Category: COVID-19
Includes manual and computer processes for donor, patient, and IT
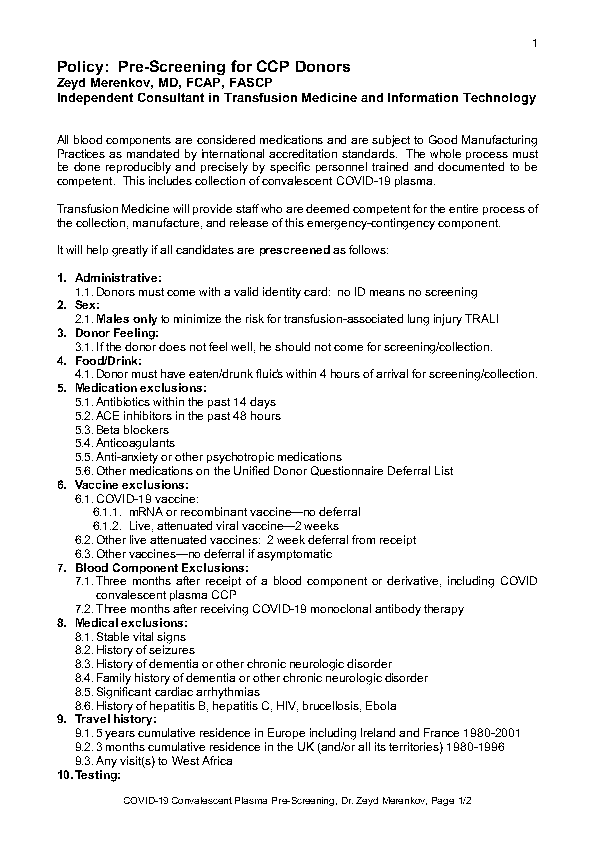
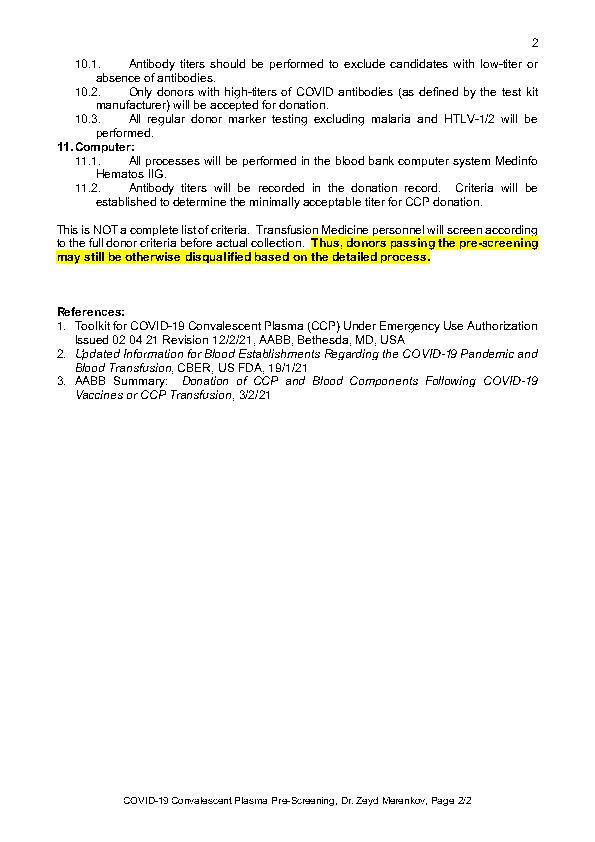
Policy: CCP Donor Pre-Screening
Process: Covid Convalescent Plasma
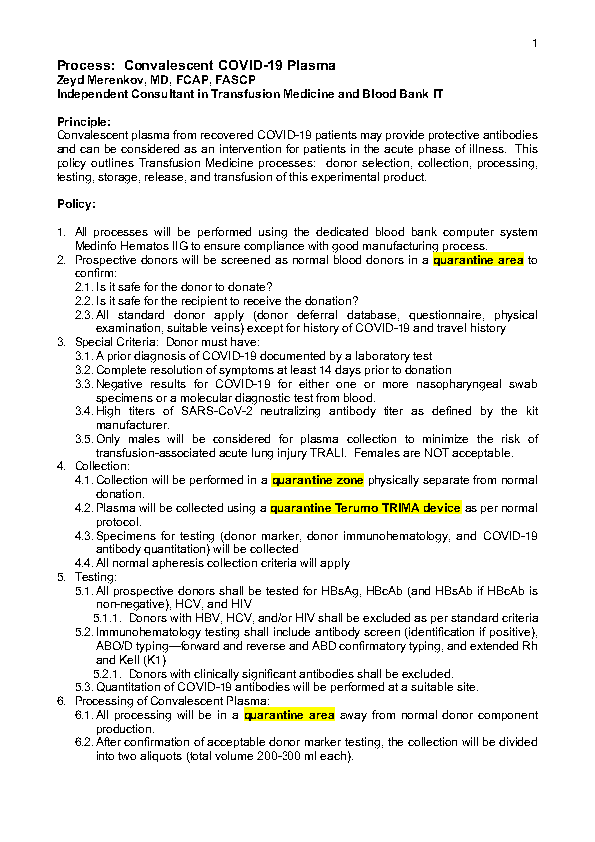
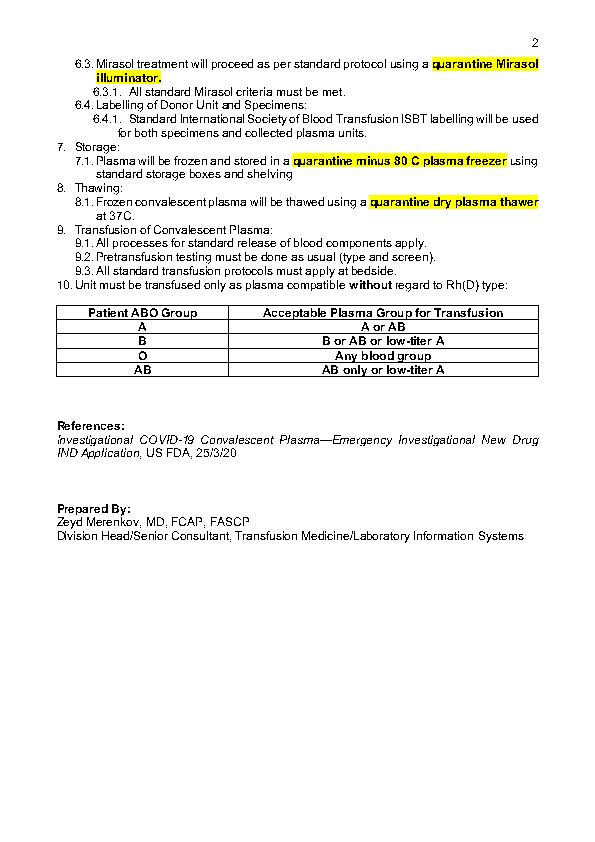
Process: Covid Convalescent Plasma
Policy: COVID Convalescent Plasma Donor Qualification
Policy: Division Head Transfusion Medicine Role in Policy Making
Principle:
The Division Head, Transfusion Medicine and Blood Banks, is responsible for all aspects of transfusion medicine at HMC for the State of Qatar. The following policy documents some of those roles.
Policy:
- The Division Head, Transfusion Medicine HTM, serves as a member of the Corporate Transfusion Committee
- The HTM through the CTC establishes criteria for transfusion of blood components and passes these through the HMC corporate process for establishing official guidelines.
- The HTM reviews blood component requests, especially in times of shortage to triage in conjunction with the Medical Director and Chairperson, DPLM
- The HTM establishes transfusion practices through the interim policies, which are in turn used to prepare processes and procedures through corporate transfusion medicine.
- The HTM serves as Project Manager for the Medinfo Hematos IIG computer system and prepares policies, processes, and procedures for Transfusion Laboratory Information Systems.
References:
Standards for Blood Banks and Transfusion Services, Current Edition AABB, Bethesda, MD, USA
My Opinion: Issues in Transfusion Medicine Software and Component Production
I anticipate that there are several innovations coming or in the process of coming to mainstream blood component production and software. Some of these I have already addressed in some of my previous posts:
Pathogen inactivation: We have had this for over a decade. However, with new emerging pathogens, this will become more important so I expect it will be adopted in many centers where it is not currently being used. I expect we will close the loop and pathogen-inactivated RBCs will be available so all components will be treated. Still, the first-generation pathogen-inactivated RBCs may have reduced shelf life compared to regular, untreated units.
Automated component production: Although this is expensive, it does provide excellent GMP production. It is fast and may provide higher yields, especially for platelets. I expect more centers will adopt this technology, especially in combination with pathogen inactivation.
Blood bank computer software: This software must be considered as dynamically changing, and considerable resources are needed to keep in compliance with ever-changing international regulations and the latest epidemiologic data. Production rules can be strictly and mercilessly enforced by a dedicated blood bank computer software. It can also ensure that the final ISBT label is not applied unless all the production rules (registration, collection, processing, and testing) are met. Manual processing is extremely risky nowadays with all the parameters to be monitored.
Patient Blood Management: Current blood bank software does not adequately address the need for prospective review of component orders. I expect that collaboration will occur between laboratory and blood bank software vendors to fill this gap.
Refrigerated platelets: The pendulum swings back to this component which was used over 40 years ago. Refrigerated platelets suspended in additive solution may be effective up to 14 days for hemostasis in the trauma setting. These platelets are activated so standard 20-24C stored platelets may be preferred for prophylactic transfusions.
Low-titer group A universal plasma: This is already available, but its use will increase because of the low numbers of group AB units available and increased demand. This includes its production for COVID convalescent plasma. Your transfusion medical director must decide what “low titer” means. Also you need a robust way of performing anti-B titers, this may require use of an immunohematology analyzer with titration built-in.
Low titer group O whole blood: Use of this product may reduce the need for components in massive transfusion settings but it requires performing anti-A and anti-B titers on large numbers of units. Your transfusion medical director must decide what “low titer” means. Also you need a robust way of performing anti-A and anti-B titers, this may require use of an immunohematology analyzer with titration built-in. Also, you must decide whether to leukodeplete the whole blood units: few whole blood filters are platelet-sparing.
CCP Collection and Exposure to COVID Vaccines
Principle:
Donor criteria for COVID convalescent plasma collection have been updated by the US FDA. This policy has adapted them to our practice setting.
Policy:
- Donors who donated CCP prior to COVID-19 vaccination may donate following vaccination if they meet remaining donor eligibility criteria.
- Donors who did NOT have symptoms and a positive diagnostic test for COVID-19 prior to vaccination are ineligible to donate plasma after COVID -19 vaccination.
- Individuals may donate CCP for up to 6 months after resolution of COVID-19 symptoms regardless of what their antibody levels are at 6 months.
- Only high-titer units (as defined by the reagent manufacturer) may be used for patient treatment.
Reference:
Regulatory Update: FDA Officials Provide Insight on High-Titer CCP, Donor Eligibility Following Vaccination, 9/2/21, AABB, Bethesda, MD, USA
COVID-19 Donor Qualification
Principle:
This is the latest update on donor qualifications during the COVID-19 pandemic and addresses issues about COVID-19 vaccination, COVID convalescent plasma use and donation, return of donors into the donor pool after COVID-19 vaccination. All of this information is subject to change as new regulations are released.
Policy:
- All donors must be in good health and meet all donor eligibility criteria at the time of the donation.
- Individuals diagnosed with COVID-19 or who are suspected of having COVID-19, and who had symptomatic disease, must refrain from donating blood for at least 14 days after complete resolution of symptoms.
- Individuals who had a positive diagnostic test for SARS-CoV-2 (e.g., a nasopharyngeal swab), but never developed symptoms, must refrain from donating at least 14 days after the date of the positive test result.
- Individuals who are tested and found positive for SARS-CoV-2 antibodies, but who did not have prior diagnostic testing and never developed symptoms, can donate without a waiting period and without performing a diagnostic test (e.g., a nasopharyngeal swab).
- Individuals who received a non-replicating, inactivated, or mRNA-based COVID-19 vaccine can donate blood without a waiting period.
- Individuals who received a live-attenuated viral COVID-19 vaccine, must refrain from donating blood for 14 days after receipt of the vaccine.
- Individuals who are uncertain about which COVID-19 vaccine was administered must refrain from donating for 14 days if it is possible that the individual received a live-attenuated viral vaccine.
- Individuals who received monoclonal antibodies should be deferred for three months from the last dose.
- Donors who have received blood components, including COVID-19 convalescent plasma are deferred for 3 months since the last transfusion.
- Recovered COVID-19 patients who are eligible to donate CCP and receive an approved COVID-19 vaccine may donate if they:
- Had symptoms of COVID-19 and a positive test result from an approved diagnostic test
- Received the COVID-19 vaccine after the diagnosis of COVID-19
- Are within 6 months after complete resolution of COVID-19 symptoms
References:
- Summary: Donation of CCP, Blood Components, and HCT/Ps Following COVID-19 Vaccines or Treatment with CCP or Monoclonals, Updated 3/2/21, AABB, Bethesda, MD, USA
- Updated Information for Blood Establishments Regarding COVID-19 Pandemic and Blood Donation, US FDA, 19/1/21
- Toolkit for COVID-19 Convalescent Plasma (CCP) Under Emergency Use Authorization Issued 02 04 21 Revision 12/2/21, AABB, Bethesda, MD, USA
