Donor marker testing algorithms are very complex and serve multiple objectives:
Is the blood safe for the recipient, i.e. minimize likelihood of disease transmission?
How do we to counsel the affected donor? Does he need referral for treatment or follow-up?
Often the donor disposition is unclear based on a single encounter and a temporary deferral must be triggered so the current results may be compared to future ones, usually after 8 weeks, 6 months, or one year—depending on the pathogen in question.
Regretfully, the significance of reactions that do not meet the criteria for positivity may be unclear. It is very difficult to explain to the donor that he has abnormal results and cannot donate but we as physicians do not know what their significance is.
Thus, the testing algorithms may trigger current additional testing, temporary deferral with repeat of testing at some future date, or permanent deferral.
At my previous positions, I started with the AABB/FDA CBER Uniform Donor Questionnaire UDQ and then modified it to include some advanced methodologies not available in the USA.
In the next series of posts I will elaborate on the processes developed for this for each marker.
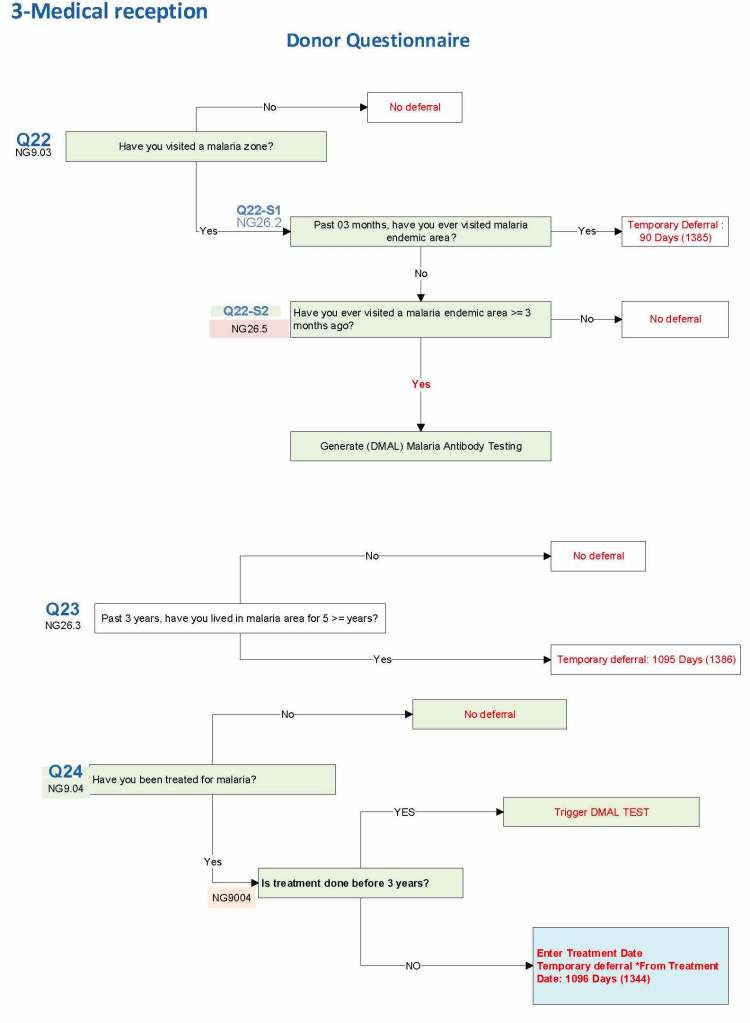
I started building this using the Uniform Donor Questionnaire UDQ from the AABB; however, I modified it to include coverage for Chikungunya, Zika, etc. and to include enhanced processes for malaria based on the Australian Red Cross.
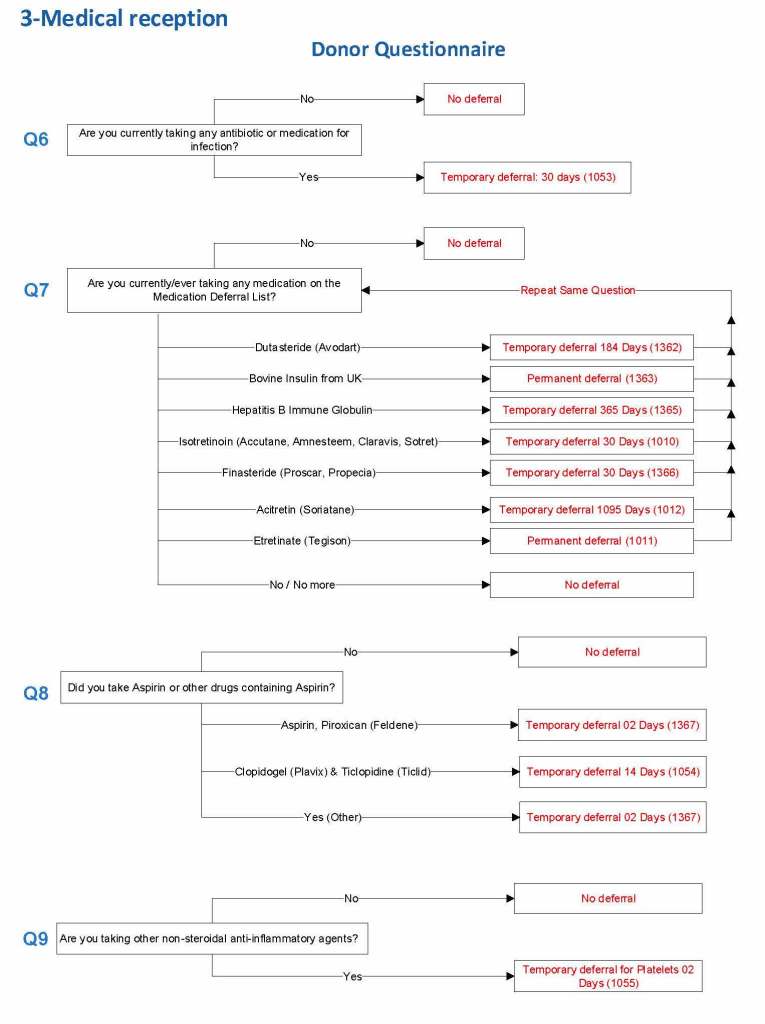
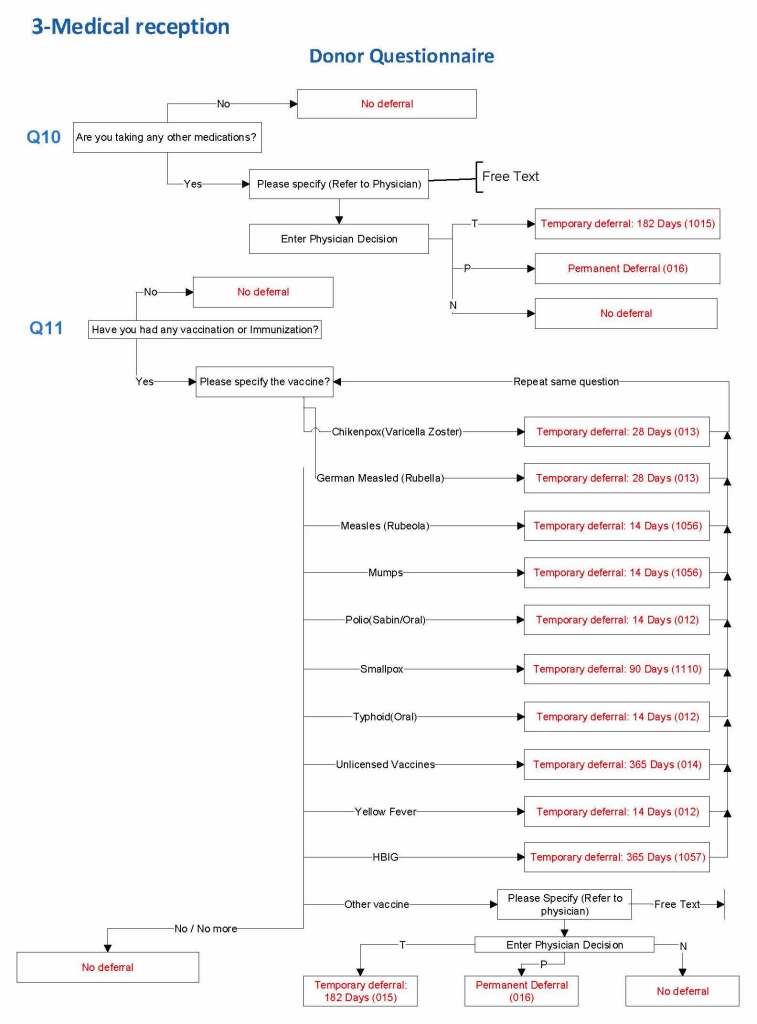
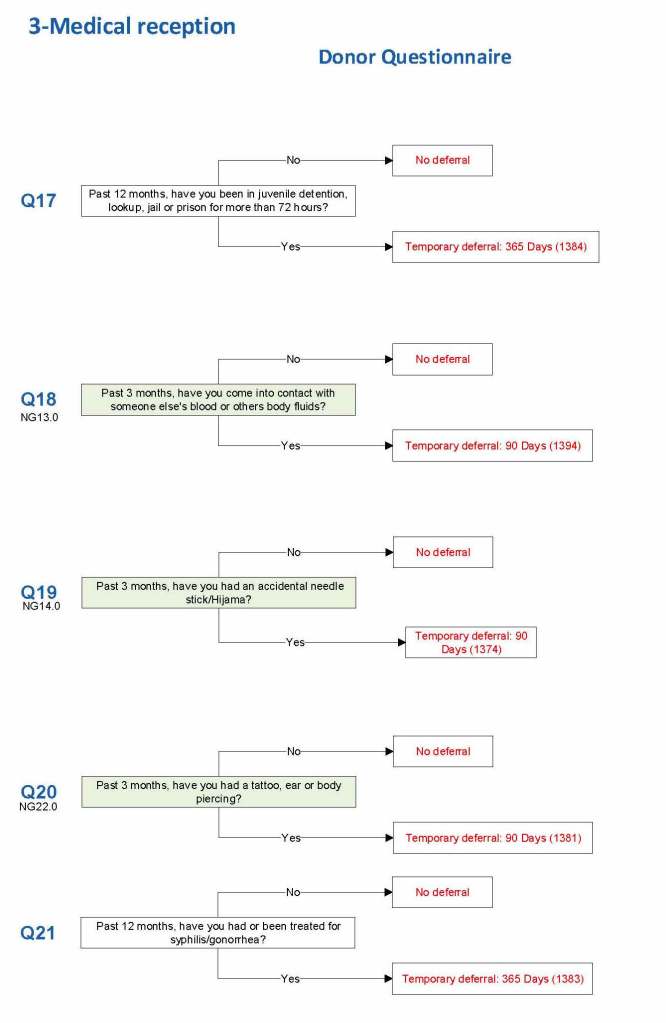
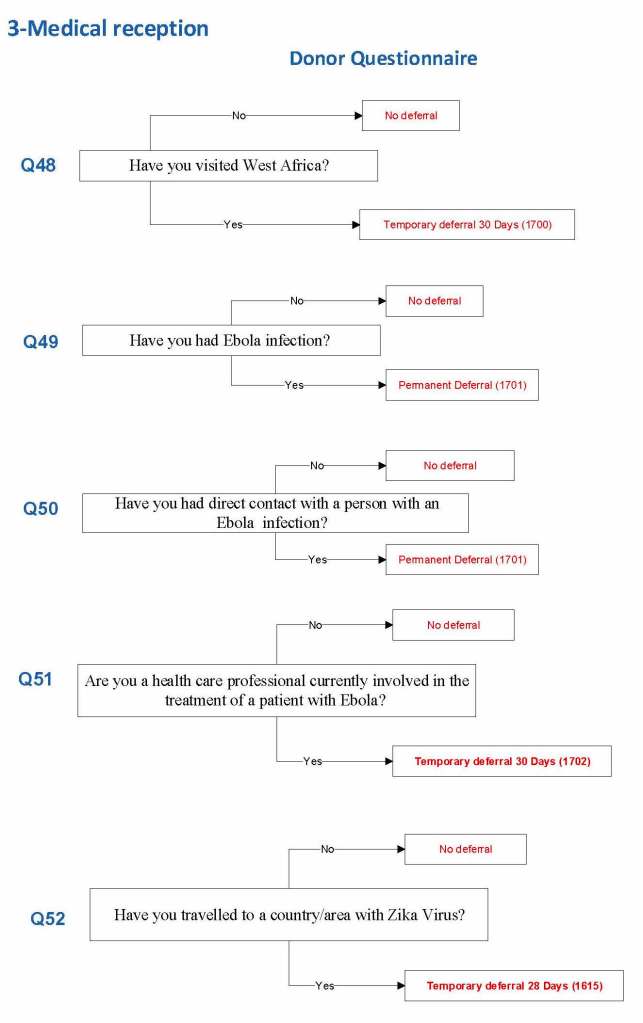
For each screening question, I prepared the exact wording (usually the UDQ’s) and set the deferral to temporary (how many days) or permanent.
Some questions were more open-ended, and the interviewer manually entered a medication, surgical procedure, etc. The transfusion physician would review this and assign a temporary (specifying the interval) or permanent deferral.
The questionnaire was constantly being updated by changes. My role was to review different accreditation systems (AABB, CE, etc.) and the World Health Organization’s websites. I would then prepare an interim policy and pass the specifications for the changes to the Medinfo software engineer and when ready, finally to the Super Users for testing. If there was an urgent change, the whole process could be completed in less than one day including validation testing.
The following shows examples of the software processes:
Medications
Body fluid exposures
Vaccinations
Malaria
Ebola/Zika
I emphasize that all of these settings are user-definable (at least in jurisdictions that permit all open, non-turnkey software).
Medication Questions:
Vaccinations:
Blood and Body Fluid Exposures:
Malaria Example: DMAL refers to the malaria antibody test.
Building the Software Processes for the Donor Collection 5:Donor Physical Examination and Adverse Reaction Reporting
Donor Physical Examination and Adverse Reactions
Donor physical examination, along with the donor questionnaire, are important both for donor and patient safety. In general:
Is it safe for the donor to donate?
Is it safe for the patient to receive the blood even if it is safe for the donor to donate.
Any donor who does not feel well must not donate. This may be the single most important step in ensuring a safe blood supply.
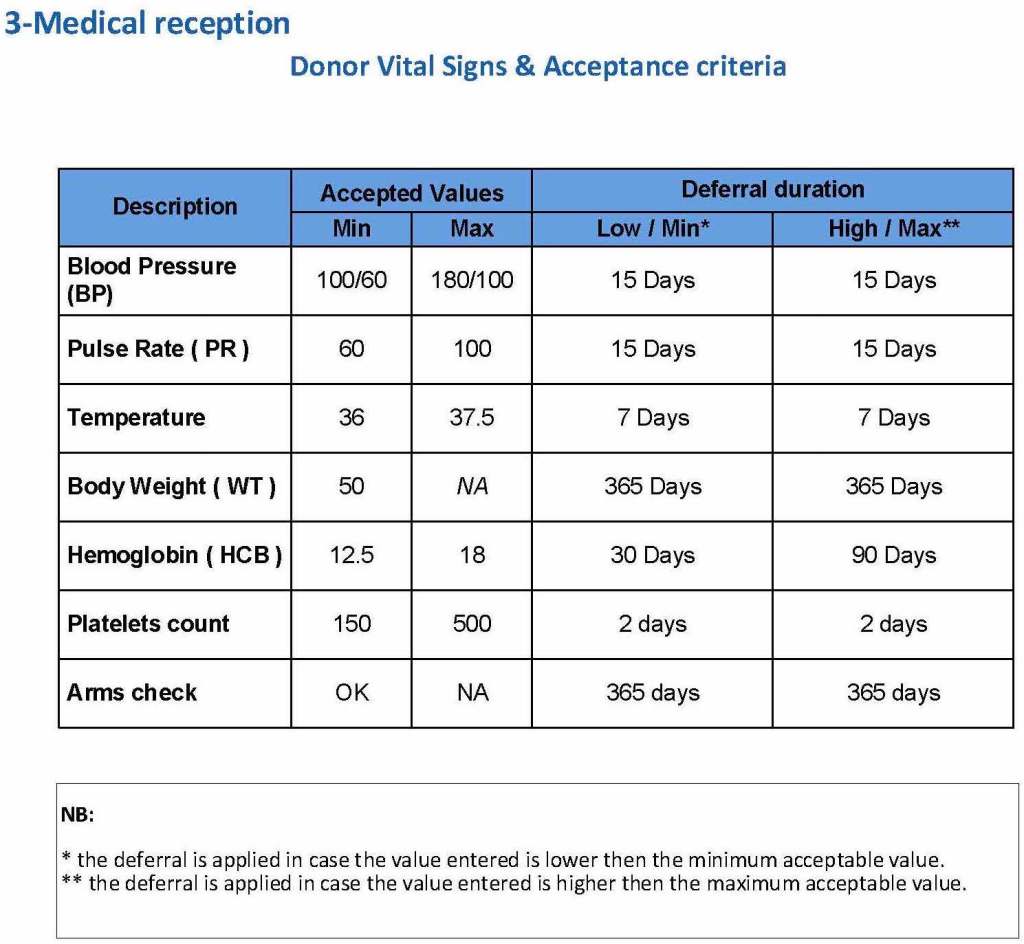
The donor physical examination includes the vital signs (blood pressure, pulse, temperature, heart rate, and temperature). I have attached a sample set of criteria for review. All are user-definable. Note how the arm examination is also included (looking for scarring, skin lesions, etc.)
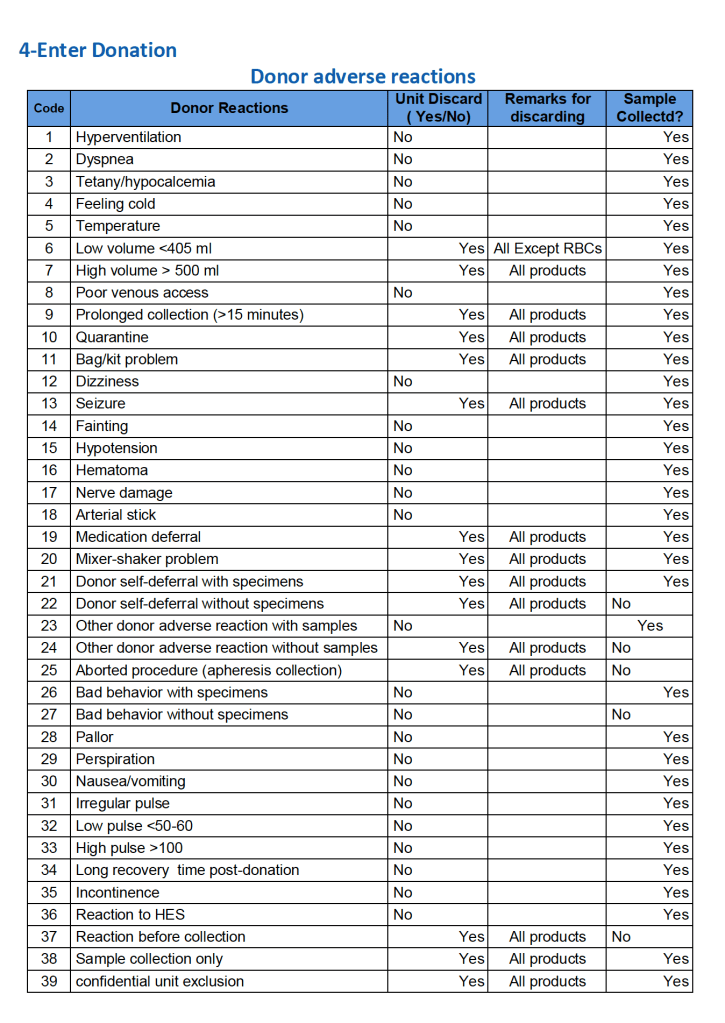
For all types of donations, there may be adverse reactions. These must be documented in the record along with the disposition of the donation. Will the donor need an extended deferral if the RBCs in the apheresis run are not returned? This can be built from the reaction documentation. Note the following sample table of reactions.
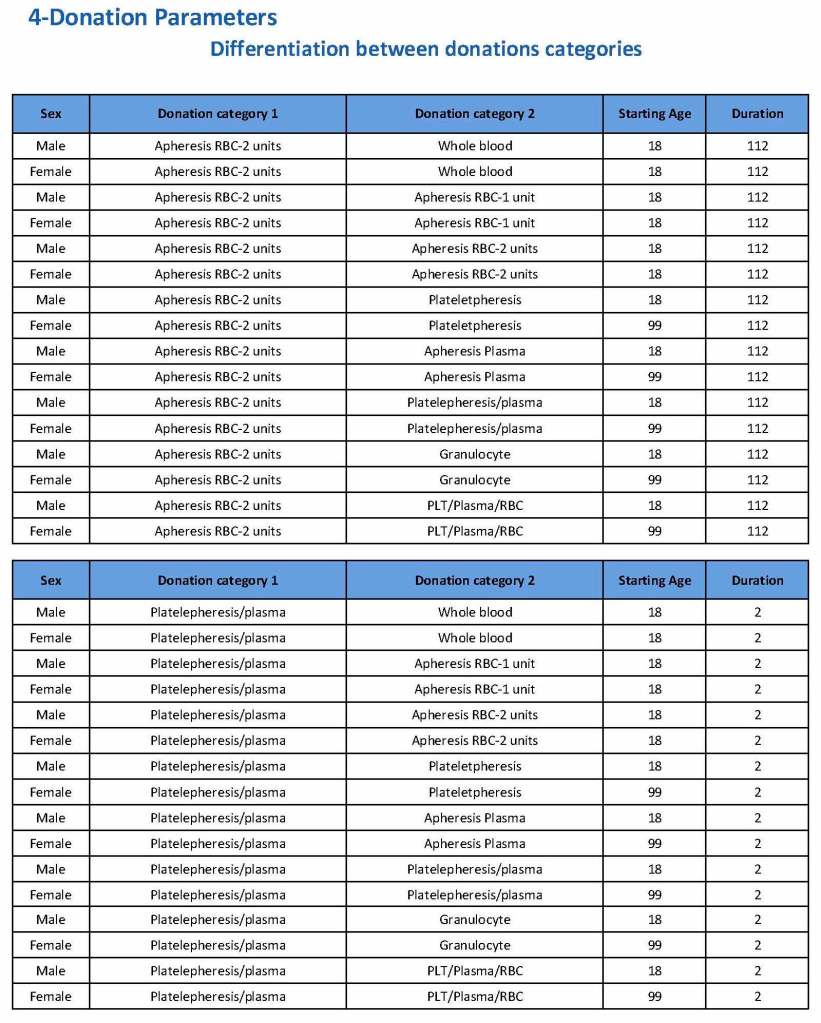
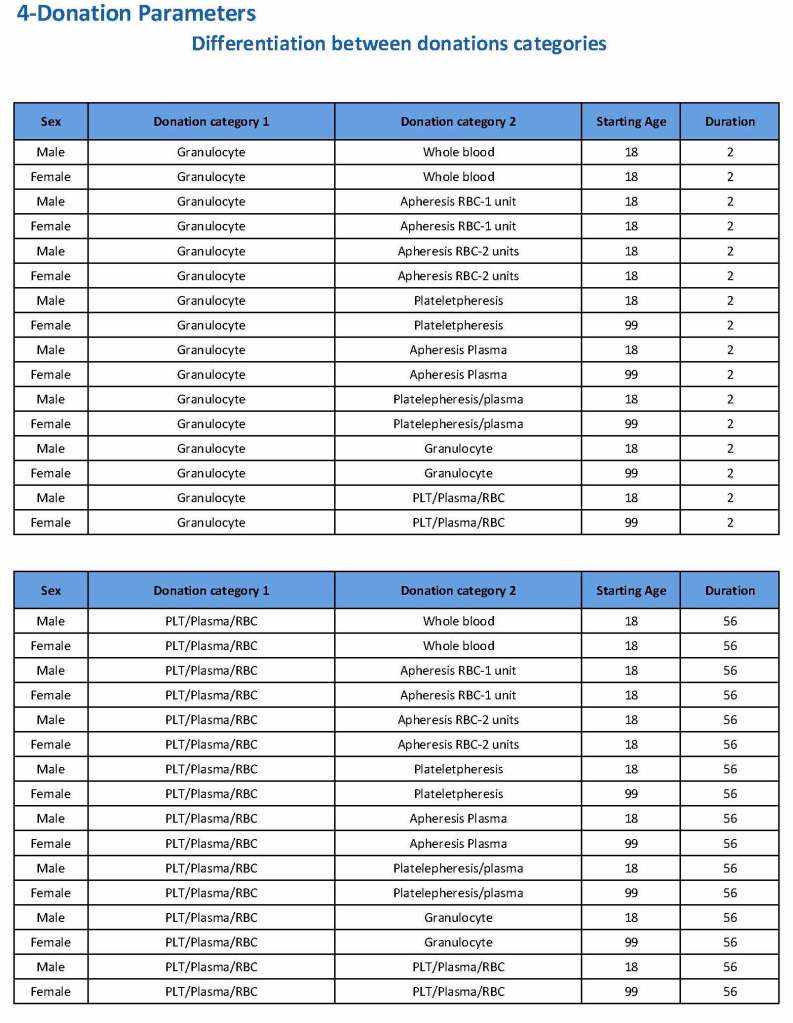
Donation can be whole blood or apheresis-based. The sex and age for each donation type is specified. At HMC, we did not accept females for platelet or plasma donations, so the starting age is listed as 99 years. Otherwise, in accordance with Qatari law, the starting age for donation is 18. All these parameters are user-definable, and a transfusion medicine physician can override the rules if necessary.
For each and every combination of donations, the deferral interval must be specified. Examples follow. The temporary deferral period is in days:
Previous donation whole blood, current donation whole blood: 56
Previous donor platelets, current donation whole blood: 2
Previous donation whole blood, current donation platelets: 56
Also note how for each possible combination there is an entry for male AND female. Females are restricted to whole blood donation and only RBCs will be made from the collection.
If there is a collection incident and the apheresis procedure is not completed, the interval will be set to 56 days. This will be covered in the post on donor adverse effect reporting.
Daratumumab is a monoclonal antibody that binds to CD38 antigen, which is expressed weakly on the surface of all RBCs. It may thus cause a positive direct antiglobulin test DAT and so interfere with compatibility testing if an antiglobulin phase is required.
This effect may persist up to 6 months after discontinuing the drug. The monoclonal antibody does not interfere with routine ABO/D typing.
Special techniques (neutralization of CD38 antibodies by CD38 anti-idiotypic antibodies, or soluble CD38 antigen) may remove the panreactivity but are not generally available. DTT, a sulfhydryl reagent may denature the native CD38 antigen on RBCs but it should be used under a biologic hood.
Kell antigens will be denatured so Kell antibodies cannot be detected after treatment so Kell-negative RBCs should be used. In the Gulf Area, this is about 72% of RBCs. In the Medinfo software a rule to require K-negative RBCs has been built.
Policy:
The clinical services must inform Transfusion Medicine of patients who will be receiving daratumumab therapy BEFORE treatment is started.
Transfusion Medicine staff will enter a general comment (i.e. not associated with a particular result) in the patients Medinfo HIIG record: PATIENT ON DARATUMUMAB.
If not already done, Transfusion Medicine staff will perform an extended antigen typing: at least C, c, E, e, K, k, Kpa, Jka, Jkb, Fya, Fyb ,M, N, S, s, Lea, Leb, P1—even if no antibodies are currently identified.
Transfusion Medicine staff will send each such patient’s record to a Transfusion Medicine Physician to determine the blood type including extended antigens to match for future transfusions.
When compatibility testing is requested, perform it as per our SOPs.
If available, prepare DTT-treated cells for testing but realize that this will denature Kell antigens. Use K-nell RBCs.
Medinfo has a rule to automatically require K-negative RBCs if this medication is used.
Release least “incompatible” RBCs must be approved by the Transfusion Medicine Physician.
When the DAT becomes negative (i.e. up to SIX months after cessation of Daratumumab therapy), routine compatibility testing and RBC selection will apply.
References:
Trick or Treatment, Anti-CD38 Reactivity and How to Treat It, AABB Satellite Symposium transcript, U. Cincinnati and RedMedEd, October, 2015 (attachment)
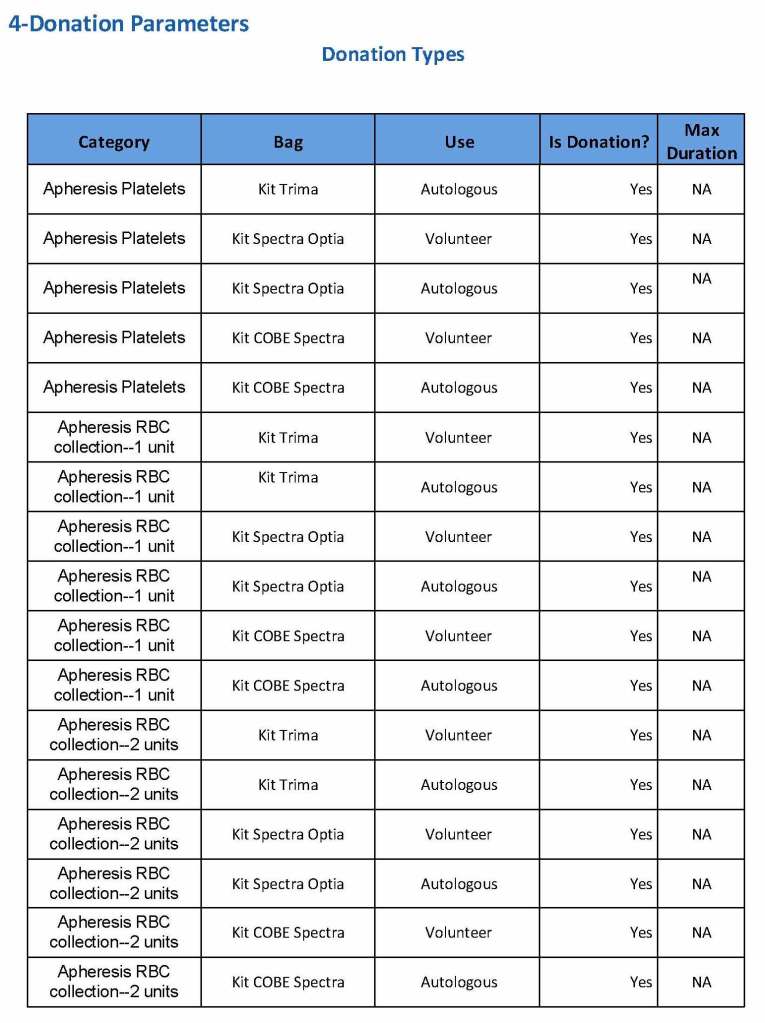
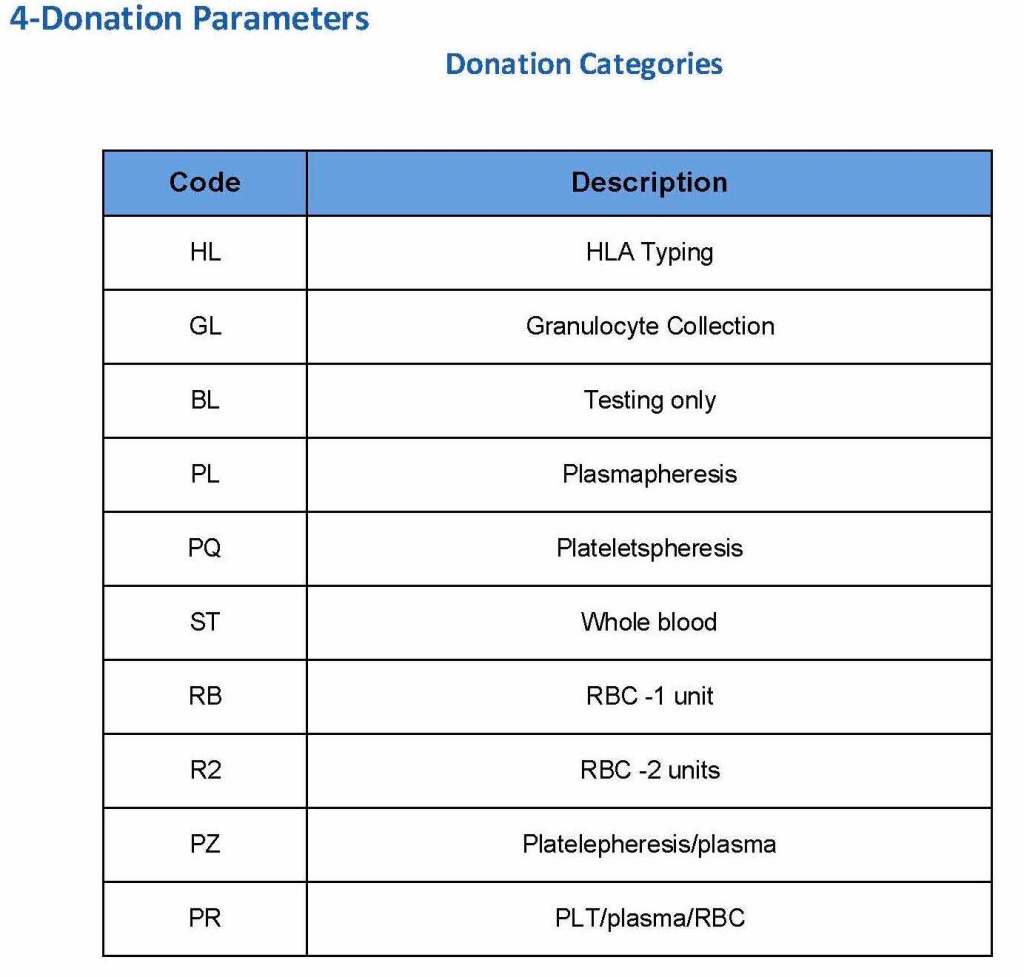
At the time of registration, the type of donation must be specified. In my last position, this could include whole blood for automated Reveos, whole blood for cryoprecipitate, plasmapheresis, COVID 19 convalescent plasmapheresis, plateletpheresis, concurrent platelet and plasmapheresis, concurrent platelet, plasma, and RBC apheresis, RBC apheresis-one unit, and RBC apheresis-2 units.
There is also a specimen-only donation without actual collection that includes database check, assignment of an ISBT specimen number, donor questionnaire, physical examination, and specimen collection only..
We specified which bag or kit could be used for each type of donation so when it was selected, only that bag type would be accepted by Medinfo
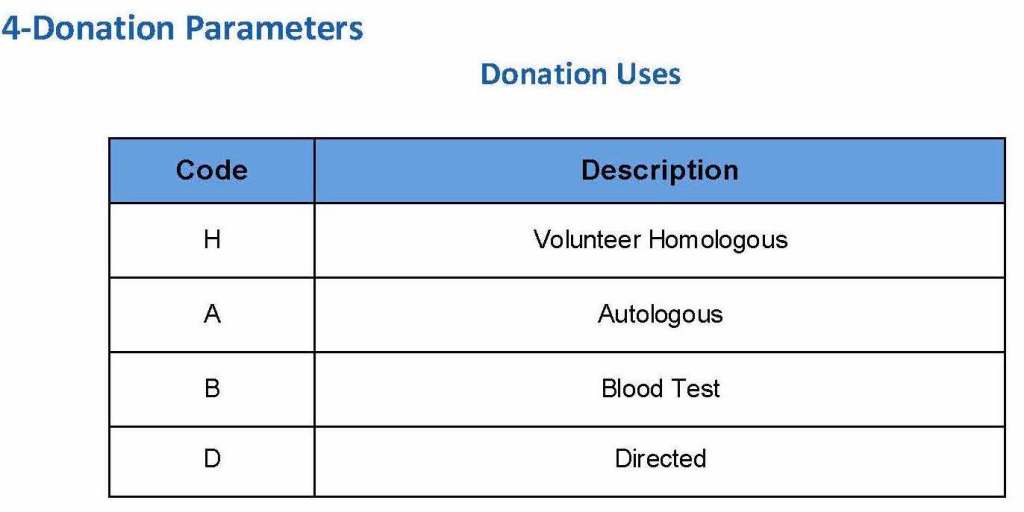
For each of these types we must specify what type of donation is permitted: volunteer, autologous, or directed.
Finally, we must indicate the maximum length of the procedure permitted. This applied to whole blood only and we set this at 15 minutes—this is user definable.
The following are a sample set of parameter settings for the above:
Note how we included contingencies for old bag sets and equipment (that we later discontinued) and for granulocyte collection (which we did not actually perform).
This policy outlines steps taken to minimize the risk of data entry errors and is based on a dualistic approach: review of results by a senior technologist and/or supervisor and various computer safeguards built into the Medinfo Hematos IIG blood bank computer HIIG system. This policy also discusses the verification (here called authorization) and purge processes of HIIG.
Policy:
Review by senior technical, supervisory, or transfusion medical staff:
Designated test procedures require review by a second technologist before authorization.
Complex immunohematology testing and specimens showing aberrant results (e.g. ABO/D discrepancies) are reviewed by the supervisors or designates and ultimately a transfusion medicine physician before authorization.
Computer system HIIG rules:
Privileges:
System restricts which staff can perform specific tests
Patient/donor identity:
System asks end-users to verify patient/donor identity before starting any access to the patient/donor record.
System performs historical database checking and flags any inconsistencies (e.g. historical ABO/D typing differences, etc.)
Testing:
Only selected staff have privileges to authorize or purge.
ABO/D testing algorithms require entry of reactions, not interpretation of results and are compared to a truth table.
Aberrant results require special review before ABO/D typing results can be authorized/purged.
D-controls must be negative to allow D typing results to be authorized for liquid D-typing reagents.
DAT results require appropriate controls to meet truth-table criteria.
Eluates require last wash to be negative before authorization
Blood components:
Selection of RBC or plasma units requires two independent sample determinations within 72 hours of each other.
ABO-incompatible RBC or FFP/FP24 transfusions are not allowed.
Donors with any detectable antibodies are permanently deferred.
Depending on the patient’s antibody history, release of RBC units may require antigen-matched units. Examples:
Mandatory matching (only antigen negative matched units allowed—no antigen positive or antigen-untyped units): Antibodies against H, D, c, K, k, Kpa, Kpb, Jsa, Jsb, Jka, Jkb antigens, anti-PP1Pk
Priority matching (incompatible or untested can be approved by a transfusion medicine physician): C,E, e, Fya, Fyb, M, S, s
Antigen matching not required: Lea, Leb, N
Least-incompatible crossmatch require special authorization to release
Protocols to force irradiation or other modified components can be setup in HIIG.
Donors:
Donor tests have same criteria as the same test used in patient testing for controls, etc.
Donor demographics are read directly from the Ministry of Interior database—no manual entry (bar code only used).
References:
Workflows for Hematos IIG (1001 through 1005), 2013
Standards for Blood Banks and Transfusion Services, Current Edition, AABB, Bethesda, MD, USA
Guidelines to the Preparation, Use, and Quality Assurance of Blood Components, European Committee (Partial Agreement) on Blood Transfusion (CD-P-TS), Current Edition
Building the Software Processes for the Donor Center 2:
Donor Collection and Screening—Registration and Pre-Donation Parameters
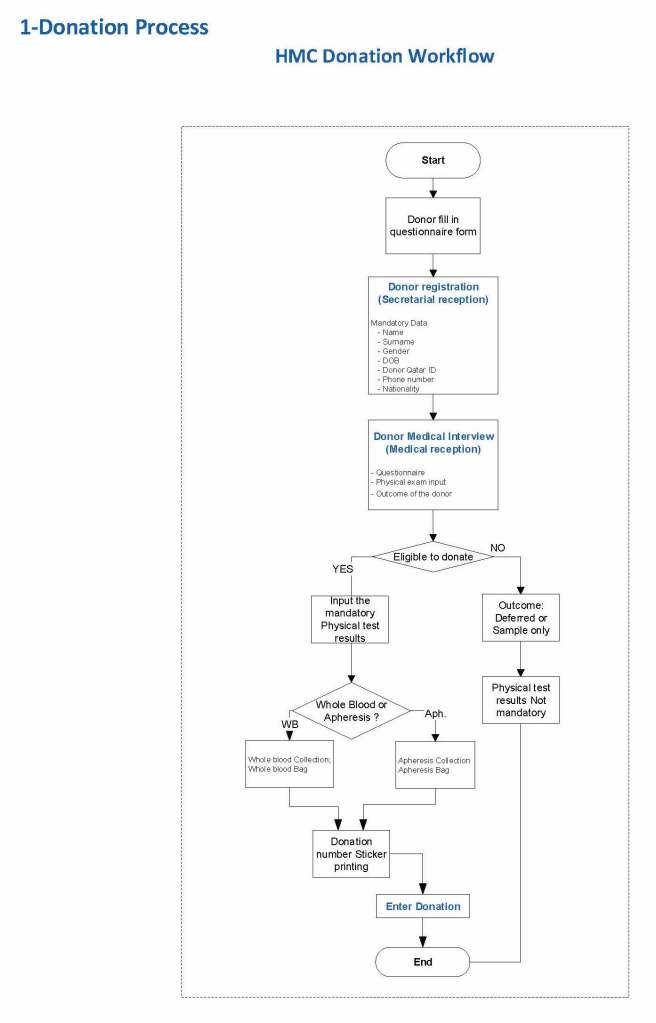
The potential donor enters the collection area. He takes a number and waits to be called. When called, he shows a picture identification card with a unique alphanumeric sequence. This is entered into the donor module software and the system checks the donor deferral database for temporary and/or permanent contraindications. If none are found, a consent form with an ISBT specimen number is generated.
In this post, we will consider:
Registration process in multiple languages
Donor deferral database
Donor consent with generated unique ISBT specimen number
Registration Parameters
Registration:
In the Middle Eastern region, multiple languages are used. Although Arabic may be the main language, not all the registration staff may speak it. English is commonly used as the main work language. The date may be entered as Common Era (Gregorian) and/or Hijri.
An issue is that for native Arabs, the only precise, unambiguous name spelling is in Arabic. English transliterations vary. Example, Muhammad in Arabic is very simple to write, in English it may be rendered as Mohamed, Mohammed, Muhammad, etc. The donor’s name should be recorded exactly as in his native alphabet. How do you register when the staff do not speak or type Arabic?
Fortunately, I have worked with software that is in UNICODE, meaning that the data does not have to be restricted to English or Latin script (I wonder why the hospital information system we had at one institution could be sold in the Middle East and not have this capability!). That means one could perform registration and donor questionnaire tasks in multiple languages, and preferable the native language of the donor. One could even prepare database reports in Arabic.
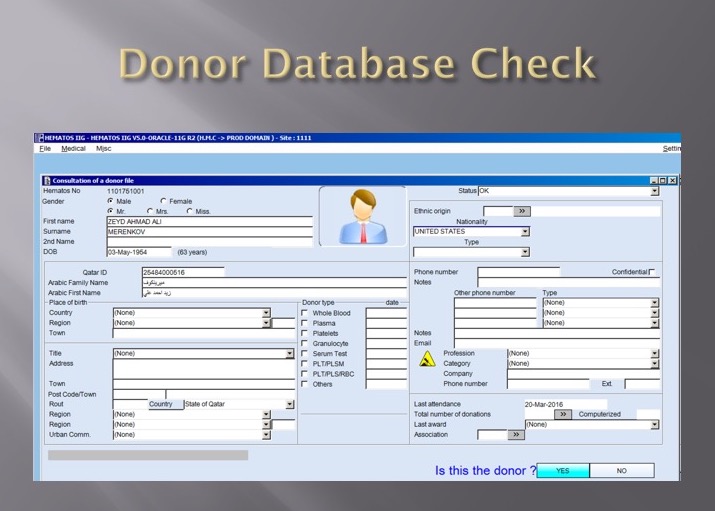
Medinfo had an elegant solution to the registration process in Qatar. It read the local identity card’s barcode issued by the Ministry of Interior and accessed (read-only) the demographic data on that donor and received back both the English and Arabic name fields:
This would generate the demographic fields in the registration:
The blood bank software would check the national donor deferral database and list any deferrals/contraindications to donation and the next eligibility date. It would also list what type of donations were permitted (e.g. for females, only RBCs could be collected and processed: if a whole blood unit was collected, then the platelets and plasma would NOT be permitted to be processed and were discarded.)
Medinfo used a unique key field, the Medinfo Hematos Donor ID for the database. This was not the same as the national ID card. All records were indexed against this number with strong security.
Donor Deferral Database:
Medinfo had already imported donor data from a previous computer system and added this to its own database. Thus, there was only one database to check. The database listed all previous donations: dates, type, status (complete, aborted). Any contraindications would be prominently shown in RED.
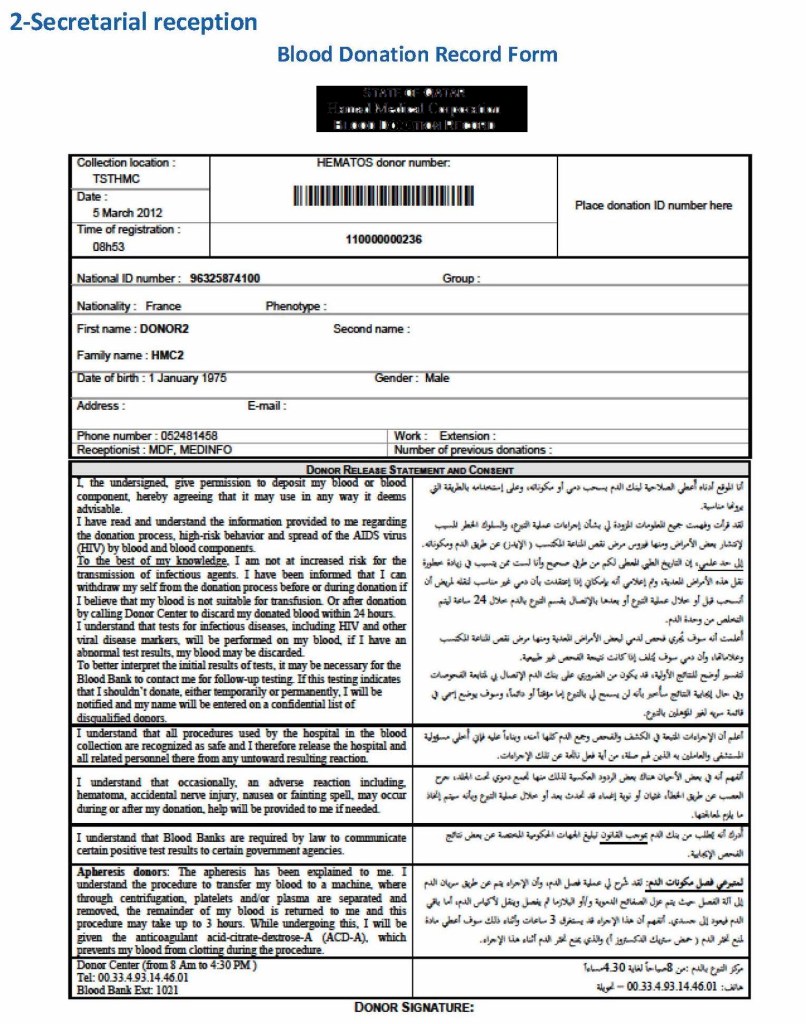
Donor Consent and Assignment of Donor Unit (ISBT Specimen) Number:
If there were no contraindications, Medinfo generated a donor consent in English and Arabic and the unique donor unit number for the current encounter:
Registration Parameters:
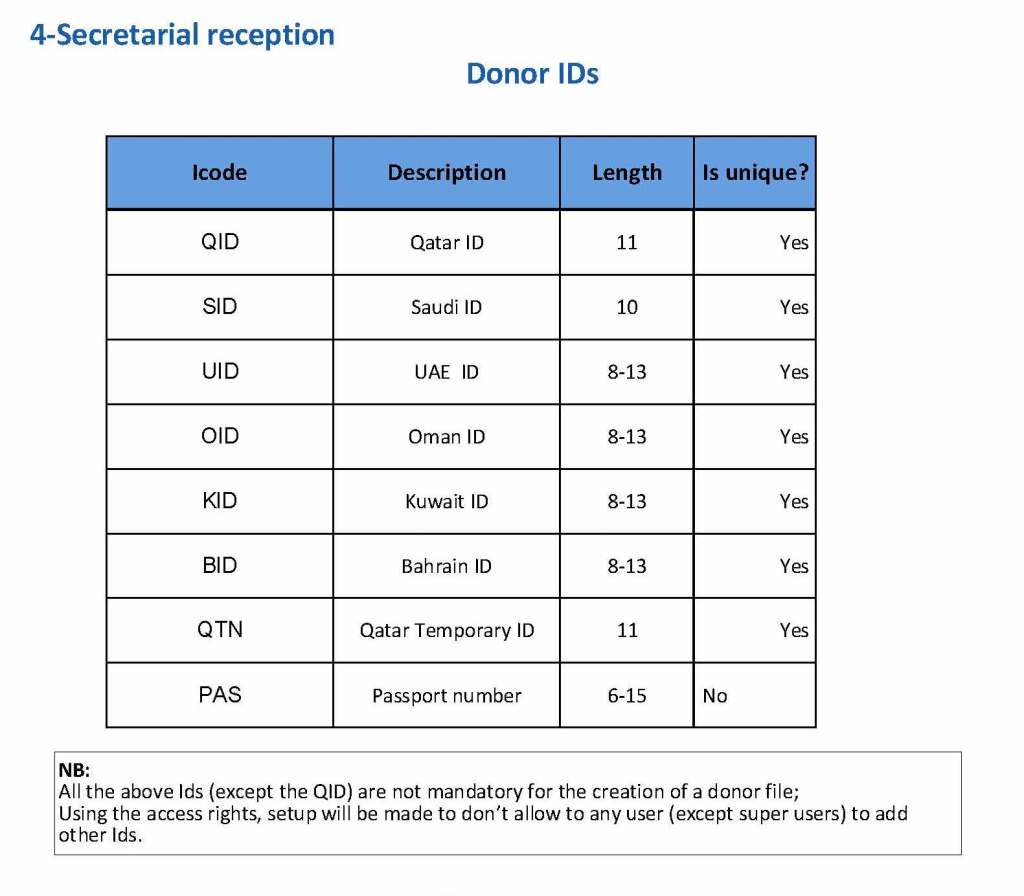
Medinfo enforced registration according to the format of the identity card. The donor ID format was built into Medinfo. If the entry deviated from this, it was rejected and registration could not continue:
The registration type would be selected (volunteer, autologous, directed, or paid). In Qatar, paid donations were not permitted:
Next, the donation type had to be selected:
At the time of registration, the type of collection bag (or kit if using Reveos) was automatically set in Medinfo. I will consider this further in the next post of this series to determine eligibility based on the previous donation interval and type.
At each donation site, the allowable types of donations and kits could be set. Based on the donation parameters above, staff could not select the wrong type of bag/kit (e.g. an apheresis kit for a mobile donation).
If there is strong antibody binding to an RBC, this may interfere with a typing reagent attaching to the cell and cause a false-negative, i.e. a “blocking” antibody. Such cells may interfere with the indirect antiglobulin test IAT, i.e. the antibody screen. The autocontrol and direct antiglobulin test DAT will be strongly positive.
The manufacturer’s instructions should be strictly followed for using its reagents in the presence of a strongly positive DAT. If there is no reaction with the typing reagent, the result must be indeterminate.
One could try a (relatively) nondestructive elution method such as gentle-heat elution to remove some of the antibody and then retype the cells. I have found this to be a simple and effective method for my staff to use. Just remember that despite being “gentle,” there will still be some hemolysis present, but here it is the cells we are trying to save.
Usually, we find this situation in a neonate born of a mother with anti-D. The baby has a strong DAT but the D typing is negative. Check the D control carefully: if it is positive, the result is indeterminate, try another method. Usually gel/glass bead methods are subject to less interference. Finally, there is always the classic saline anti-D!
In Medinfo software with a blocking antibody, a nonnegative control will trigger a manual review of the results. There will be no automatic release.
Here is my process for handling blocking antibodies, which I set up for HMC Doha:
INTERIM POLICY: ANTIGEN TYPINGS IN PRESENCE OF STRONGLY POSITIVE DIRECT ANTIGLOBULIN TEST (DAT): RULE OUT BLOCKING ANTIBODY
Principle:
Antigen typing of cells with large amounts of coating antibody (i.e. strongly positive DAT 3-4+) may not always be possible because the bound antibody may block available antigen sites. This policy is to clarify how to recognize and handle such situations.
Policy:
Always follow the manufacturer’s instructions for the use of the typing reagent.
In particular, note whether a control must be run with the test (e.g. D-control, D-diluent, etc.) or if it is included in the gel or glass bead card.
If a control is required, use exactly what the manufacturer recommends.
DO NOT SUBSTITUTE ANYTHING ELSE AS THE CONTROL!!
Interpret the reactions exactly as the manufacturer indicates.
If the test is invalid because of the control or any other reason, report the antigen typing as indeterminate and send for Transfusion Medicine Physician review.
If the DAT is 3-4+ and the antigen typing shows no reaction (apparent negative), send the case to the Transfusion Medicine Physician for review and final interpretation. DO NOT ENTER THE RESULT AS NEGATIVE UNLESS THE TMP INSTRUCTS YOU TO DO THIS!!
To rule out a blocking antibody, a special elution to gently remove the coating antibody may be needed so that the RBCs can then be typed (not acid glycine technique—rather, gentle heat elution.) The Transfusion Medicine Physician will decide whether to do this additional testing.
References:
Standards for Blood Banks and Transfusion Services, Current Edition, AABB, Bethesda, MD, USA
Technical Manual, Current Edition, AABB, Bethesda, MD, USA
Guidelines to the Preparation, Use, and Quality Assurance of Blood Components, European Committee (Partial Agreement) on Blood Transfusion (CD-P-TS), Current Edition
This is a first is a series of detailed posts of how I collaborated with Medinfo (Nice, France) to build customized donor software for both Saudi National Guard Health Services and Hamad Medical Corporation Doha.
In particular, we were using a non-turnkey software which could be built to order. If we didn’t know what we were currently doing, how could we build something better?
At both sites, we had good manual systems in effect and prepared detailed mapping of the current state. We reviewed our variance reports to see where we needed to bolster the system and improve the critical control points.
We studied the software options and prepared a draft Medinfo future state from which we started to build the system. We did this in small stages so we could test it and adjust our settings as needed—without being charged extra (unlike a general laboratory software I had been working with at the same time, which always charged an arm and a leg).
To do this, I engaged early a team of my most computer-literate staff to work as Super Users. In the Donor Center, this consisted of nurses and technologists.