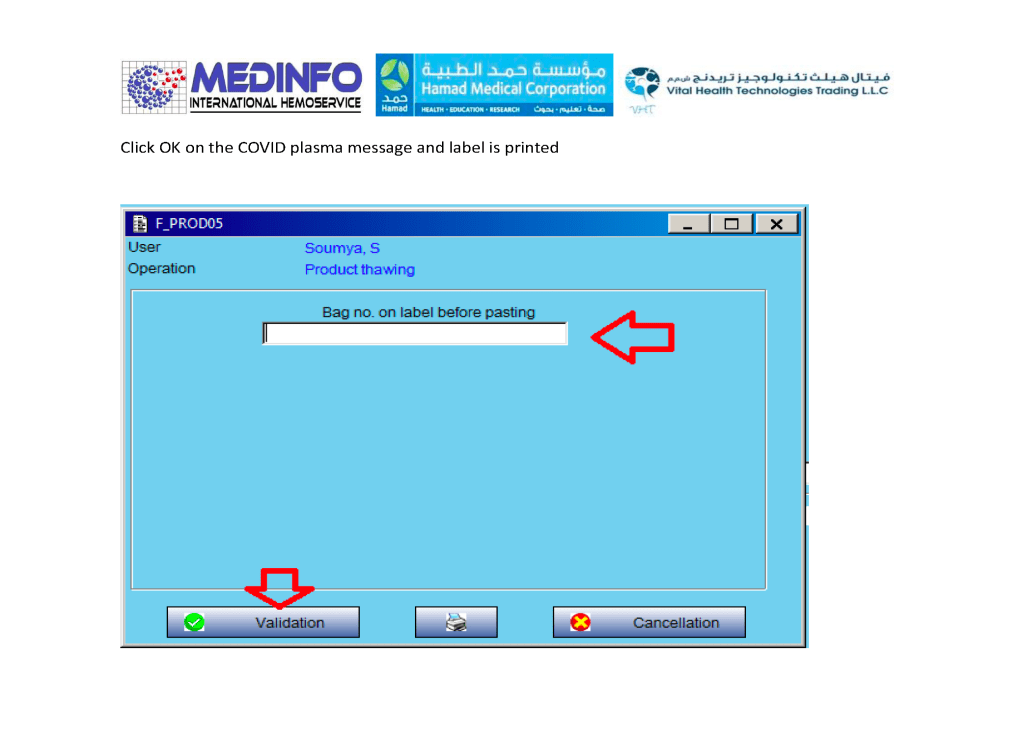
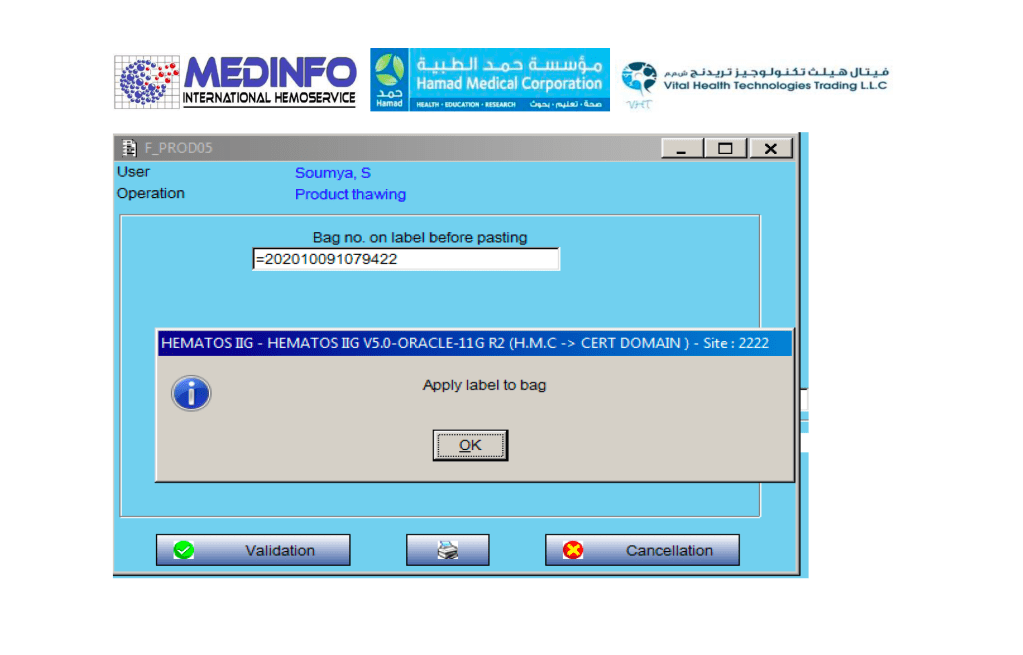
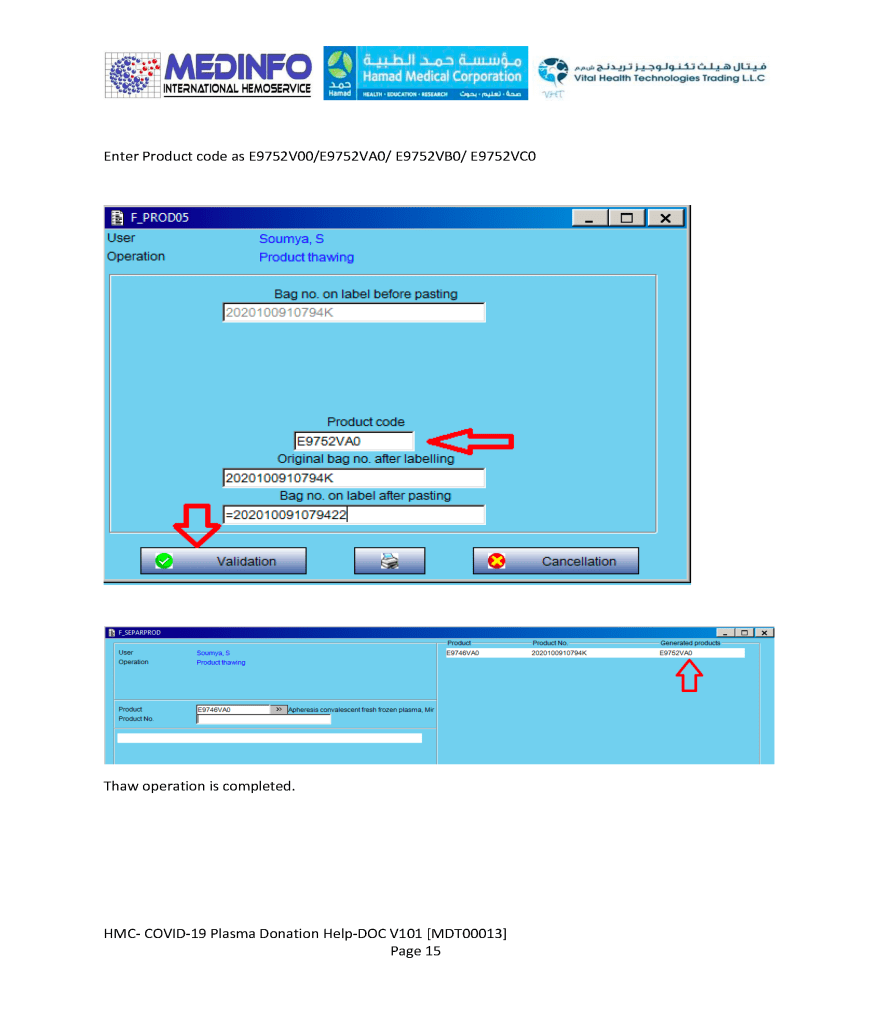
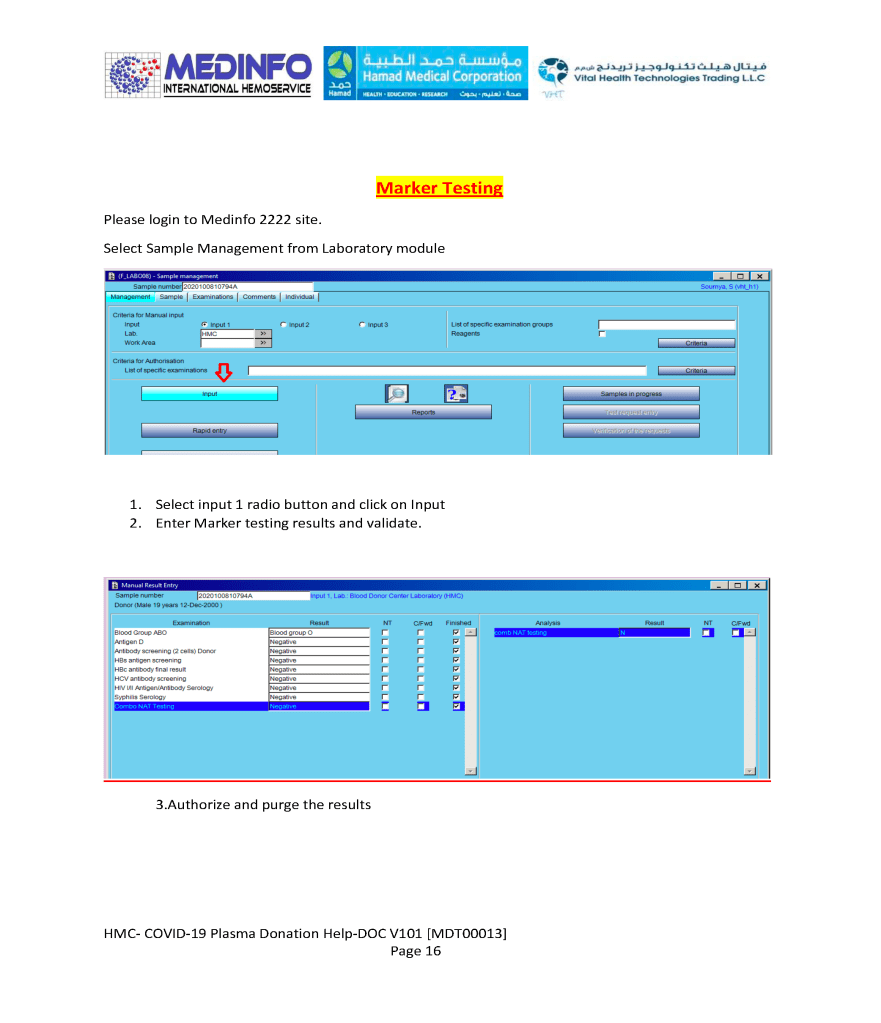
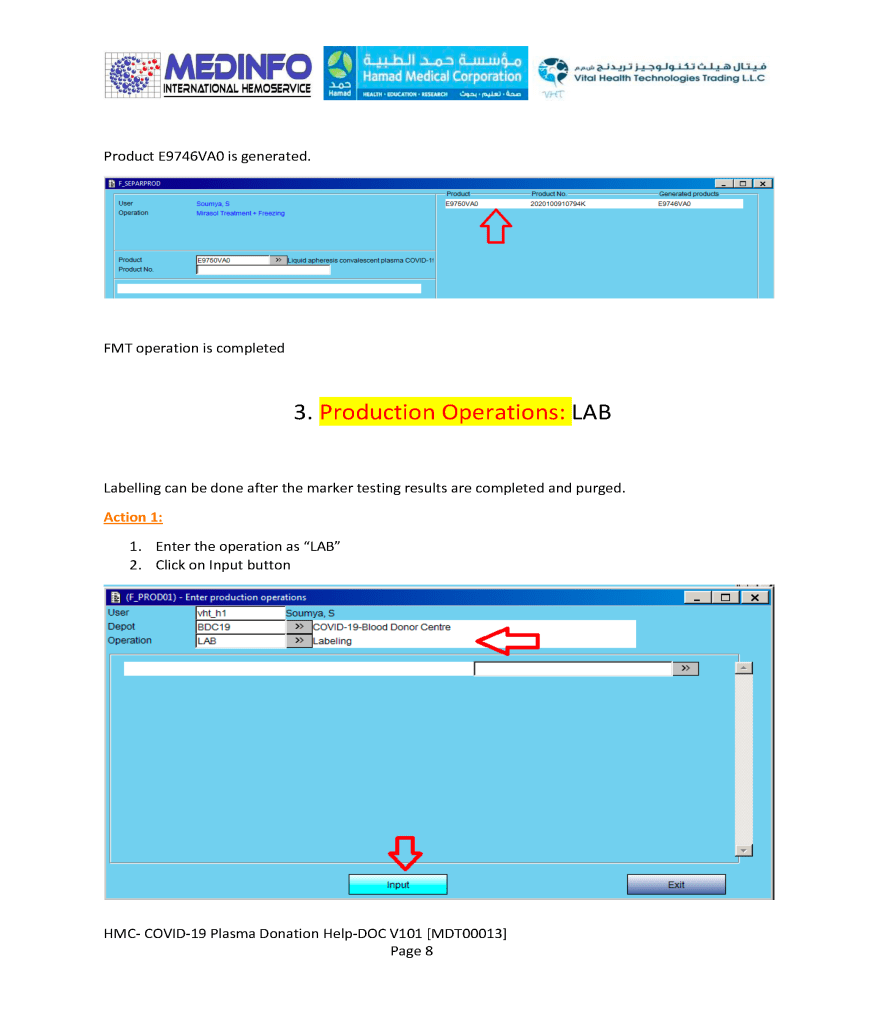
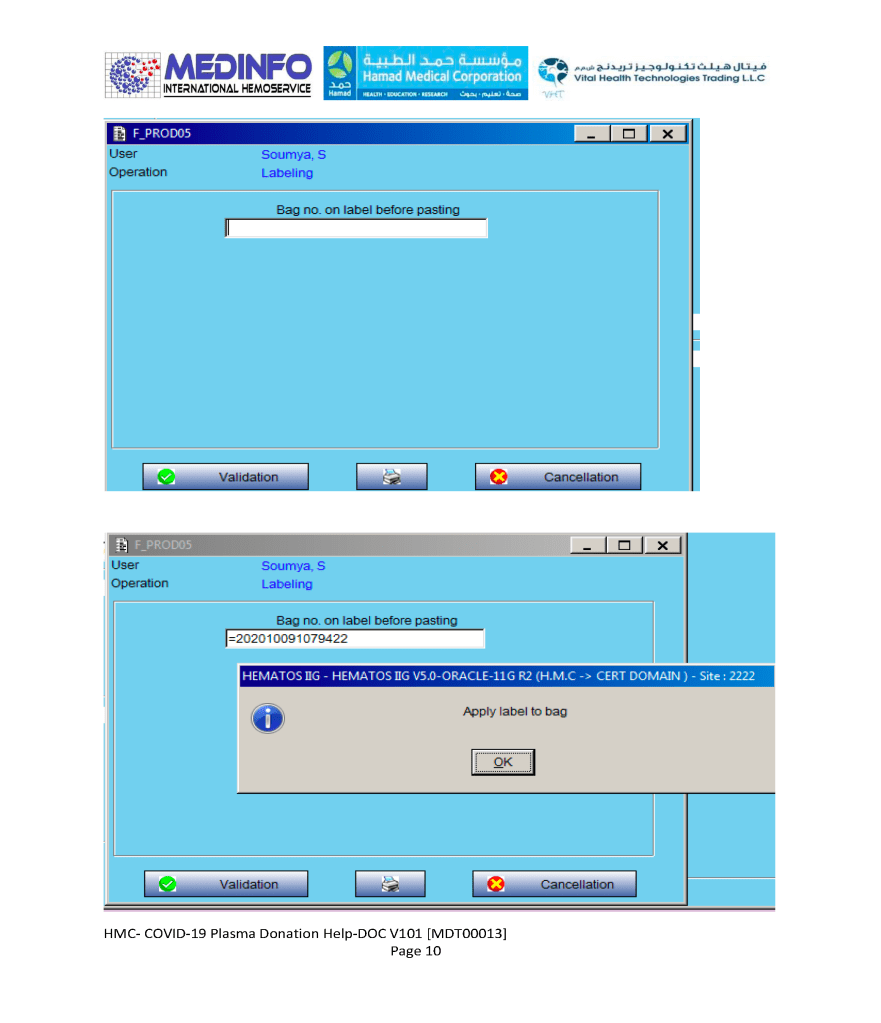
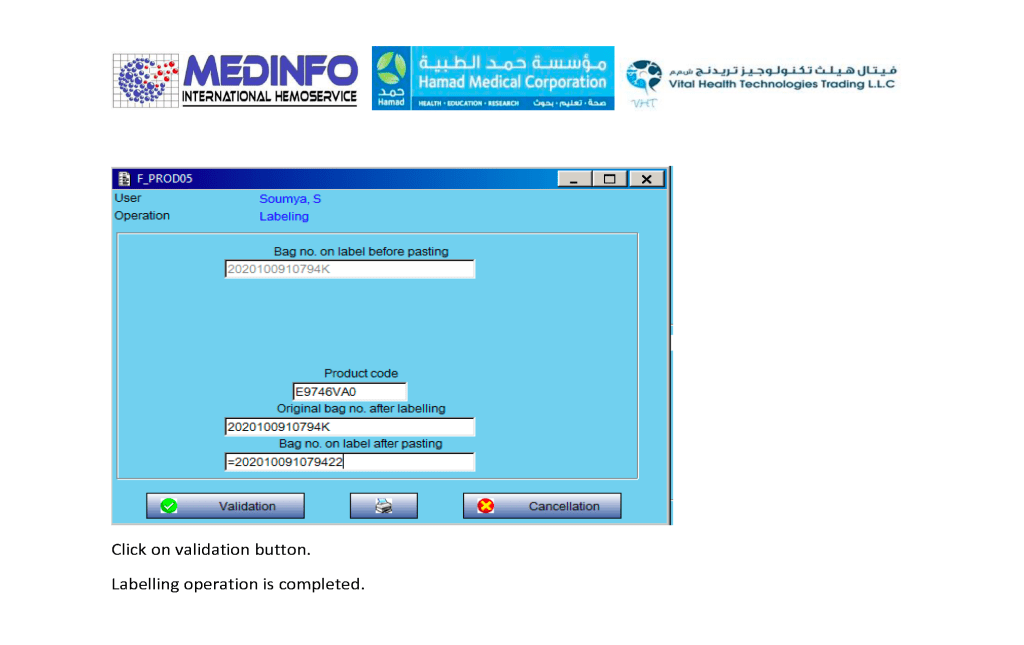
This is a part of a continuing series of posts on the actual Medinfo design of the CCP donation and release processes and covers CCP plasma thawing/labelling and donor marker testing. It highlights specific changes made for the parallel CCP system.
Thus, the machine interfaces for testing are the same as for regular testing and are not included in this document. Likewise, donor immunohematology testing is the same as for regular donors and is not addressed here
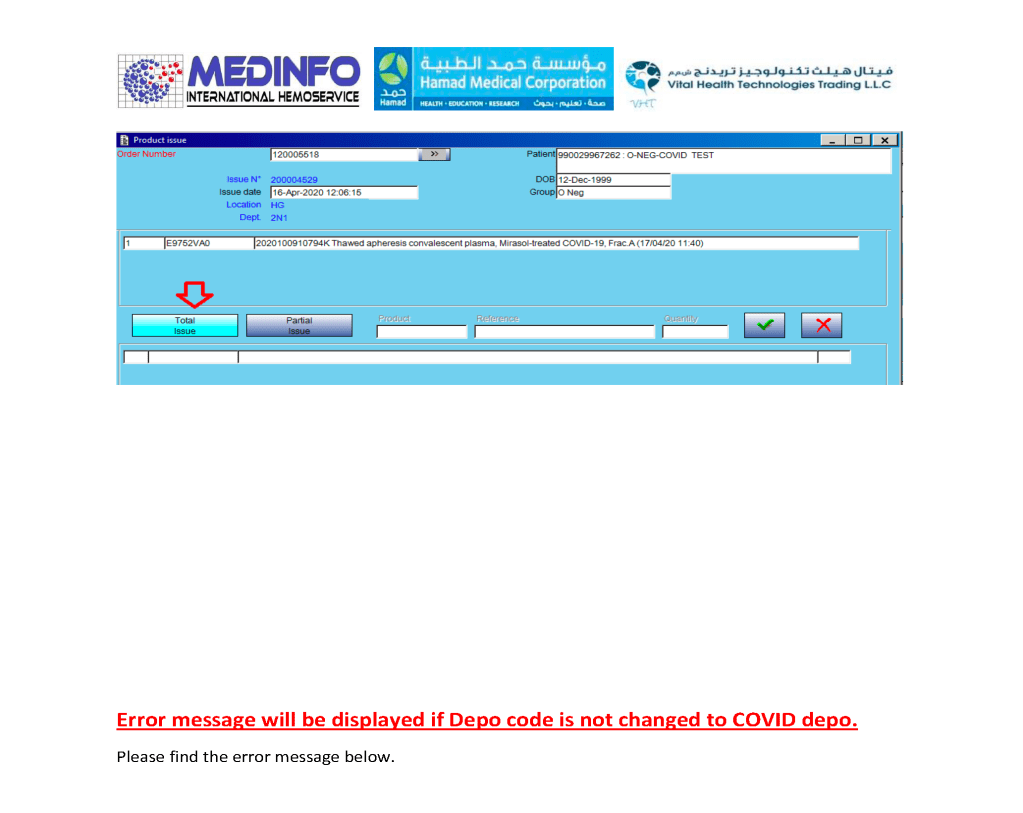
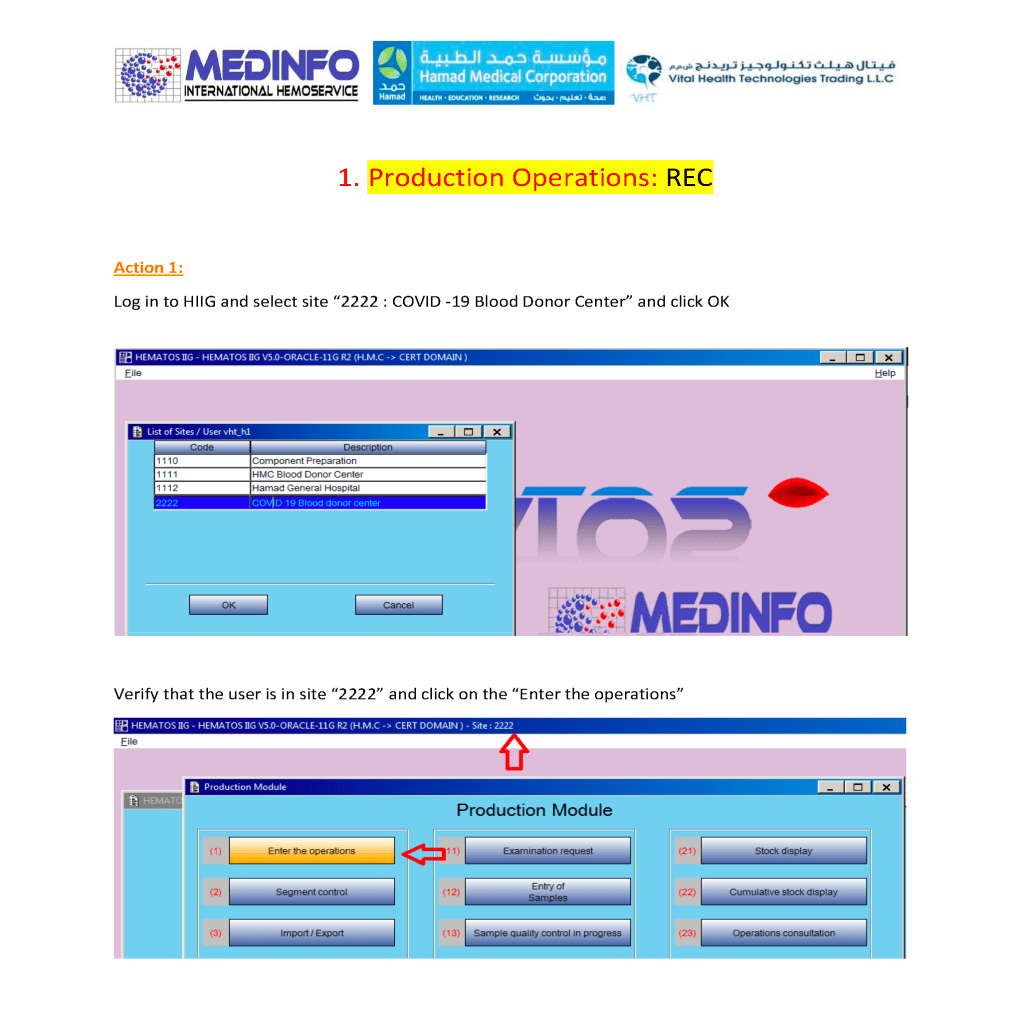
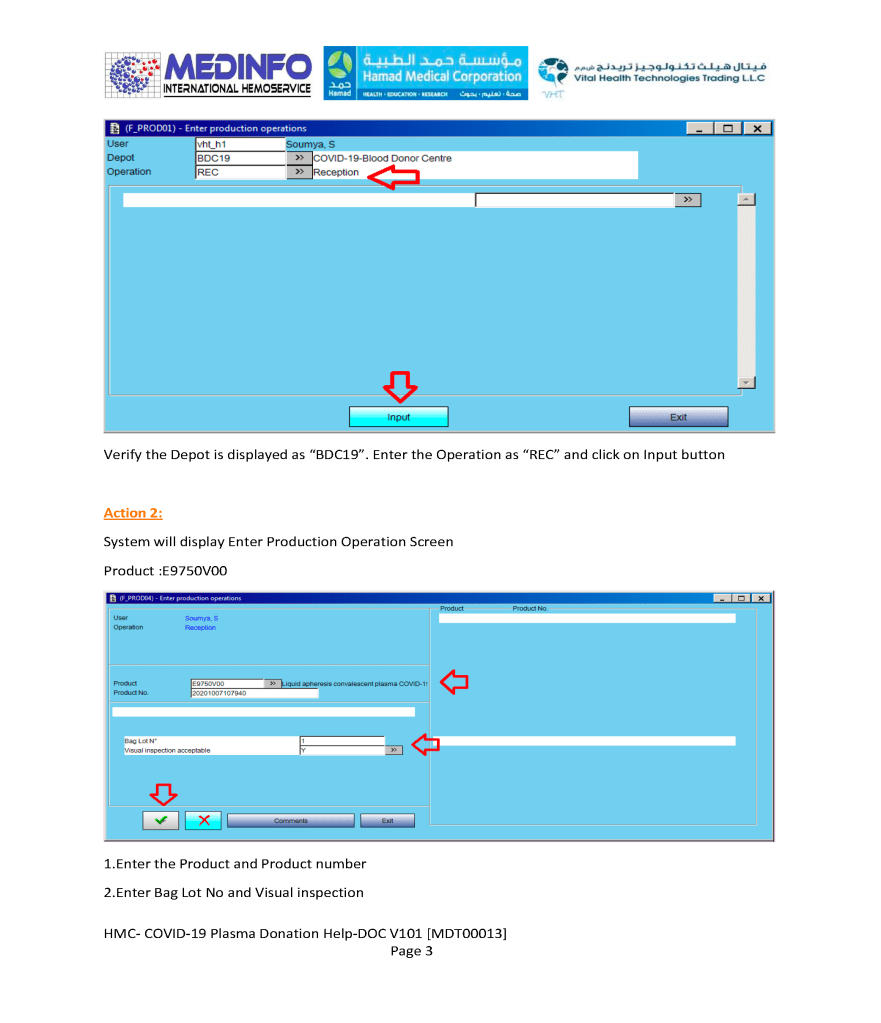
This is a part of a series of posts on the actual Medinfo design of the CCP donation and release processes. The registration of the donor and site, donor questionnaire/collection, and receipt/division of the product were covered in recent previous posts.

This is a part of a series of posts on the actual Medinfo design of the CCP donation and release processes. The registration of the donor and site and donor questionnaire/collection were covered in recent previous posts.
\
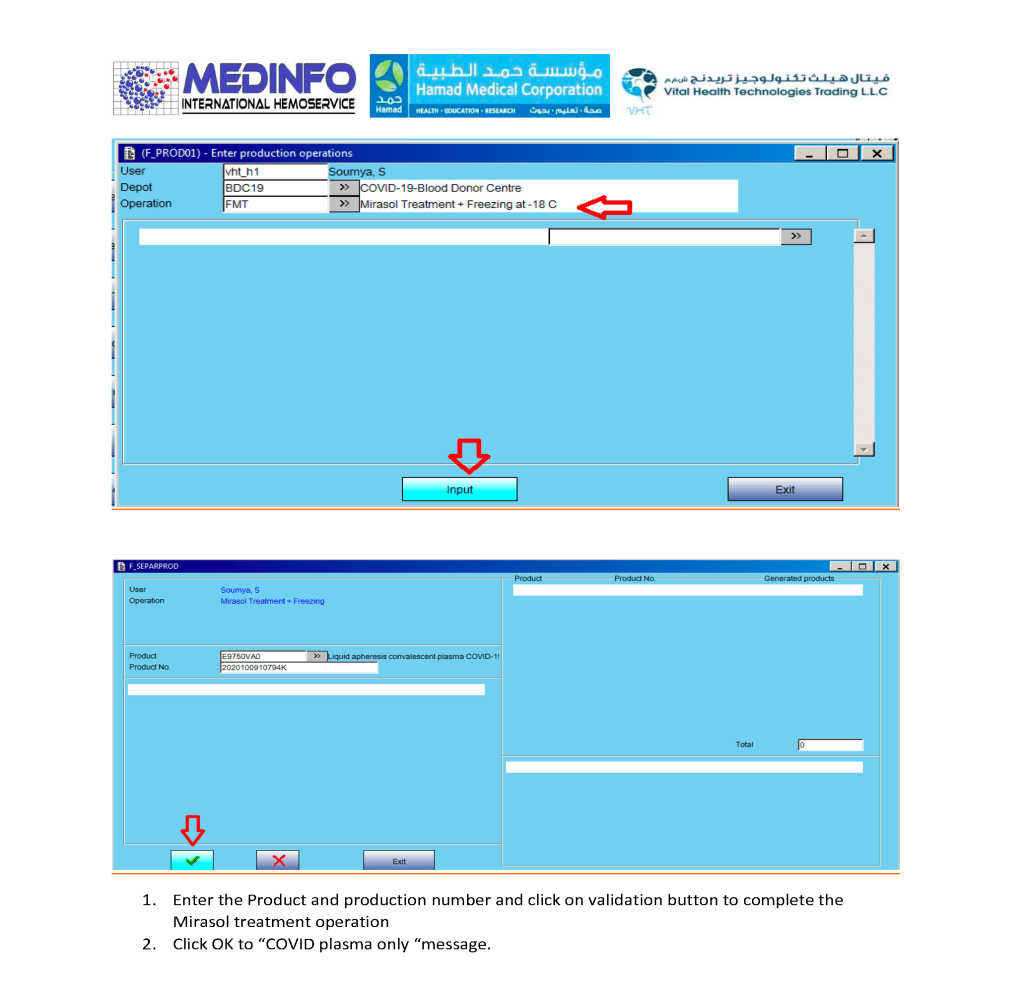
The process (pathogen-inactivation with Mirasol and freezing) wiil continue in a subsequent post.
