Skip to content
Open Menu
Blog (Home)
Transfusion Medicine
Blood Bank IT
COVID-19 Plasma CCP
Plasma Fractionation
About me
Work with me
Contact me
Search
Search for:
Close
Dr. Zeyd Merenkov
Transfusion Medicine, Blood Bank IT, Pathogen Inactivation, Plasma Fractionation, COVID-19 Convalescent Plasma Production
Category:
Transfusion Medicine
Includes patient, donor, apheresis and related IT topics
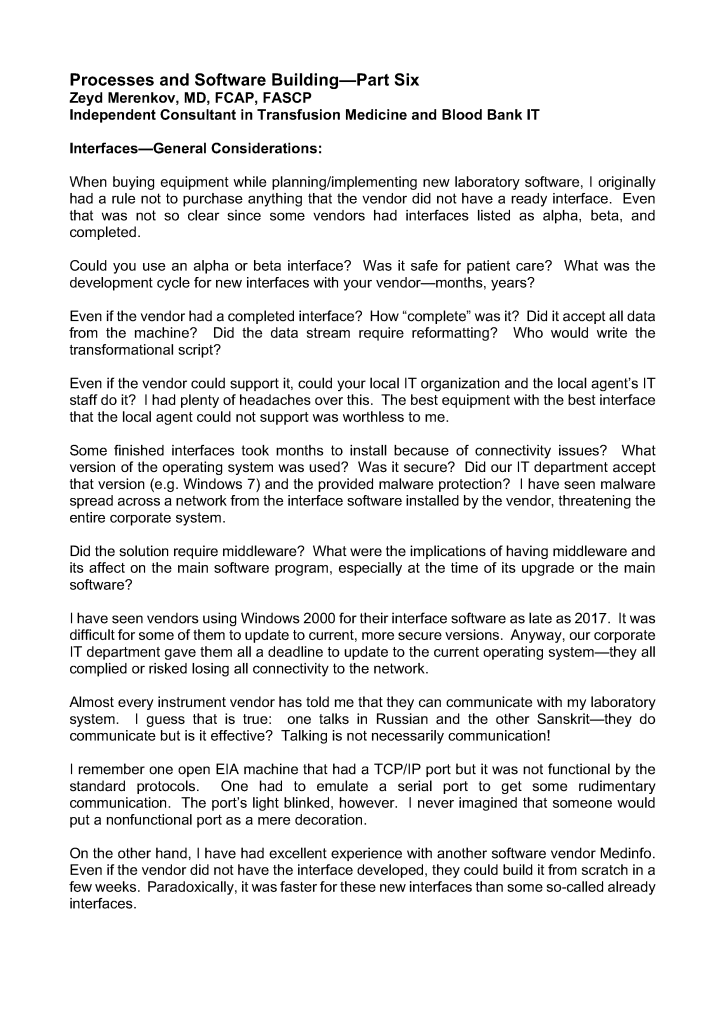
Interfaces–General Considerations
13th Jul 2026
12th Jan 2026
drzeyd
Rules in Software
Image
12th Jul 2026
11th Jan 2026
drzeyd
Rh Incompatible Transfusion Letter, NGHA
11th Jul 2026
9th Jan 2026
drzeyd
Reveos Interface
Image
11th Jul 2026
10th Jan 2026
drzeyd
Reverting to the Original ABO Type
Image
9th Jul 2026
8th Jan 2026
drzeyd
Release of Multiple Components
Image
8th Jul 2026
7th Jan 2026
drzeyd
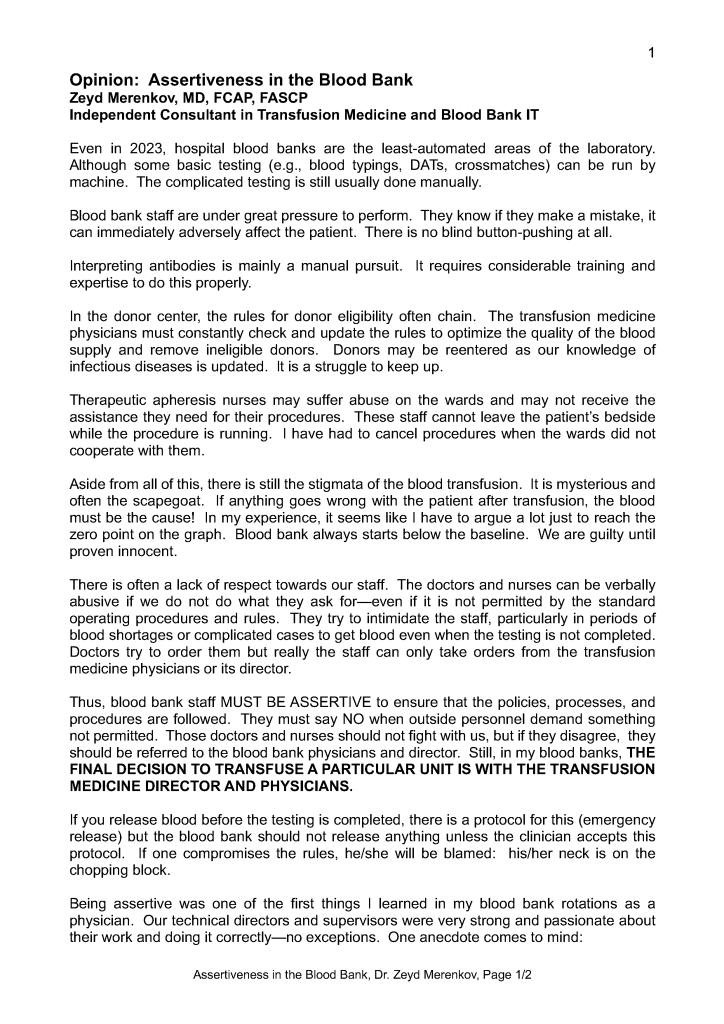
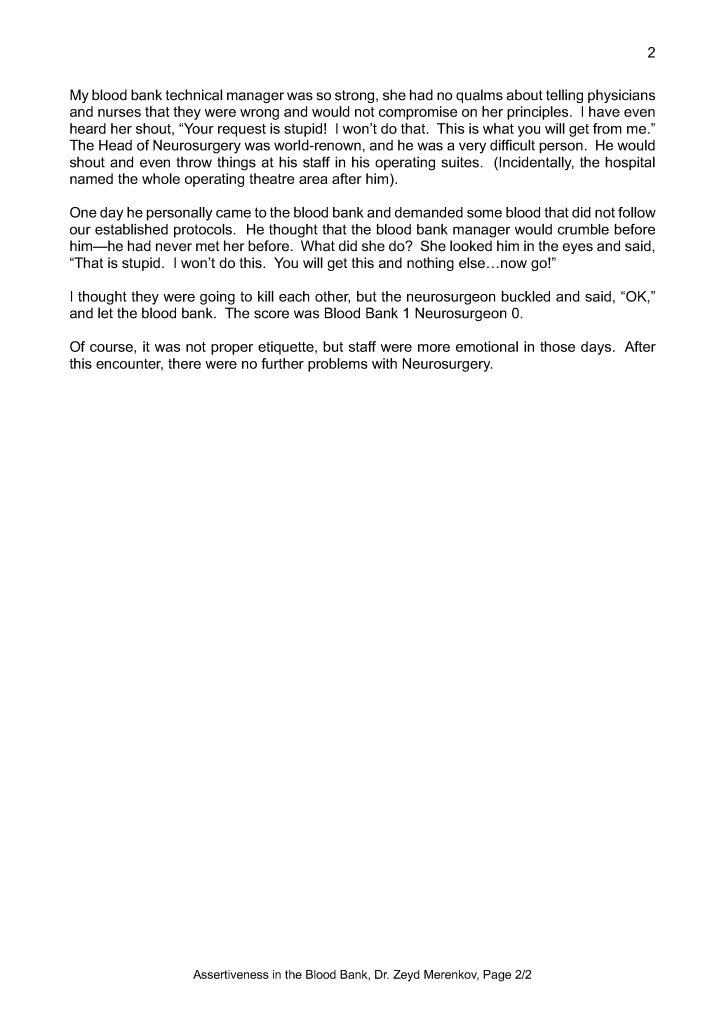
Assertiveness in the Blood Bank
7th Jul 2026
drzeyd
Policy: Handling Registration Errors
Image
7th Jul 2026
6th Jan 2026
drzeyd
Projective Exercise: DAT Pos Eluate Neg
Image
5th Jul 2026
3rd Jan 2026
drzeyd
Projective Exercise 7
Image
4th Jul 2026
2nd Jan 2026
drzeyd
Posts navigation
Older Posts
Newer Posts
Back to top
Subscribe
Subscribed
Dr. Zeyd Merenkov
Join 41 other subscribers.
Sign me up
Already have a WordPress.com account?
Log in now.
Dr. Zeyd Merenkov
Subscribe
Subscribed
Sign up
Log in
Report this content
View site in Reader
Manage subscriptions
Collapse this bar
Loading Comments...
Write a Comment...
Email (Required)
Name (Required)
Website